w w w . r b o . o r g . b r
Original
Article
Use
of
risedronate
for
consolidation
and
callus
formation
in
Colles
fractures
in
postmenopausal
women:
SOLID
study
Lindomar
Guimarães
Oliveira
a,∗,
Sérgio
Ragi
Eis
b,†,
Henrique
Mota
Neto
c,
Frederico
Barra
de
Moraes
d,
Luiz
Antônio
Silveira
Simões
Pires
e,
José
Wanderley
Vasconcelos
faClínicadeOrtopediaeFraturas,Goiânia,GO,Brazil
bClínicadeDiagnósticoePesquisadaOsteoporosedoEspíritoSanto,Vitória,ES,Brazil cUniversidadeEstadualdoCeará,Fortaleza,CE,Brazil
dSchoolofMedicine,UniversidadeFederaldeGoiás,Goiânia,GO,Brazil
eOrthopedicsandTraumatologyService,HospitalSãoLucas,PontifíciaUniversidadeCatólica,PortoAlegre,RS,Brazil fCentrodePesquisaSOSTrauma,SãoLuiz,MA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received3June2014 Accepted25June2014 Availableonline17April2015
Keywords:
Fractureconsolidation Collesfracture Bisphosphonates
a
b
s
t
r
a
c
t
Objective:Thisopen,randomizedandblindedparallel-groupmulticenterstudyevaluated theefficacyofActonel®(35mg)pluscalcium/vitaminDversuscalcium/vitaminDalonefor preservingbonemineraldensity(BMD)inpostmenopausalwomenwithCollesfractures.
Methods:PatientswithaCollesfractureforsevendayswererandomizedtoreceiveeither Actonel®(35mg)onceaweekpluscalcium/vitaminD(ACDgroup)orcalcium/vitaminD alone(CDgroup).Thepatientswereevaluatedafter90and180daysoftreatment.
Results:59ACDpatientsand56CDpatientscompletedalltheevaluations.Attheendofthe study,theBMDoftheradiusatthefracturelocationshowedanegativechangeintheCD group(32.8%).ThelossofBMDintheACDgroup(20.8%)wasslightlylessthanthatintheCD group.TherewasadifferenceintheproportionsofpatientswithBMDlossesattheendof thestudyperiodinthetwotreatmentgroups,infavoroftheACDgroup,althoughthiswas notstatisticallysignificant.Therewasnosignificantdifferenceinradiologicalidentification ofcallusformationbetweenthetreatmentgroups.Inthemajorityofthepatients,thecallus couldberadiologicallyidentifiedafter90days.
Conclusion:PostmenopausalwomenwithCollesfractureswhoreceivedrisedronatesodium pluscalcium/vitaminDdidnot showanysignificant differenceinBMDlossinforearm
∗ Correspondingauthor.
E-mail:[email protected](L.G.Oliveira).
† Inmemoriam.
http://dx.doi.org/10.1016/j.rboe.2015.04.004
fractures,incomparisonwiththosewhoreceivedcalcium/vitaminDalone.Risedronate aprotectiveeffectregardingBMDlossduetoimmobilization.Thetimetakenforfracture consolidationtobeachievedwasunaffected.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Uso
de
risedronato
na
consolidac¸ão
e
formac¸ão
do
calo
na
fratura
de
Colles
em
mulheres
na
pós-menopausa
–
Estudo
Solid
Palavras-chave:
Consolidac¸ãodafratura FraturadeColles Difosfonatos
r
e
s
u
m
o
Objetivo: Esteestudomulticêntrico,randomizado,aberto,grupoparaleloavalioua eficá-ciadeActonel® 35mgmaiscálcio/vitaminaDversuscálcio/vitaminaDisoladamentena preservac¸ão da densidade mineral óssea(DMO) em mulheres pós-menopausadas com fraturadeColles.
Métodos: PacientescomfraturadeCollesemsetediasforamaleatoriamentedesignadas parareceberActonel®35mgsemanalmentemaiscálcio/vitaminaD(GrupoAO[GAO])ou cálcio/vitaminaD(grupoO[GO])isoladamente.Aspacientesforamavaliadasapós90e180 diasdetratamento.
Resultados: Completaramasavaliac¸ões59pacientesnoGAOe56noOG.Nofimdoestudo,a DMOdorádionolocaldafraturamostrouvariac¸ãonegativanoGO(32,8%)quefoi discreta-mentemenornoGAO(20,8%),assimcomoumaperdamenornaDMOnoGAOcomparado comoOG.Houvediferenc¸anaproporc¸ãodepacientecomperdadaDMOnofimdoestudo nosdoisgruposdetratamentoemfavordoGAO,apesardenãoestatisticamente signifi-cante.Nãohouvediferenc¸asignificativanaidentificac¸ãoradiológicadaformac¸ãodocalo entreosgruposdetratamento.Namaioriadaspacientesaidentificac¸ãoradiológicadocalo ocorreudepoisde90dias.
Conclusão: Mulherespós-menopausadascomfraturadeCollesquereceberamrisedronato sódico, além docálcio/vitamina D, comparado comcálcio/vitamina Dnão mostraram diferenc¸asignificativanaperdadaDMOnafraturadoantebrac¸o,comtendênciadeefeito protetordorisedronatonaperdadaDMOdevidoàimobilizac¸ão.Otempoatéaconsolidac¸ão dafraturanãofoiafetado.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
The potential for accelerating or improving the formation ofacallusandpreventingprogressionoffracturesto pseu-darthrosishasbeen correlatedwithmechanicalprocedures for stabilizing bone fragments. However, this reality has changesinthelightoftheprovenefficacyofphysicalmethods ormedications.1
Bisphosphonateshavebeen studiedregardingtheir pos-sible positive or negative influence on formation of bone calluses.Thisgivesrisetoquestionsthatrelatetohow bis-phosphonatesmightinterferewithboneconsolidation;what theirinfluenceonthehistology,morphologyand biomechan-icsofthecallusmightbe;whatthebesttimeafterthefracture forstartingmedicationwouldbe;whetherbisphosphonates mighthaveanyeffectonconsolidationamongpatientswho usedthem previously, beforethe fracture;and whether all typesofbisphosphonatesactinthesamemannerwithregard toformationofthebonecallus.2–4
At therapeutic doses for osteoporosis, different
bis-phosphonates have not shown negative effects on bone
consolidationbuthaveshownimprovementstothe biome-chanical aspects of bone.5–9 Experimental studies using risedronate haveshown thatconsolidation occurs,without anychangetothetimetaken,butwithbonecallusofbetter histologicalquality.10,11
Materials
and
methods
Studydesign
Thiswasacomparativeparallel-groupopenrandomized mul-ticenter phase IV study conducted in six study centers in Brazil:Goiânia(one),Fortaleza(one),Niterói(one),SãoLuísdo Maranhão(one)andSãoPaulo(two).Thestudywasapproved bytheappropriateethicscommitteesandthepatientsgave theirfreeand informedconsentinwriting,beforeany pro-ceduresrelatingtothestudywerestarted.Furthermore,the studywasconductedinaccordancewithgoodclinical prac-ticesandwiththeethicalprinciplesthatoriginatedfromthe DeclarationofHelsinki.
Eachpatientwasevaluatedovera180-dayperiod,through sevenevaluationvisits:VO(baseline):visitmadesevendays afterColles fracture occurred;VR,randomizationvisit (day 0),madesevendaysafterthebaseline;andsubsequent vis-itsmade15(V1),30(V2),45(V3),90(V4)and180(V5)daysafter therandomizationdate.Amongthevisits,anintervalofthree dayswasallowed.
Patients
Womenwhohadbeenpostmenopausalforatleasttwoyears wereeligibletoparticipateiftheypresentedaCollesfracture thatwasconfirmedwithinaperiodofsevendaysbeforeentry intothestudy.Thepatientswerestratifiedbyageina1:1ratio (<65and≥65years)andaccordingtoT-score≤−2.0standard deviationsinthelumbarspine(L1–L4 and/orL2–L4)and/or femoralneckand/ortotalfemurand/or33%radius.
Themaininclusionandexclusioncriteriawereasfollows:
Inclusion criteria: postmenopausalfor atleast two years; Collesfractureconfirmedwithoccurrencesevendaysbefore entryintothestudy;T-score≤−2.0standarddeviationsinthe lumbarspine(L1–L4and/orL2–L4)and/orfemoralneckand/or totalfemurand/or33%radius.
Exclusioncriteria:previousfractureinthesamewristor fore-arm;fracturethat,intheopinionoftheorthopedicsurgeon or person responsible for the case, shouldonly be treated surgically;distalfractureoftheradiusorfracturesin contralat-eralbonesthatoccurredpreviouslyorconcomitantly,which mightimpedecomparisonsoftheBMDevaluationsoverthe courseofthestudy;use ofmedicationsconcomitantlythat mightaffectthecalciummetabolism;previoustreatmentwith bisphosphonatesformorethan 12monthsoverthe last36 months;useofbisphosphonatesforanyperiodoftimeover thelastthreemonths;cumulativeuseofbisphosphonatesfor morethan 36monthson any occasion;rheumatoid arthri-tisoranyotherdiseasewithinvolvementofthewrist;hyper orhypothyroidismthatisknowntobestable,withor with-outtreatment;hypocalcemia,liverdisease,kidneydiseaseor rheumaticdiseases.
Studytreatments
At the randomization visit, the eligible patients were designated to receive one of the two study treatments: Actonel®+Oscal®group(GAO):35mgofsodiumrisedronate
onceaweekplus1000mgofcalciumand400IUofvitaminD onsixdaysaweek(i.e.notonthedayonwhichrisedronate wouldbetaken);orOscal®group(GO):1000mgofcalciumand 400IUofvitaminDdaily(i.e.sevendaysaweek).
Efficacyassessments
Efficacywas based onthe changes seeninthe T scoresin theproximalregionoftheforearm(33%oftheregionofthe radius),fromthebaselinetoV4(90days)andV5(180days) afterthetreatmentandwasexpressedaspercentagesforthe twoarmsfracturedandnon-fractured).
Thedifferencewascalculatedinthefollowingmanner:T
scoreatV4minusTscoreatbaseline,dividedbyTscoreat baseline.
ThesamecalculationwasusedforthechangeinTscore fromthebaselinetoV5(180days);themeanchangeinTscore intheproximalforearm(33%oftheregionoftheradius)from thebaselinetoV4andV5inthetwoarms(fracturedand non-fractured),withradiologicalidentificationofcallusformation bymeansofX-rays.
Bonemineraldensity(BMD):BMDwasmeasuredbymeans ofdual-energyX-rayabsorptiometry(DXA),usingaGE/Lunar densitometer(DPXIQ,DPXNT,MD+Prodigy)orHologic densit-ometer(QDR2000,QDR200+,QDR4500,DelphiorDiscovery) onthelumbarspineandproximalfemur(femoralneckand totalhip)andthedistalregionoftheforearm(fracturedand non-fractured),atthebaselineandthenat90and180days. TheBMDmeasurementswererepeatedusingDXAforthe dis-talregionoftheforearm(fracturedandcontralateral).
X-rays:Radiologicalimagesofthewristandarm(fractured andcontralateral)wereobtainedintwoviews(posteroanterior andlateral),atthebaselineand15,30,45and180daysafter thefracture.ThemainX-rayparametersformonitoringthe consolidationofthefracturewereformationandviewingof bonebridgesalongthefracturelines,identifiedinthecortexin eachview.Fractureconsolidationwasdefinedasthepresence ofbonebridgesinthreeofthefourcorticalimagesevaluated intheseviews.
Qualitycontrolprocedureswereestablishedbymeansof training andcertification ofthe teaminvolvedinusingthe densitometryandX-rayequipment,withcentralanalysisof the tests performed, performed by the coordinator of the OsteoporosisResearchand DiagnosisCenter(CEDOES).The examinerswereblindedwithregardtothestudytreatment administeredineachcase.
Safetyassessments
Safetywasassessedaccordingtothetypeandseverityofthe adverseeventsthatwerereportedbythepatientsorobserved insomeotherwaybytheinvestigator.
Definitionofthestudypopulation
(PP)consistedofpatientswhoweretreatedwithoutsignificant violationsoftheprotocolwhohadatleastoneBMDevaluation intheproximalregionoftheforearm(33%oftheregionofthe radius)onthesideofthefracture,atthebaselineandatV4 (90days).
Statisticalplan
AllthetestsappliedwereperformedusingSASv9.1andthe statisticalsignificancelevelwastakentobe5%.
Calculations were based on comparison of the groups
regardingthe mean change inBMD after90 days of treat-ment,expressedasapercentage.Powerof80%,significance levelof5%and discontinuationrateof10%were used.The standarddeviationwasassumedtobe0.08,withadifference ofinterestof4%betweenthegroups(meanpercentagechange inBMDafter90daysoftreatment).Therefore,theestimated totalnumbertoberecruitedwas140patients(70pergroup).
Thepercentagechange(%)inBMDafter90days(V4)and 180daysoftreatmentwascalculatedinthefollowingmanner:
– %changeatV4=[(T-scoreV4−T-scoreV0)/|T-scoreV0|]*100 – %changeatV5=[(T-scoreV5−T-scoreV0)/|T-scoreV0|]*100
The demographic variables of continuous nature were
described separately for the two treatment groups using
means, standard deviations and ranges. Comparisons
betweenthetreatmentgroupswereindicatedusingStudent’s
ttestvalues.Thediscretedemographicvariableswere sum-marizedin frequencytablesand comparisonsbetweenthe treatmentgroupswerebasedonpvaluesfromthechi-square testorFishertest,dependingonthefrequencyoftheevents.
The Mann–Whitney U test (independent observations)
was appliedforcomparisonbetweenthe treatmentgroups regardingchangesinT-scores(%)fromthevisitV0tothevisit V4andfromthevisitV0tothevisitV5.
TheWilcoxonsignedranktest(dependentobservations) was applied to compare the visits (V4 and V5) regarding changesinT-score(%),ineachtreatmentgroup.Tocompare thetreatmentgroupsbetweenthevisitsregardingmean T -scores,amodelofanalysisofvariance(ANOVA)wasapplied, withthefactorsfromthetreatmentgroups(Actonel+Oscal andOscal),visits(V0,V4andV5)andtherespective interac-tionsbetweenthem.Tocomparethetreatmentgroupswith regard to radiological identification of the callus, the chi-square test or Fisher F test was applied, according to the frequencyoftheevents.
Results
Patients
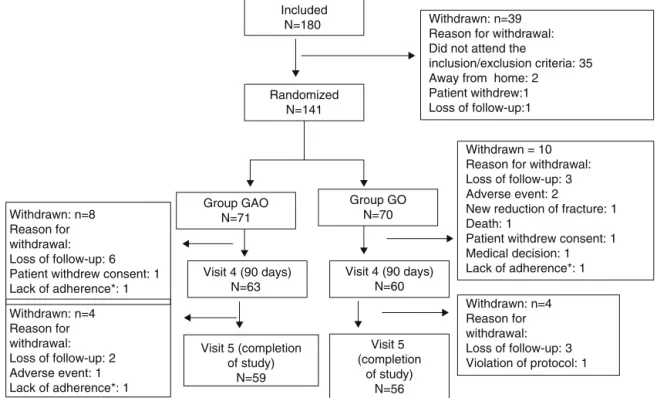
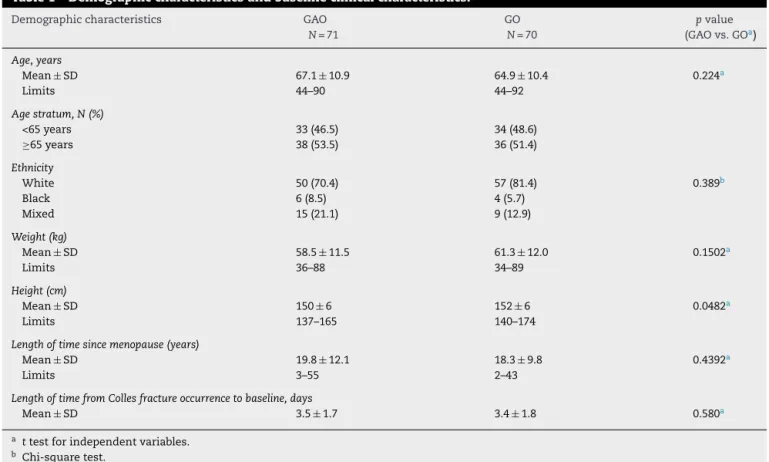
Thepatients’distributionispresentedinFig.1.Attheendof the study,59 patientsinGAOand56 inGOhad completed all the evaluations as planned.A total of 137 patients (70 in GAO and 67 in GO) received at leastone dose ofstudy medicationandwereevaluatedregardingefficacyandsafety. Thegroupswere showntobehomogenous atthebaseline regardingdemographicandclinicalcharacteristics(Table1).
Therewerenostatisticallysignificantdifferencesbetween the groups in relation to the side on which the fracture occurred:36/71patients(50.7%)hadaCollesfractureinthe left forearm inGAOand 38/70(54.3%)inGO (p=0.670).For the majority ofthe patients, the universal classificationof
Randomized N=141
Withdrawn: n=39 Reason for withdrawal: Did not attend the
inclusion/exclusion criteria: 35 Away from home: 2
Patient withdrew:1 Loss of follow-up:1
Group GAO N=71
Group GO N=70
Visit 4 (90 days) N=63
Visit 4 (90 days) N=60
Withdrawn = 10 Reason for withdrawal: Loss of follow-up: 3 Adverse event: 2
New reduction of fracture: 1 Death: 1
Patient withdrew consent: 1 Medical decision: 1 Lack of adherence*: 1 Withdrawn: n=8
Reason for withdrawal: Loss of follow-up: 6 Patient withdrew consent: 1 Lack of adherence*: 1
Withdrawn: n=4 Reason for withdrawal: Loss of follow-up: 2 Adverse event: 1 Lack of adherence*: 1
Withdrawn: n=4 Reason for withdrawal: Loss of follow-up: 3 Violation of protocol: 1
*Use of less than 80% of the study medication
Included N=180
Visit 5 (completion of study)
N=59
Visit 5 (completion
of study) N=56
Table1–Demographiccharacteristicsandbaselineclinicalcharacteristics.
Demographiccharacteristics GAO
N=71
GO
N=70
pvalue (GAOvs.GOa)
Age,years
Mean±SD 67.1±10.9 64.9±10.4 0.224a
Limits 44–90 44–92
Agestratum,N(%)
<65years 33(46.5) 34(48.6)
≥65years 38(53.5) 36(51.4)
Ethnicity
White 50(70.4) 57(81.4) 0.389b
Black 6(8.5) 4(5.7)
Mixed 15(21.1) 9(12.9)
Weight(kg)
Mean±SD 58.5±11.5 61.3±12.0 0.1502a
Limits 36–88 34–89
Height(cm)
Mean±SD 150±6 152±6 0.0482a
Limits 137–165 140–174
Lengthoftimesincemenopause(years)
Mean±SD 19.8±12.1 18.3±9.8 0.4392a
Limits 3–55 2–43
LengthoftimefromCollesfractureoccurrencetobaseline,days
Mean±SD 3.5±1.7 3.4±1.8 0.580a
a ttestforindependentvariables.
b Chi-squaretest.
Table2–ChangeinTscoreinproximalforearm(33%)onfracturedside,expressedaspercentage,inmodifiedITT population.
V4 V5 pvaluea
GAO
No.ofpatients N=59 N=59
Mean±SD −25.7±40.7 −20.8±39.5
Min/Median/Max −200/−15.2/27.8 −200/−9.1/15.4 0.727
GO
No.ofpatients N=57 N=56
Mean±SD −31.9±62.5 −32.8±68.0
Min/Median/Max −400/–21.4/75 −366.7/−18.9/90 0.769
pvalueb(groups) 0.352 0.069
a Wilcoxonsignedranktest.
b Mann–WhitneyUtest.
theCollesfracturewasI orII/IIa:15/71patients(21.1%)and 46/71(64.8%),respectively,inGAO;and16/70(22.9%)and43/70 (61.4%),respectively,inGO(p=0.917).
TheBMDmeasurement(evaluatedbymeansoftheTscore) didnotshowanystatisticallysignificantdifferencebetween thetreatmentgroupsatthebaseline,inforearmsdiagnosed withfractures,inforearmswithoutfracturesandinthe lum-barspine,femoralneckandtotalfemur.Themajorityofthe patientsinthetwotreatmentgroupsusedatleast80%ofthe totalnumberofpillsplannedpervisit.
Findingsonthesideofthefracturedforearm
Onthesideofthefracturedforearm,adecreaseinBMDwas observed(evaluatedusingthe%oftheTscore)fromV0 to
V4(90days)andV5(180days)inthetwotreatmentgroups, rangingfrom20.8%to32.8%(Table2).
There was atendency towardgreater reductioninBMD (evaluatedusingthe Tscore)amongthepatientsinGO.At V4,thisreductionwasapproximately15%inGAOand21%in GO.AtV5,thislossofBMDwasapproximately9%inGAOand 19%inGO.Nostatisticallysignificantdifferencebetweenthe groupswasreachedateithervisit:p=0.352and0.069forV4 andV5,respectively(Table2).Likewise,nostatistically signif-icantdifferenceinTscorevariationwasfoundincomparing V4andV5inthetwogroups(p=0.727and0.769forGAOand GO,respectively).
Table3–ChangeinTscoreinproximalforearm(33%)on fracturedside,expressedaspercentage,inPP
population.
Groups V4 pvalue(groups)a
GAO
No.ofpatients N=45 Mean±SD −24.6±41.9 Min/Median/Max −200/−15.2/27.8
GO
No.ofpatients N=46 Mean±SD −27.4±30.8
Min/Median/Max −166.7/−23.0/20% 0.110
a Mann–WhitneyUtest.
FromV0 toV4 (day90),mostofthepatientsinthetwo treatmentgroupspresentedlossofBMD:46/63(73.0%)inGAO and46/60(76.7%)inGO.Themean±SDforthelossofBMD was−0.5(0.4)inGAOand−0.7(0.4)inGO.ComparingV0with V5(day180),alossofBMDcouldbeseenin39/59patients (66.1%)inGAOandin43/56(76.8%)patientsinGO.Themean ±DPofthedifferenceinBMDbetweenV0andV5was−0.5 (0.4)forGAOand−0.7(0.4)forGO.
Findingsonthenon-fracturedside
Inthenon-fracturedforearm,theBMDevaluatedaccordingto thechangeinTscore(%)fromV0untilthevisitsV4andV5 rangedfrom4.2%upwards(anincreasefromV0toV4,i.e.day 90)to−6.0%downwards(areductionfromV0toV5,i.e.day 180)(Table4).
AtV4,theincreaseinBMD(evaluatedaccordingtotheT
score)wasseentobegreaterinGO(4.2%)thaninGAO(1.9%); andatV5,therewasareductioninBMD(evaluatedaccording totheTscore)inthetwogroups.ItwasgreaterinGO(−5.7%) thaninGAO(−2.2%).Nostatisticallysignificantdifferences wereobservedbetweenthetreatmentgroupsatthetwovisits orbetweenthevisitsforthetwotreatmentgroups(Table4).
Furthermore,approximately30%and42%ofthepatients inthetwotreatmentgroupsshowedlossesofBMDfromthe baselinetoV4(day90)andtoV5(day180),respectively.
In relation to the proportion of patients with losses of BMD at V4, there was a statistically significant difference
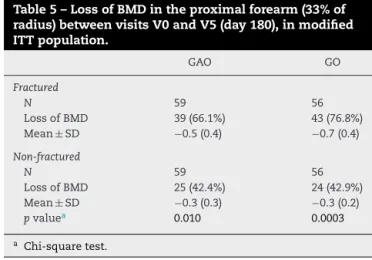
Table5–LossofBMDintheproximalforearm(33%of radius)betweenvisitsV0andV5(day180),inmodified ITTpopulation.
GAO GO
Fractured
N 59 56
LossofBMD 39(66.1%) 43(76.8%)
Mean±SD −0.5(0.4) −0.7(0.4)
Non-fractured
N 59 56
LossofBMD 25(42.4%) 24(42.9%)
Mean±SD −0.3(0.3) −0.3(0.2)
pvaluea 0.010 0.0003
a Chi-squaretest.
between the fractured and non-fractured sides in the two treatmentgroups(GAOandGO;p<0.0001forboth).This dif-ferenceinpatternobservedintheforearmsbetweenthesides wasprobablyrelatedtotheimmobilizationofthefractured side(Table5).
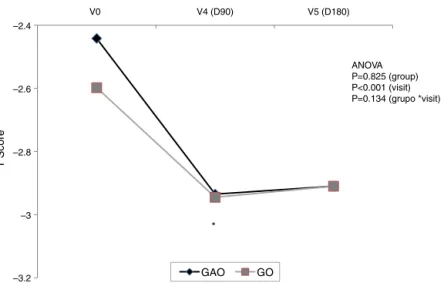
TheANOVA modelcompared the mean T scoresin the
twotreatmentgroupsbetweenthevisits,usingthetreatment group(GAOorGO)andthevisits(V0,V4andV5)asfactors, along withtheir respectiveinteractions.There was no evi-denceofsignificantinteractionbetweenthefactors,eitherfor thesidewiththefracture(p=0.134)orforthenon-fractured side(p=0.982).Thissuggeststhatthetwotreatmentgroups hadsimilarpatternsoverthecourseoftime(Figs.2and3).
Onthesidewiththefracture,therewasastatistically sig-nificantdifferencebetweenthevisits,suchthatthemeanT
scoreswere significantlylower atV4 and V5,inrelationto V0 (p<0.001),althoughno differences were foundbetween thetreatmentgroups(p=0.825)(Fig.2).Onthesidewiththe fracture, therewas no evidence of any statistically signifi-cantvariationbetweenthegroups(p=0.554)orvisits(p=0.081) (Fig.3).
Radiologicalevaluation
Theresultsfromradiologicalidentificationofthecallusover thecourseofthevisitsdidnotshowanyevidenceofany sig-nificantdifferencebetweenthetreatmentgroupsatthevisits
Table4–ChangeinTscoreinproximalforearm(33%)onnon-fracturedside,expressedaspercentage,inmodifiedITT population.
V4 V5 pvaluea(visits)
GAO
No.ofpatients N=59 N=59
Mean±SD 1.9±17.4 −2.2±28.2
Min/Median/Max −36.4/0/79.2 −133.3/0/75.5 0.223
GO
No.ofpatients N=57 N=56
Mean±SD 4.2±37.4 −5.7±29.8
Min/Median/Max −142.9/3.8/150 −142.9/0/34.6 0.128
pvalueb(groups) 0.438 0.861
a Wilcoxonsignedranktest.
–3.2 –3 –2.8 –2.6 –2.4
V0 V4 (D90) V5 (D180)
GAO GO
ANOVA P=0.825 (group) P<0.001 (visit) P=0.134 (grupo *visit)
*
T Score
Fig.2–ResultsfromtheANOVAmodelforthefracturedside.
–3.2 –3 –2.8 –2.6 –2.4
V0 V4 (D90) V5 (D180)
GAO GO
ANOVA P=0.554 (group) P=0.081 (visit) P=0.982 (grupo *visit)
*
T Score
Fig.3–ResultsfromtheANOVAmodelforthenon-fracturedside.
V1(p=0.674),V2(p=0.755)andV3(p=0.749),withregardtothe proportionofthepatientsinwhomthecalluswasidentified onX-rays.Attheothervisits(V4andV5),thecalluswasseen bymeansofX-raysinalmostallthepatients,inbothgroups, andnostatisticalcomparisonwasmade.
Safety
InGAO,23/71randomizedpatients(32.4%)reported thatat least one adverse event occurred during the study period, totaling 34 suchevents. In GO, 23/70 randomizedpatients (32.9%)reportedthatadverseeventsoccurredduringthestudy period,totaling 41 suchevents.Three adverseevents were consideredbytheinvestigatortobeserious.InGAO,onecase ofrenewedfracturingofthewristwasreported.Thiswas con-sideredtobeofmoderateintensityandneededhospitalization andsurgeryforexternalfixationtobeimplemented.Itwas reportedthatthepatienthadrecovered.InGO,twocasesof adverseeventsoccurred.Oneoftheseconsistedofa hypoe-choicaccumulationintherightcalf,whichwasconsideredto beofmoderateintensity.Thiscaserequiredhospitalization
andthepatientwasstillrecoveringatthetimeofthisreport. Theotheradverseeventcomprisedcardiorespiratoryarrest, whichoccurredatthepatient’shome,wasofsevereintensity andresultedindeath.
Noneofthesethreeadverseeventswasconsideredbythe investigatortoberelatedtothestudymedication.InGO,both oftheadverseeventsledtointerruptionofthetreatment.For the patientinGAO,administrationofthestudy medication wasnotimmediatelystoppedbecauseoftheadverseevent, buttheeventledtowithdrawalfromthestudy.
Discussion
Inthepresentstudy,after90daysofrisedronateuse,no signifi-cantvariationinthelossofBMDwasseeninthefracturedarm, orinthenon-fracturedarm.Thesamepatternwasobserved after180daysoftreatment,whichsuggeststhatrisedronate hasaprotectiveeffectduetotheimmobilization.
Several medications have been used to improve bone
consolidation, both for accelerating the process and also for improving the quality of the bone callus, i.e. through improvingthemicroarchitecture,volumeandbiomechanical strengthofthecallus.Thesemedicationsincludestrontium ranelateanddrugsthatactontheWntsignalingsystem,such teriparatideandtheantibodiesanti-sclerostinandDKK-1.12–15 Somemedications havebeenrecognizedasharmfulto cal-lusformationandtheseincludecorticoids,chemotherapeutic agents,antibiotics,anti-inflammatoryagents,anticoagulants andanticonvulsants.16
However,bisphosphonates arethe drugsthathavebeen studiedmost.Thesefavorformationofamorevoluminous callus with mineralization and make the callus mechani-callymorecompetent,butwithaslowerremodelingrate.17–22 Anotherfactordiscussedintheliteraturehasbeenthetime atwhichbisphosphonateuseshouldstart,afterafracturehas occurred.Someevidencefavorsstartingtouse bisphospho-nates15daysaftertheevent,whileotherevidencesuggests that, independent of the time at which they are admin-istered, they do not interfere with bone consolidation or withpostoperative healing followingoccurrences of osteo-poroticfractures.23,24 Thetimetakentoreachconsolidation isunrelatedtothe severityoftheosteoporosis orthe type offracture.25Therapyusingbisphosphonatescanbe contin-uedafteroccurrencesoffracturesofthedistalradius,without deleteriousclinicaleffectsonconsolidation.26
When used for long periods, bisphosphonates may
increasetheoccurrencesofmicroandmacrofracturesin ani-malsandhumans.Theyalsogiverisetopreferentialfracture sites.However,biomechanicalgainsregardingthebone cal-lusareobserved(sizeandexternaldiameter).Itseemsthat theorganismcompensatesforthenegativeeffectofthe med-icationandmodulatesthemorphologyofthecallussoasto obtainbetterbiomechanicalfunction(mechanostat).27
Theeffectsofrisedronatehavebeenstudiedbothin rela-tion toimprovement ofbonemineral density and fracture preventioninpatientswithosteoporosis andin relationto use during bone consolidation. It has been observed that risedronate does not interfere negatively with bone callus formationandcanbeusedwithoutdeleteriouseffectson con-solidation.On the contrary,it increasesthe volume ofthe callusanditsbiomechanicalresistance.28,29
TheBMD of33% of the radiuson the fractured side at theendofsixmonths(V5)presentedanegativechange of 32.8%intheOscalgroupandonly20.8%intheActonel+Oscal group,whichshowedthatrisedronatehadatendencytoward havingaprotectiveeffectagainstlossofBMDcausedby post-fractureimmobilization(p=0.069).Eventhoughtherewasno statisticallysignificantdifferencebetweenthetwogroups,it wasseenthattherewaslowerlossofBMD(evaluatedusing
T scores) in the group treated with Actonel+Oscal (mean
decreaseof−0.5),inrelationtothegroupthatusedOscalalone (meandecreaseof−0.7),asshowninTable5.Thiswaspossibly duetothegreatvariabilityofthedata.
TheBMDof33%oftheradiusonthenon-fracturedsideat theendofsixmonths(V5)presentedanegativechangeof5.7% inGOandonly2.2%inGAO,withadifferenceof3%infavor ofrisedronate.However,therewasnostatisticallysignificant difference(p=0.861)(Table4).
AsshowninFig.2, theinitialBMDof33%oftheradius onthefracturedside(measuredusingtheTscore)decreased significantly(p<0.001)duringthetreatment(fromV0toV5), whilethisdifferencewasnotobservedonthenon-fractured side. This shows the significant influence of immobiliza-tion ofafractureonboneloss.Regarding theproportionof patientswithlossofBMDatV5,therewasastatistically sig-nificantdifferencebetweenthefracturedandnon-fractured sides,forbothtreatmentgroups(GAO,p=0.010;GO,p=0.0003) (Table 5). This pattern of difference observed between the groupswasprobablyrelatedtoimmobilizationofthefractured side(Table5).Thesedatashowthatrisedronateprovided pro-tectioninrelationtolossofBMDduringtheimmobilization ofalimb(osteoporosisofdisuse),whichisdiscussedinother studies.30
Therewasnosignificantdifferenceinradiological identifi-cationofthebonecallusatthetimesofthevisits(V1toV5), orbetweenthetreatmentgroups.Thus,useofrisedronatein ourstudydidnotpresentanynegativeclinicaleffectonbone consolidation.Inmostofthepatients,radiological identifica-tionofthecallusoccurredatV3,withasimilarpatterninthe twogroups.Furthermore,thesafetyprofileofrisedronatewas showntobesimilartothatofthecontrolgroup.
Limitationsofthestudy:Giventhatthisstudywasdesigned withoutcomparisonwithplacebo,webelievethattheremay havebeenanimportanteffectonBMD,sincethetestswere evaluated centrally,asdescribedinthe methodology. How-ever,basedonthewell-establishedsideeffectsthathavebeen describedpreviouslyforthisclassofmedications,aneffectin interpretingthesafetydatacannotbetotallyruledout.
Conclusions
PostmenopausalwomenwithCollesfractures whoreceived sodiumrisedronatepluscalciumandvitaminD,in compar-ison with calcium and vitamin D only, did not show any significantdifferenceregardinglossofBMDinthefractured andnon-fracturedforearmafter90days(primaryobjective) and 180days(secondaryobjective).Risedronatewasshown tohaveatendencytowardaprotectiveeffectregardingloss ofBMDduetoimmobilization.Thetimetakentoreach frac-tureconsolidationwasunaffectedandthetwogroupsshowed similarsafetypatterns.
Conflicts
of
interest
sponsoredbyServierLaboratories,Sanofi-Aventis,Lillyand BlauFarmacêutica.
Thisstudy receivedfinancial support and backing from Sanofi forits design, conduction, data-gathering, manage-ment, data analysis and data interpretation, along with editorialassistanceforthemanuscript.
Acknowledgments
OurspecialthankstoDrs.BenHurAlbergaria,MárcioPassini deSouza,Jorge dosSantosSilvaand Edson Cerqueira Gar-cia de Freitas for their valuable contributions toward the designofthis researchprojectand collaborationin discus-sionsregardingtheproject,andindraftingthefinaltextof thismanuscript.
r
e
f
e
r
e
n
c
e
s
1. FleischH.Canbisphosphonatesbegiventopatientswith fractures.JBoneMinerRes.2001;16(3):437–40.
2. LiJ,MoriS,KajiY,MashibaT,KawanishiJ,NorimatsuH.Effect ofbisphosphonate(incadronate)onfracturehealingoflong bones.JBoneMinerRes.2001;14(3):969–79.
3. NymanMT,PaavolainenP,LindholmTS.Clodronateincreases thecalciumcontentinfracturecallus.ArchOrthopTrauma Surg.1994;112(5):228–31.
4. SchenkRK.Biologyoffracturerepair.In:BrownerBD,Jupiter JB,LevineAM,TraftenPG,editors.Skeletaltrauma.
Philadelphia,PA:Saunders;1998.p.31–75.
5. BarnesGL,KsotenuikPJ,GerstenfeldLC,EinhornTA.Growth factorregulationoffracturerepair.JBoneMinerRes. 1999;14(11):1805–15.
6. HyvönenPM,KarhiT,KosmaV-M,Liimola-LuomaL, HanijärviH.Theinfluenceofdichloromethylene bisphosphonateonthehealingofalongbonefracture, compositionofbonemineralandhistologyofboneintherat. PharmacolToxicol.1994;75(6):384–90.
7. GoodshipAE,WalkerPC,McNallyD,ChambersT,GreenJR. Useofabisphosphonate(pamidronate)tomodulatefracture repairinovinebone.AnnOncol.1994;5(Suppl7):S53–5. 8. PeterCP,CookWO,NunamakerDM,ProvostMT,SeedorJG,
RodanGA.Effectofalendronateonfracturehealingandbone remodelingindogs.JOrthopRes.1996;14(1):74–9.
9. MadsenJE,Berg-LarsenT,KirkebyOJ,FalchJA,NordslettenL. Noadverseeffectsofclodronateonfracturehealinginrats. ArchOrthopScand.1998;69(5):532–6.
10.OliveiraLAA,GuarnieiroR,RodriguesCJ,SantanaPJ, BatistaMA.Avaliac¸ãodoefeitodoresidronatosódicona consolidac¸ãodefraturas:estudoexperimentalemratos.Acta OrtopBras.2004;12(2):7–83.
11.Colón-EmerichC,NordslettenL,OlsonS,MajorN,BoonenS, HaentjensP,etal.Associationbetweentimingofzoledronic acidinfusionandhipfracturehealing.OsteoporosInt. 2011;22(8):2329–36.
12.PietrograndeL,RaimondoE,FossaliA,ZaolinoC.Biological andpharmacologicalfactorinfluencingthefracturehealing. AgingClinExpRes.2011;23(2Suppl):65–8.
13.GoldhahnJ,FerónJM,KanisJ,PapapoulosS,ReginsterJY, RizziliR,etal.Implicationsforfracturehealingofcurrentand
newosteoporosistreatments:anEsceoconsensuspaper. CalcifTissueInt.2012;90(5):343–53.
14.BukataSU.Systematicadministrationofpharmacological agentsandbonerepair:whatcanweexpect.Injury. 2011;42(6):605–8.
15.AspenbergP,JohanssonT.Teriparatideimprovesearlycallus formationindistalradialfractures.ActaOrthop.
2010;81(2):234–6.
16.PountosI,GeorgouliT,BlokhuisTJ,PapeHC,GiannoudisPV. Pharmacologicalagentsandimpairmentoffracturehealing: whatistheevidence.Injury.2008;39(4):384–94.
17.MatosMM,TannuriU,GuarnieiroR.Theeffectofzoledronate duringbonehealing.JOrthopaedTraumatol.2010;11(1): 7–12.
18.MashibaT,HiranoT,TurnerCH,ForwoodMR,JohnstonCC, BurrDB.Suppressedboneturnoverbybisphosphonates increasesmicrodamageaccumulationandreducessome biomechanicalpropertiesindogribs.JBoneMinerRes. 2000;15(4):613–20.
19.FloraL,HassingGS,ParfittAM,VillanuevaAR.Comparative skeletaleffectsoftwodiphosphonatesindogs.MetabBone DisRelatRes.1980;2:389–407.
20.LiJ,MoriS,KajiY,KawanishiJ,AkiyamaT,NorimatsuH. Concentrationofbisphosphonate(incadronate)incallusarea anditseffectsonfracturehealinginrats.JBoneMinerRes. 2000;15(10):2042–51.
21.LenehanTM,BalligandM,NunamakerDM,WoodFEJr.Effect ofEHDPonfracturehealingindogs.JOrthopRes.
1985;3(4):499–507.
22.KimTY,HáYC,KangBJ,LeeYK,KooKH.Doesearly administrationofbisphophonateaffectfracturehealingin patientswithintertrochantericfractures.JBoneJointSurgBr. 2012;94(7):956–60.
23.JorgensenNR,SchwarzP.Effectsofanti-osteoporosis medicationsonfracturehealing.CurrOsteoporosRep. 2011;9(3):149–55.
24.AspenbergP,WermelinK,TengwallP,FahlgrenA.Additive effectsofPTHandbisphosphonatesonthebonehealing responsetometaphysealimplantsinrats.ActaOrthop. 2008;79(1):111–5.
25.GongHS,SongCH,LeeYH,RheeSH,LeeHJ,BaekGH.Early initiationofbisphosphonatedoesnotaffecthealingand outcomesofvolarplatefixationofosteoporoticdistalradial fractures.JBoneJointSurgAm.2012;94(19):1729–36.
26.RozentalTD,VasquezMA,ChackoHT,AyoguN,BouxseinML. Comparisonofradiograficfracturehealinginthedistalradius forpatientsonandofbisphosphonatetherapy.JHandSurg Am.2009;34(4):595–602.
27.LittleDG,RamachandranM,SchindelerA.Theanabolicand catabolicresponseinbonerepair.JBoneJointSurgBr. 1998;9(4):425–33.
28.BoyceRW,PaddockCL,GleasonJR,SietsemaWK,EriksenEF. Theeffectsofrisedronateoncaninecancellousbone remodeling:three-dimensionalkineticreconstructionofthe remodelingsite.JBoneMinerRes.1995;10(2):211–5.
29.HarrisST,WattsNB,GenantHK,McKeeverCD,HangartnerD, KellerM,etal.Effectsofrisedronatetreatmentonvertebral andnonvertebralfracturesinwomenwithpostmenopausal osteoporosis.JAMA.1999;14(14):1344–52.
30.MaedaH,KimmelDB,LaneN,RaabD.Themusculoskeletal responsetoimmobilizationandrecovery.Bone.