w w w . r b o . o r g . b r
Original
Article
Intra
and
interobserver
concordance
of
the
AO
classification
system
for
fractures
of
the
long
bones
in
the
pediatric
population
夽
Artur
Yudi
Utino
∗,
Douglas
Rene
de
Alencar,
Leonardo
Fernadez
Maringolo,
Julia
Machado
Negrão,
Francesco
Camara
Blumetti,
Eiffel
Tsuyoshi
Dobashi
EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(Unifesp),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8August2014 Accepted21August2014 Availableonline15August2015
Keywords:
Bonefractures/classification Child
Orthopedics Method
a
b
s
t
r
a
c
t
Objective:TheAOclassificationforfracturesofthelongbonesinthepediatricpopulation wasdevelopedandvalidatedin2006.However,thecomplexityofthissystemhaslimited itsuseinclinicalpracticeandfewstudiesintheliteraturehaveevaluateditsreproducibility andapplicability.Thepresentstudyhadtheobjectiveofdeterminingtheintraand interob-serveragreementusingthepediatricAOsystem,amongphysicianswithdifferentlevelsof experience.
Methods:Aftermakingthesamplecalculation,108consecutiveradiographsonlong-bone fracturesinpatientsaged0–16years,comingfromthedigitalfilesofthequaternary-level hospital,wereselected.Theradiographswereclassifiedbyfiveexaminerswithdifferent levelsofexperienceafterpriorexplanationsaboutthesystem.Achartcontainingimages fromtheclassificationwasmadeavailableforconsultation.Theevaluationsweremadeat twodifferenttimesbyeachobserver.TheFleisskappaindexwasusedtoascertaintheintra andinterobserveragreement.
Results:Intraobserveragreementthatwasatleastsubstantialwasobtainedforalltheitems oftheclassificationanditreachedexcellentlevelsforallobserversinrelationtofiveofthe sevenitemsconsidered.Theinterobserverevaluationpresentedexcellentlevelsof agree-mentintwoitems,substantialintwoitems,moderatetosubstantialinoneitemandpoor tomoderateinoneitem.Noinfluencefromtheobserver’sexperiencewasobservedwith regardtoobtaininghigherorlowerlevelsofagreement,eitherintheintraobserverorinthe interobserverevaluation.
Conclusions: Inthisstudy,theintraandinterobserveragreementwasconsideredtobegood orexcellentforthepediatricAOclassificationsystem,fortheparametersofbone,segment, pairedbone,subsegment,standardanddeviation.However,theintra andinterobserver
夽
WorkdevelopedintheDisciplineofPediatricOrthopedics,DepartmentofOrthopedicsandTraumatology,UniversidadeFederalde SãoPaulo(Unifesp),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.Y.Utino). http://dx.doi.org/10.1016/j.rboe.2015.08.001
agreementwasstatisticallyunsatisfactoryfortheparameterofseverity/sideofavulsion.The levelsofagreementobtaineddidnotdependontheobserver’slevelofexperiencewithin pediatricorthopedics.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Concordância
intra
e
interobservadores
do
sistema
de
classificac¸ão
AO
para
fraturas
dos
ossos
longos
na
populac¸ão
pediátrica
Palavras-chave:
Fraturasósseas/classificac¸ão Crianc¸a
Ortopedia Método
r
e
s
u
m
o
Objetivo:Aclassificac¸ãoAOparafraturasdosossoslongosnapopulac¸ãopediátricafoi desen-volvidaevalidadaem2006.Entretanto,acomplexidadedessesistematemlimitadooseu usonapráticaclínica.Poucosestudosnaliteraturaavaliamsuareprodutibilidadee aplicabil-idade.Estetrabalhotevecomoobjetivodeterminaraconcordânciaintraeinterobservadores comousodosistemadeclassificac¸ãoAOpediátricaentremédicosdediferentesníveisde experiência.
Métodos: Apósafeituradocálculoamostral,foramselecionadas108radiografias consecu-tivasdefraturasdeossoslongosdepacientesde0–16anos,provenientesdoarquivodigital deumhospitaldenívelquaternário.Asradiografiasforamclassificadasporcinco exami-nadorescomdiferentesníveisdeexperiênciaapósumaexplicac¸ãopréviasobreosistema. Foimostradaumaplanilha quecontinhaasimagensdaclassificac¸ãoparaconsulta.As avaliac¸õesforamfeitasemdoismomentosdistintosporcadaobservador.OíndiceKappa deFleissfoiusadoparaverificaraconcordânciaintraeinterobservadores.
Resultados: Foramobtidasconcordânciasintraobservadoresnomínimosubstanciaisem todosositensdaclassificac¸ão,alcanc¸aramníveisexcelentesportodososobservadoresem cincodosseteitensconsiderados.Aavaliac¸ãointerobservadoresapresentouníveisde con-cordânciaexcelentesemdoisitens,substancialemdoisitens,moderadaasubstancialem umitemepobreamoderadaemumdositens.Nãoseobservouinfluênciada experiên-ciadoobservadornaobtenc¸ãodemaioresoumenoresníveisdeconcordância,intraou interobservadores.
Conclusões: Nesteestudo,aconcordânciaintraeinterobservadoresfoiconsideradaboaou excelenteparaosistemadeclassificac¸ãoAOpediátricoparaosparâmetros:osso,segmento, ossopareado,subsegmento,padrãoedesvio.Noentanto,aconcordânciaintrae interob-servadoresfoiestatisticamenteinsatisfatórianoparâmetrogravidade/ladodaavulsão.Os níveisdeconcordânciaobtidosindependemdaexperiênciadoobservadoremortopedia pediátrica.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Themainreasonforhospitalizationwithinpediatric ortho-pedicsisfractures ofthe long bones.1 Classificationofthe fracturesisessentialfordeterminingtheepidemiology, facil-itating communication between orthopedists and defining treatment algorithms.2 Several classification systems have beendevelopedbasedonthelocationandmorphologyofthe injuries,inordertocategorizeeachtypeofinjuryoflongbones inchildren.1
TheAOclassificationforlong-bonefracturesinadultsisnot usedforthepediatricpopulationbecauseitdoesnottakeinto considerationtheboneelasticity,presenceofthegrowthplate andanatomicalcharacteristics ofthe epiphysis.1Thesame traumamechanismmayproducedifferentfracturepatterns
inchildren,suchasplasticdeformities,greenstickfractures andcomplexfractures.1Anotherimportantcharacteristicis thegreaterfragilityofthegrowthplate,whichislessresistant thanthesurroundingbone,thusmeaningthatthisstructure ismoreeasilyinjured.
ThepediatricAOclassificationtakesintoconsiderationthe AOsystemforlong-bonefracturesinadultsandthemost rel-evantpediatricfractures.Thelocationofthefractureandits morphologyaretakenintoconsideration.Theboneis subdi-videdintothreesegments:proximal(epiphysis+metaphysis), diaphyseal and distal (epiphysis+metaphysis). Regarding morphology,thediseasecodeforthechildandthefracture severityanddisplacement,whichdependonthetypeof frac-ture,areconsidered.1
TheauthorsofthepediatricAOclassificationhavealready reachedthe thirdstageofthe validationprocess,i.e. appli-cation of the proposed system within the context of a prospectiveclinicalstudy.2However,thedegreeof complex-ity of this method and the difficulty in incorporating it into clinical practice lead us to believe that studies eval-uating its reproducibility and accuracy are still needed, especially if less experienced orthopedists are taken into consideration.
Thus,weconceivedthisstudywiththeaimofestimating theintraand interobserver agreementofthe AO classifica-tionsystemforlongbonesinchildren,amongexaminerswith differentlevelsofexperience.
Materials
and
methods
Thisresearchprojectwas submittedtothe researchethics committeeoftheBrazilPlatformforassessmentandapproval (approvalnumber:29073114.3.0000.5505).
Samplecalculation
Firstly,wedeterminedthenumberofradiographsthatwould beneededtoobtainkappavaluesgreaterthan0.70,through testswithasignificancelevelof5%andpowerof80%.The calculationshowedthatwewouldneedtoevaluateatleast 95radiographs.Theformulausedforthiscalculationwasas follows4:
N={(z(alpha)∗root(Q0)+z(beta)∗root(Q1))/(K1−K0)}2
Inwhichz(alpha) andz(beta)areobtainedfromthe nor-maldistribution;Q0andQ1areobtainedfromthetableofthe referencearticleforthesamplesize;andK1and K0 arethe kappavaluesobtainedfromthehypothesesofthetest.Forthis analysis,weobtain:
N={(1.64∗root(0.817)+0.84∗root(0.301))/(0.9−07)}2=94.92
Sampleselection
These examinations were obtained consecutively between January 2013 and March 2014 in the imaging diagnostics department of a quaternary-level university hospital, with priorauthorization.Alltheradiographsproducedduringthis periodthatwere identified inthedigital filesas imagesof segments of the appendicular skeleton were obtained for evaluation.Thesesegmentsincludedthepelvis,thigh,knee, lower leg, ankle, shoulder, upper arm, elbow, forearm and wrist.Examinationsperformedonchildrenaged0–16years whopresentedfractureofthelongboneswereincluded.The
radiographswereselectedsoastoincludeexaminationswith twoviewsandgoodradiographicquality.Thiswasdonebytwo orthopedistswhodidnotparticipateintheclassification pro-cess.Thus,119radiographsonfracturesofthelongboneswere collected,inanteroposteriorandlateralviews.Amongthese, sixwereexcludedduetopoorquality andfivebecausethe growthplatehadalreadyclosed.Thestudythereforeincluded 108radiographs.
Processofclassifyingtheradiographs
Theradiographswereclassifiedbyfiveexaminerswith differ-entlevelsofexperience.Onewasatexpertlevel(>10years ofexperienceasapediatricorthopedist–examiner5),one wasatadvancedlevel(>5yearsofexperienceasapediatric orthopedist–examiner4),onewasatmediumlevel(>1year ofexperience asapediatric orthopedist–examiner 3) and twowereatbasiclevel(generalorthopedists–examiners1 and2).
Withtheaimofminimizingbiasduetodifficultiesin inter-pretationandinexperiencewiththeclassificationsystem,the observersweregivenpriorexplanationsregardingthe classi-ficationsystemsused.Furthermore,duringtheclassification process,abrochurecontainingtheentireAOclassificationfor pediatriclong-bonefractureswasavailableforeach partici-pant.
The radiographs were organized in chronological order in a closed digital file. The classifications were made by fiveobservers,attwodifferenttimes,withanintervalof15 daysbetweenoneevaluationandtheother.Eachofthefive researchersevaluatedandclassifiedtheradiographs indepen-dently.Theobserversweregivenallthetimethattheyneeded toevaluatetheradiographs.
Theparticipantswereinstructednottodiscussthe clas-sification systems untilthe end of the classificationstage. Furthermore,theydidnothaveaccesstothe patients’ his-toriesortoanyclinicaldata.
Statisticalanalysis
Thestatisticalanalysisontheresultsobtainedwasperformed byaspecialistprofessionalinthefieldofmedicalstatistics. TheFleisskappatestwasusedtoassesstheintraand interob-serveragreementforeachscale.5,6Itisconsideredthatusing theFleisskappacoefficientisthemostappropriatemethod forsituationsinwhichmultipleexaminationsorevaluations are made and when the scale evaluated presents several categories.7
Fractureclassificationsystem
Theoverallstructureoftheclassificationisbasedonthe loca-tionofthefractureanditsmorphology.Thefracturelocations coveredarethedifferentlongbonesandtheirrespective seg-mentsandsubsegments.Themorphologyofthefractureis describedbyaspecificcodethatrepresentsthefracture pat-tern,withacodefortheseverityandanadditionalcodethat isusedforcertaintypesoffractures(displacedsupracondylar fracturesofthehumerus,displacedfracturesoftheheadand neckoftheradiusandfracturesofthefemoralneck).10
Thenumberingsystemforthelongbones(1–4)andforthe segments(proximal=1,diaphyseal=2anddistal=3)issimilar tothatoftheAOsystemdescribedbyMüllerforfracturesof thelongbonesinadults.11Itdiffersinrelationtothecoding formalleolarfractures,suchasfracturesofthedistaltibiaor fibula.Moreover,thedefinitionsofthethreebonesegments differfromthoseofadults.ThelettersR,U,TandFreferto theradius,ulna,tibiaandfibulaandareaddedtothecode forthesegment,inrelationtopairedbones,whenonlyone boneisfracturedorwhenbothbonesarefracturesbutwith differentpatterns.10
Withregard tothe subsegments, segments 1and 3 are subdividedintotwosubsegments:theepiphysis(E)andthe metaphysis(M).Segmenttwoisthesameasthediaphyseal subsegment(D).10
Themetaphysisisdefinedasasquareinwhichthesides have the same length as the widest part of the growth place.Inrelationtopairedbonessuchastheradius/ulnaand tibia/fibula,bothbonesshouldbeincludedinthesquare.The proximalfemurisanexception:itsmetaphysisisnotdefined asasquarebutislocatedbetweenthegrowthplateandthe subtrochantericline.10
Ifthecenterofthefracturelineislocatedinsidethe above-mentionedsquare,itisametaphysealfracture.Iftheepiphysis andtherespectivegrowthplate(physis)areincluded,itisan epiphysealfracture.Intraandextra-articularligament avul-sionsareepiphysealandmetaphysealinjuries,respectively.10 Acertainnumberoffracturepatternsthatareimportant inchildrenaredescribedbytheso-called“childcode”.These fracturepatterns arespecificforthe subsegmentsinwhich theyarelocatedandthusaregroupedasE,MorD.Thiscode alsotakesintoconsideration someinternationallyaccepted classificationsystemsforpediatricfractures(suchasthe clas-sificationofSalter–Harris).3,10,12
Theseveritycodedistinguishesbetweentwogrades: sim-ple(.1)andmultifragmented(.2).Todescribethesideofthe avulsion,whennecessary,theletterMwouldindicatemedial ligamentavulsionandtheletterL,lateral.
Supracondylarfracturesofthehumerus, whichare clas-sifiedas13-M/3,aredescribedusinganadditionalcodethat takes into consideration the degreeof displacement (I–IV), whichisverysimilartotheclassificationofGartland.13
Whenthe pairedbones(radius/ulna ortibia/fibula) both presentthesamefracturepattern,theyshouldbedocumented byonlyoneclassificationcode.Inthiscase,theseveritycode willbethatofthebonethatismoreseverelyfractured.On the otherhand, whenonlyonebone isfractured,a lower-caseletterdefinesthisbone(r,u,torf)andshouldbeadded tothe code forthe segment.For example,22u describes a
Table1–Statisticalanalysisonintraobserveragreement accordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedin thepediatricAOclassification:inthistable,thebone.CI, confidenceinterval.
AOclassification Fleisskappaindex 95%CI
Lower Upper
Bone
Examiner1 1 1 1
Examiner2 1 1 1
Examiner3 1 1 1
Examiner4 0.99 0.9704 1
Examiner5 1 1 1
diaphyseal fracture of the ulna in isolation. Furthermore, when the two bones are fractured with different fracture patterns, each fracture should beclassified separately and alower-case letter shouldbeincluded intheclassification. For example, a complete spiral fracture of the radius and plasticdeformityofthe ulnaareclassifiedas22r-D/5.1and 22u-D/1.1.10
Fracturesoftheheadandneckoftheradiusaredescribed byanadditionalcode(I–III)thattakesintoaccounttheangle andgradeofdisplacement.Fracturesofthefemoralneckare proximalmetaphysealfractures(M),withanintertrochanteric linethatlimitsthemetaphysis.Thesemetaphysealfractures can be divided into threetypes, which are representedby an additional code (I–III)that takes into account the posi-tionofthefractureintheproximalmetaphysis:transcervical, basicervicalandtranstrochanteric.10
Results
Intraobserveragreement
Thedatarelatingtothestatisticalevaluationonintraobserver agreementandtherespectiveresultsaccordingtotheFleiss kappaindexareshowninTables1–7.Eachitemthatforms partoftheclassificationwasanalyzedindependentlyandis presentedinaspecifictable.
Ingeneralterms,substantialcorrelationofagreementwas foundinrelationtopracticallyalltheitemsaddressedinthe classification.Excellentagreementlevelswereobtainedbyall
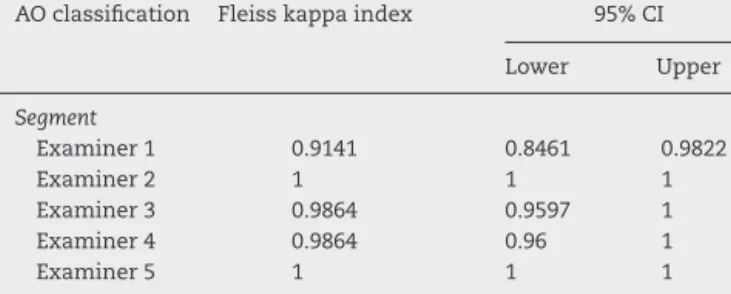
Table2–Statisticalanalysisonintraobserveragreement accordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedin thepediatricAOclassification:inthistable,the segment.CI,confidenceinterval.
AOclassification Fleisskappaindex 95%CI
Lower Upper
Segment
Examiner1 0.9141 0.8461 0.9822
Examiner2 1 1 1
Examiner3 0.9864 0.9597 1
Examiner4 0.9864 0.96 1
Table3–Statisticalanalysisonintraobserveragreement accordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedin thepediatricAOclassification:inthistable,thepaired bone.CI,confidenceinterval.
AOclassification Fleisskappaindex 95%CI
Lower Upper
Pairedbone
Examiner1 0.95 0.8935 1
Examiner2 0.9811 0.9441 1
Examiner3 0.9199 0.8429 0.9918
Examiner4 1 1 1
Examiner5 1 1 1
Table4–Statisticalanalysisonintraobserveragreement accordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedin thepediatricAOclassification:inthistable,the subsegment.CI=confidenceinterval.
AOclassification Fleisskappaindex 95%CI
Lower Upper
Subsegment
Examiner1 0.8467 0.7495 0.9439
Examiner2 1 1 1
Examiner3 0.9890 0.9673 1
Examiner4 0.9483 0.8953 1
Examiner5 0.8685 0.7890 0.9480
Table5–Statisticalanalysisonintraobserveragreement accordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedin thepediatricAOclassification:inthistable,thepattern. CI,confidenceinterval.
AOclassification Fleisskappaindex 95%CI
Lower Upper
Pattern
Examiner1 0.8035 0.7110 0.8959
Examiner2 0.9142 0.8496 0.9788
Examiner3 0.9612 0.9279 0.9945
Examiner4 0.9113 0.8444 0.9781
Examiner5 0.8597 0.7828 0.9367
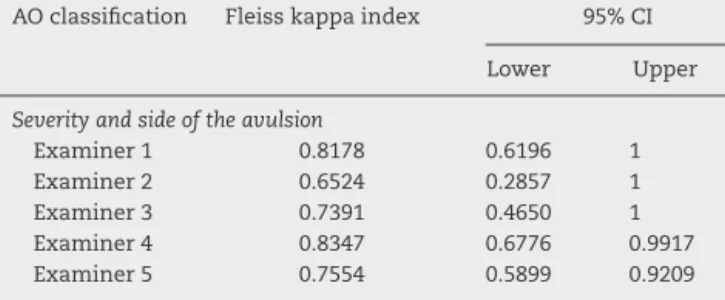
Table6–Statisticalanalysisonintraobserveragreement accordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedin thepediatricAOclassification:inthistable,theseverity andsideoftheavulsion.CI=confidenceinterval.
AOclassification Fleisskappaindex 95%CI
Lower Upper
Severityandsideoftheavulsion
Examiner1 0.8178 0.6196 1
Examiner2 0.6524 0.2857 1
Examiner3 0.7391 0.4650 1
Examiner4 0.8347 0.6776 0.9917
Examiner5 0.7554 0.5899 0.9209
Table7–Statisticalanalysisonintraobserveragreement accordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedin thepediatricAOclassification:inthistable,the displacement.CI,confidenceinterval.
AOclassification Fleisskappaindex 95%CI
Lower Upper
Displacement
Examiner1 0.9068 0.7632 1
Examiner2 1 1 1
Examiner3 0.9524 0.9025 1
Examiner4 0.8779 0.7560 0.9998
Examiner5 0.9361 0.8716 1
theobserversinrelationtotheitemsbone,segment,paired bone,subsegment, patternand displacement.Ontheother hand,theseverityandsideofavulsionpresentedsubstantial agreementforthreeobserversandexcellentfortheothertwo. Lastly,itwasseen thatgreaterobserverexperiencedidnot necessarilyimplyahigherlevelofagreement.
Interobserveragreement
Tables 8–14 show the results from the Fleiss kappa index relatingtotheinterobserveranalysisonthefirstandsecond assessmentsbytheexaminersinvolvedinthisstudy.
Theinterobserveragreementindexwasconsideredtobe excellentfortheitemsofboneandsegmentandsubstantial fortheitemsofpairedboneandsubsegment.Theitem pat-ternshowedmoderateagreementonlyforoneoftheobservers incomparisonwiththeothers,excellentfortwoother exam-iners andsubstantialagreementinthecorrelationbetween theremainingobservers.Lastly,theitemofseverityandside oftheinjurywastheonethatpresentedgreatestdisparityof results.Itreachedanexcellentagreementindexonlyinthe comparativeanalysisbetweentwooftheobservers,whilethe othersrangedfrompoortomoderate,atmost.Onceagain,the resultsdonotallowanycorrelationbetweentheagreement levelsobtainedandtheobservers’experience.
Discussion
ThepediatricAOclassificationisarelativelynewmethodfor groupingandstandardizingthedescriptionsofdifferenttypes oflong-bonefractures inchildren.Inthe orthopedic litera-ture,onlyaverylimitednumberofstudieshaveaddressedthis topic.Thisstimulatedourgrouptoconductthepresentstudy, withtheaimofassessingtheapplicabilityandreproducibility ofthissystemwithinoursetting.
Anidealclassificationsystemshouldconformtoverywell defined criteria, such as being easy to apply, being highly reproducible, having high accuracy, being capable of ade-quatelyguidingthetreatmentandbeingcapableofindicating theprognosisfortheinjuries.2,14–17Inaddition,anideal clas-sification should enable comparisons between the results obtainedfromdifferentseries,andshouldallowbetter doc-umentationofepidemiologicaldata.2
Table8–StatisticalanalysisoninterobserveragreementaccordingtotheFleisskappaindex,describedforeachexaminer andforeachoftheparametersanalyzedinthepediatricAOclassification:inthistable,thebone.CI,confidenceinterval.
Bone Examiner2 Examiner3 Examiner4 Examiner5
Examiner1 1(95%CI:1–1) 1(95%CI:1–1) 1(95%CI:1–1) 0.99(95%CI:0.97–1)
Examiner2 1(95%CI:1–1) 1(95%CI:1–1) 0.99(95%CI:0.97–1)
Examiner3 1(95%CI:1–1) 0.99(95%CI:0.97–1)
Examiner4 0.99(95%CI:0.97–1)
Table9–StatisticalanalysisoninterobserveragreementaccordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedinthepediatricAOclassification:inthistable,thesegment.CI, confidenceinterval.
Segment Examiner2 Examiner3 Examiner4 Examiner5
Examiner1 0.8886(95%CI:0.81–0.96) 0.8886(95%CI:0.81–0.96) 0.86(95%CI:0.77–0.94) 0.83(95%CI:0.74–92)
Examiner2 0.9729(95%CI:0.93–1) 0.9727(95%CI:0.93–1) 0.9457(95%CI:0.89–0.99)
Examiner3 0.9454(95%CI:0.89–0.99) 0.9186(95%CI:0.85–0.98)
Examiner4 0.9453(95%CI:0.89–99)
Table10–StatisticalanalysisoninterobserveragreementaccordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedinthepediatricAOclassification:inthistable,thepairedbone.CI, confidenceinterval.
Pairedbone Examiner2 Examiner3 Examiner4 Examiner5
Examiner1 0.7988(95%CI:0.69–0.91) 0.6593(95%CI:0.52–0.79) 0.95(95%CI:0.89–1) 0.95(95%CI:0.89–1)
Examiner2 0.6439(95%CI:0.51–0.78) 0.8497(95%CI:0.75–0.94) 0.8497(95%CI:0.75–0.94)
Examiner3 0.6510(95%CI:0.52–0.78) 0.6510(95%CI:0.52–0.78)
Examiner4 1(95%CI:1–1)
Table11–StatisticalanalysisoninterobserveragreementaccordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedinthepediatricAOclassification:inthistable,thesubsegment.CI, confidenceinterval.
Subsegment Examiner2 Examiner3 Examiner4 Examiner5
Examiner1 0.8378(95%CI:0.74–0.94) 0.8114(95%CI:0.71–0.91) 0.7977(95%CI:0.68–0.91) 0.6445(95%CI:0.51–0.78)
Examiner2 0.8718(95%CI:0.79–0.95) 0.9585(95%CI:0.90–1) 0.7442(95%CI:0.63–0.86)
Examiner3 0.8318(95%CI:0.74–0.93) 0.7414(95%CI:0.62–0.86)
Examiner4 0.7464(95%CI:0.64–0.86)
Table12–StatisticalanalysisoninterobserveragreementaccordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedinthepediatricAOclassification:inthistable,thepattern.CI, confidenceinterval.
Pattern Examiner2 Examiner3 Examiner4 Examiner5
Examiner1 0.7567(95%CI:0.64–0.87) 0.7118(95%CI:0.60–0.82) 0.7531(95%CI:0.64–0.87) 0.4327(95%CI:0.34–0.53)
Examiner2 0.7117(95%CI:0.59–0.84) 0.8971(95%CI:0.82–0.97) 0.4534(95%CI:0.36–0.55)
Examiner3 0.7486(95%CI:0.63–0.86) 0.4451(95%CI:0.35–0.54)
Examiner4 0.4924(95%CI:0.4–0.59)
Table13–StatisticalanalysisoninterobserveragreementaccordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedinthepediatricAOclassification:inthistable,theseverityandsideof theavulsion.CI,confidenceinterval.
Severityandsideof theavulsion
Examiner2 Examiner3 Examiner4 Examiner5
Examiner1 0.1547(95%CI:–0.7to0.38) 0.4992(95%CI:0.18–0.82) 0.8347(95%CI:0.68–0.99) 0.3286(95%CI:0.09–0.57)
Examiner2 –0.03(95%CI:–0.05to0) 0.27(95%CI:0–0.54) 0.1818(95%CI:0–0.38)
Examiner3 0.4296(95%CI:0.08–0.77) 0.0912(95%CI:–0.07to0.25)
Table14–StatisticalanalysisoninterobserveragreementaccordingtotheFleisskappaindex,describedforeach examinerandforeachoftheparametersanalyzedinthepediatricAOclassification:inthistable,thedisplacement.CI, confidenceinterval.
Displacement Examiner2 Examiner3 Examiner4 Examiner5
Examiner1 0.8160(95%CI:0.67–0.96) 0.7840(95%CI:0.65–0.92) 0.8160(95%CI:0.67–0.96) 0.7584(95%CI:0.61–0.91)
Examiner2 0.7850(95%CI:0.63–0.94) 1(95%CI:1–1) 0.6611(95%CI:0.46–0.86)
Examiner3 0.8056(95%CI:0.66–0.95) 0.6084(95%CI:0.41–0.80)
Examiner4 0.6611(95%CI:0.46–0.86)
classificationforadultsasitsbasis.Thismethodisbasedon analphanumeric system and aimsto categorize the main descriptive elementsofthese fractures,suchastheir loca-tionandtype.11Thisclassificationwasvalidatedinastudy publishedbySlongoetal.,3andstartedtobeusedinstudies conductedbytheauthorswhoconceptualizedit.
Untilthen,eachbodysegmentoftheimmatureskeleton hadbeenstudiedinisolation.Theclassificationofeachbody segment of the immatureskeleton was studied separately andtheclassificationsofthedifferenttypesoffracturewere determinedbyauthorswithparticularinterestineachofthe regionsstudied.Weobservedthatforthisreason,therewasa largenumberofclassificationsforchildhoodandadolescence, guidedbydifferentcriteria.Forexample,wecancitethe sys-temsofPoland,18Bergenfeldt,19Aitken,20SalterandHarris,12 andPeterson21forgrowthplateinjuries.Weareawarethatthis multiplicityofclassificationmethodsisfoundforfractures ofavarietyofsegmentsoftheimmatureskeleton.However, Slongoetal.2emphasizedthatalmostnoneofthesesystems havebeensubjectedtopropervalidationforsubsequent clin-icalapplication.
Independent of the classification method, it is ideally expectedthatthereshouldbeahighlevelofagreementamong the professionalswho use thesemethods. Weobserved in ourstudythatforthevariablesofseverityandpatterninthe AOclassificationsystemforchildren,thelevelofagreement achievedwasloweramongsomeoftheexaminers. Forthe variableofpattern,thereareninesubtypesforthelengthof theepiphysisandsevenforthelengthofthediaphysis. There-fore,wetaketheviewthatthelargenumberofoptionsforeach ofthesevariablesallowseachexaminertohavemorechoices thatcanbemade,andthatthisisindependentofthe exper-tiseand/orexperienceofthoseinvolved.Theinferencethat wecanmakeisthat,despitethelogicoftheclassification sys-temsavailable,asadvocatedbytheirrespectiveauthors,they canbeconsideredtobeverycomplex,regardlessofthe detail-ingofeachcategory.Therefore,thisdidnotallowtheretobe anadequatelevelofconfidencebetweentheobservers,when applied.
Asmallernumber ofoptionsmay alsogeneratea more reliable classificationsystem, but this may not resolvethe problemoftheclassifications,inageneralmanner.For exam-ple,inthestudybySidoretal.,22reductionofthenumberof typesoffractureinordertoapplythemodifiedNeer classifi-cationfortheproximalhumeruswasnotfoundtoprovideany increaseinagreement.
Webelievethat,inageneralmanner,ourstudypresents severalimportantpoints.Firstly,webroughttogetheralarge number of cases (108) that presented great variability of injuries. We observed that other studies presented series
ranginginsizefrom10to275cases.10,14Instudiesinthe lit-eraturethatinvolvedthetypeofanalysisusedinourstudy, therewasanaverageparticipationoffiveevaluatorsforevery 50cases.14Secondly,ourobservershadavarietyoflevelsof experience,whichalsomadeitpossibletoascertainwhether the degreeoflearningmightinterferewiththe application ofthedifferentclassificationsystems. Inourstudy,greater experienceamongtheexaminersdidnotincreasethe agree-mentamongtheitemsevaluated,whichdenotesthatitmay bepossibletomakegeneraluseoftheclassificationsystemfor theentirecommunityoforthopedicsurgeons,independentof theirexperienceofmanagingpediatricfractures.2
Wesupporttheideathatsimplifiedclassificationsystems wouldbeexpectedtopresenthigherlevelsofintraand inter-observeragreementthanwouldthesystemsevaluatedinthis study.Theywouldalsobeexpectedtomoreefficiently pre-dictwhatthebesttreatmentmethodwouldbeandwhattype wouldgiverisetothelowestlatecomplicationrates.Thus, asystemthatencompassesthepredicatesofanideal clas-sificationneedstobeplannedforlong-bonefracturesofthe immatureskeleton.
In this manner, in our opinion, an ideal classification system has notyet been achieved. The complexity of the analysis onfractures that involve thelocomotor apparatus duringchildhoodandadolescenceisdirectlyrelatedtoseveral factors:age;differencesingrowthbetweendifferentbone seg-ments;growth patterns;boneremodelingrates;mechanical actiononthebone;stateoftheadjacentstructures;difference ingrowthratesbetweentheproximalanddistalgrowthplates; growth oftheepiphysis;statusofthecirculation;energyof thetraumainvolved,etc.Theneedforcomprehensionofthe influenceofall thesevariables thatchange withgrowthof thelocomotorapparatusmakescreationofasingleacceptable classificationsystemaverycomplextask.
Conclusions
Inthisstudy,theintraand interobserveragreementforthe pediatricAOclassificationsystemwasconsideredtobegood orexcellentfortheparametersofbone,segment,pairedbone, subsegment, pattern and displacement.However, the intra and interobserver agreement relating to the parametersof severityandsideoftheavulsionwasstatistically unsatisfac-tory.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. MelingT,HarboeK,EnoksenHC.Reliableclassificationof children’sfracturesaccordingtothecomprehensive classificationoflongbonefracturesbyMüller.ActaOrthop. 2013;84(2):207–12.
2. AudigéL,BhandariM,HansonB,KellamJ.Aconceptforthe validationoffractureclassifications.JOrthopTrauma. 2005;19(6):401–6.
3. SlongoT,AudigéL,SchlickeweiW,ClavertJM,HunterJ. DevelopmentandvalidationoftheAOpediatric
comprehensiveclassificationoflongbonefracturesbythe PediatricExpertGroupoftheAOFoundationincollaboration withAOClinicalInvestigationandDocumentationandthe InternationalAssociationforPediatricTraumatology.JPediatr Orthop.2006;26(1):43–9.
4. CantorAB.Sample-sizecalculationsforCohen’skappa. PsycholMethods.1996;1(2):150–3.
5. RosnerBA.Fundamentalsofbiostatistics.4thed.Belmont: DuxburyPress;1995.p.426.
6. FleissJL.Statisticalmethodsforratesandproportion.2nded. NewYork:Wiley;1981.
7. VieraAJ,GarrettJM.Understandinginterobserveragreement: thekappastatistic.FamMed.2005;37(5):360–3.
8. AltmanDG.Practicalstatisticformedicalresearch.3rded. London:ChapmanandHall;1995.p.403–9.
9. LandisJR,KochGG.Themeasurementofobserveragreement forcategoricaldata.Biometrics.1977;33(1):159–74.
10.SlongoT,AudigéL,ClavertJM,LutzN,FrickS,HunterJ.The AOcomprehensiveclassificationofpediatriclong-bone fractures:aweb-basedmulticenteragreementstudy.JPediatr Orthop.2007;27(2):171–80.
11.MüllerM,NarzarianS,KochP,SchatzkerJ.The
comprehensiveclassificationforfracturesoflongbones. Berlin;Heidelberg;NewYork:Springer-Verlag;1990.
12.SalterRB,HarrisWR.Injuriesinvolvingtheepiphysealplate.J BoneJointSurgAm.1963;45(3):587–622.
13.GartlandJJ.Managementofsupracondylarfracturesofthe humerusinchildren.SurgGynecolObstet.1959;109(2):145–54. 14.AudigéL,BhandariM,KellamJ.Howreliablearereliability
studiesoffractureclassifications?Asystematicreviewof theirmethodologies.ActaOrthopScand.2004;75(2):184–94. 15.GarbuzDS,MasriBA,EsdaileJ,DuncanCP.Classification
systemsinorthopaedics.JAmAcadOrthopSurg. 2002;10(4):290–7.
16.BursteinAH.Fractureclassificationsystems:dotheywork andaretheyuseful?JBoneJointSurgAm.1993;75(12):1743–4. 17.MartinJS,MarshJL.Currentclassificationoffractures.
Rationaleandutility.RadiolClinNorthAm. 1997;35(3):491–506.
18.PolandJ.Traumaticseparationoftheepiphysis.London: Smith,Elder&Co;1898.p.144–62.
19.BergenfeldtE.BeitragezurKenntnisdertraumatischen EpiphysenlosungenandenlangenRohrenknochender Extremitaten:eineklinisch-rontgenologischeStudie.Acta ChirScand.1933;73Suppl.28.
20.AitkenAP.Theendresultofthefractureddistaltibial epiphysis.JBoneJointSurg.1936;18(3):685–91.
21.PetersonHA.Physealfractures.Part3:Classification.JPediatr Orthop.1994;14(4):439–48.