w w w . r b o . o r g . b r
Original
Article
Reproducibility
of
the
Tronzo
and
AO
classifications
for
transtrochanteric
fractures
夽
Carlos
Augusto
Mattos,
Alexandre
Atsushi
Koza
Jesus,
Michelle
dos
Santos
Floter,
Luccas
Franco
Bettencourt
Nunes
∗,
Bárbara
de
Baptista
Sanches,
José
Luís
Amim
Zabeu
HospitaleMaternidadeCelsoPierro,PontifíciaUniversidadeCatólicadeCampinas(PUC-Campinas),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6August2014 Accepted23September2014 Availableonline15August2015
Keywords:
Hipfractures Femoralneck
fractures/classification Testreproducibility
a
b
s
t
r
a
c
t
Objective:To analyze the reproducibility of the Tronzo and AO classifications for transtrochantericfractures.
Method:Thiswasacross-sectionalstudyinwhichtheintraobserverandinterobserver con-cordancebetweentworeadingsmadeby11observerswasanalyzed.Theanalysisofthe variationsusedthekappastatisticalmethod.
Results:ModerateconcordancewasfoundinrelationtotheAOclassification,whileslight concordancewasfoundfortheTronzoclassification.
Conclusion: ThisstudyfoundthattheAO/Asifclassificationfortranstrochantericpresented greaterintraandinterobserverreproducibilityandthatgreaterconcordancewascorrelated withgreaterexperienceoftheobservers.Withoutdivisionintosubgroups,theAO/Asif clas-sification wasshown,asdescribedintheliterature, tobeacceptable forclinicalusein relationtotranstrochantericfracturesofthefemur,althoughitdidnotshowabsolute con-cordance,giventhatitsconcordancelevelwasonlymoderate.Nonetheless,itsconcordance wasbetterthanthatoftheTronzoclassification.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Reprodutibilidade
das
classificac¸ões
de
Tronzo
e
AO
para
fraturas
transtrocanterianas
Palavras-chave:
Fraturasdoquadril Fraturasdocolo femoral/classificac¸ão Reprodutibilidadedostestes
r
e
s
u
m
o
Objetivo:Analisar a reprodutibilidade das classificac¸ões AO e de Tronzo para fraturas transtrocanterianas.
Método:Estudotransversalqueanalisouaconcordânciaentreduasleiturasfeitaspor11 observadores,intraobservadoreseinterobservadores.Aanálisedasvariac¸õesusouométodo estatísticoKappa.
夽
WorkperformedintheOrthopedicsandTraumatologyService,HospitaleMaternidadeCelsoPierro(PUC-Campinas),Campinas,SP, Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](L.F.B.Nunes).
http://dx.doi.org/10.1016/j.rboe.2015.08.002
Resultados: Verificou-se concordância moderada para a classificac¸ão AO enquanto a classificac¸ãoTronzomostrouconcordâncialeve.
Conclusão: Otrabalhoevidencioumaiorreprodutibilidadeda classificac¸ãoAO/Asifinter eintraobservadorparaasfraturastranstrocanterianasdefêmur,oquetemrelac¸ãocom oaumentoda predominânciade concordânciacomaexperiência dosobservadores. A classificac¸ãoAO/Asifsemdivisãoemsubgruposmostrou-se,assimcomodescritona liter-atura,aceitaparaousoclíniconasfraturastranstrocanterianasdefêmur.Noentanto,não mostrouconcordânciaabsoluta,umavezqueseuníveldeconcordânciaéapenasmoderado, massuperiorquandocomparadacomaclassificac¸ãoTronzo.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Transtrochantericfracturesareextracapsularandare charac-terizedasoccurringintheareabetweenthegreaterandlesser trochantersofthefemur.1Thisareaofthefemuris predomi-nantlyspongyandvascularized.
Elderlypatientsaremorevulnerabletothis typeof frac-turebecauseoftheirbonefragility.Inthesepatients,falling tothegroundisarelativelycommonmechanism.1,2 In sur-veysconducted between1941and 1971 thatwere cited by DeLee,3itwasnotedthatpatientswithtranstrochanteric frac-tureswereonaverage10–12yearsolderthan patientswith fracturesofthefemoralneck(whichareintracapsular),with ameanbetween66and76years.Itwasalsonotedthatcases amongfemalespredominatedovercasesamongmales,with ratiosof2:1–8:1.
Transtrochantericfracturesalsoaffectyoungadults, espe-cially through mechanisms of high-energy trauma.1 The incidenceofthesefracturesisincreasing,alongwiththecosts involvedintreatingthem.InBrazil,inasurveyconductedby theMinistryofHealth,itwasobservedthat90%ofthe finan-cialresourcesdestinedfororthopedicdiseasesareconsumed byninediseases,andtranstrochantericfractureswereoneof these.4
Another problem that is faced is that one-third of the patients diewithin the first year afterthe injury and that approximately50%ofthepatientsbecauseincapableof walk-ingaloneorgoingupstairs,and20%requirefull-timehome care.5
Theprincipalmethodforpreciselydeterminingthe diagno-sisofthesefracturesisradiography,butshorteningofthelimb anditspositioninginexternalrotationareimportantclinical findingsthatcorroboratethediagnosisofthistypeofinjury.6 Thetreatmentissurgicalandinvolves useofplates witha sliding screw,cephalomedullarynails or fixed-angleplates, withaviewtoachievingpatientrehabilitationasquicklyas possible.6
Thereareseveralclassificationsystemsfor transtrochan-tericfractures.However,themaincharacteristicofa classi-fication system isthat it should containvalid information that helps to describe the nature of the fracture, such as topography,configurationofthefracture,degreeofstability and severity.Another characteristicisthatit shouldaid in planningforosteosynthesisandinpredictingtheprognosis
afterdefinitivesynthesis,withtheobjectiveofachieving sta-bleanatomicalprimaryreduction.2,7Itisalsoimportantthat anyclassificationsystemshouldbereproduciblebetween dif-ferentobserversandalsobythesameobserverondifferent occasions.7
TheTronzoclassificationfortranstrochantericfractures8 wascreated in1974andisstillonethesystemsmostused today.ItwasbasedontheclassificationofBoydandGriffin,9 whoclassifiedfracturesaccordingtothepossibilityof achiev-ing and maintainingreduction(fourtypes: I–stableintwo parts;II–unstableandcomminutive;III–unstableandreverse oblique;andIV–intertrochanteric–subtrochantericwithtwo fractureplanes).In1949,Evans7classifiedfracturesafter sur-gicaltreatmentasstableorunstable.
Tronzo8 (Fig. 1) modified the classification of Boyd and Griffin,9andthisresultedinfivetypes.Thisclassification sys-temisgreatlyusedtoday.
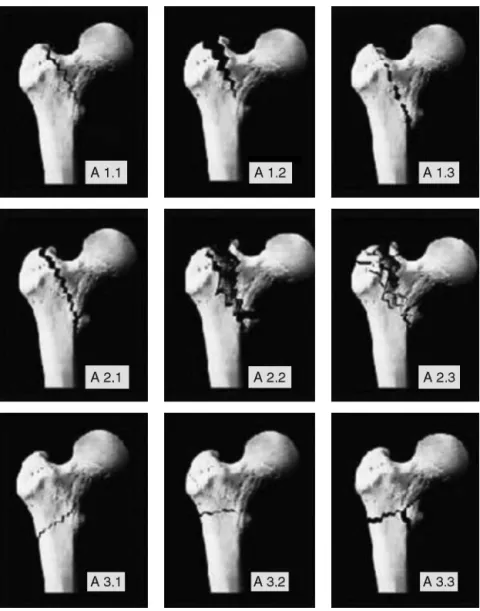
The AO (Arbeitsgemeinschaft für Osteosynthesefragen) classification10,11wasinitiallycreatedbyMülleretal.10inthe 1980sandhasperiodicallyundergoneupdateswiththeaimof standardizingtheclassificationoffracturesforworldwide cov-erage,throughasystemforlocatingtheboneandthetypeof involvement(letterandnumber),suchthatanalphanumeric code would makeit possiblefor professionalsto promptly know what hadhappened, whichwould facilitate commu-nication between orthopedicservices. For this reason, this systemistheonecurrentlymostusedinstudies.Inthis sys-tem,trochantericfracturesarerepresentedbycode31-A.They aresubdividedintothreegroupsbaseontheobliquityofthe fracturelineandthedegreeofdamage(bonefragmentation).11 Group1presentsafracturelinethatstartsinanyregion ofthegreatertrochanterandextendsasfarasapointabove orbelowthelessertrochanter.Thereareonlytwofragments andthemedialcortexisfracturedinonlyonelocality.These fracturesarestableafterreductionandfixation,sincethereis goodcontactbetweenthefragments,withoutboneloss.The lessertrochanterisintact.11
Fig.1–Tronzoclassification.
Group 3 presents a fracture line that crosses the intertrochantericregion,abovethelessertrochantermedially andbelowthecrestofthevastuslateralisinthelateralregion. Thelineaffectsbothcorticesandhasthecharacteristicsof reverseobliquity.3
Thisclassificationalsodividesthegroupsintothree sub-groups,butinthepresentstudy,onlythegroups31-A1,31-A2 and31-A3(Fig.2)areused,giventhatfracturesofthesame subgrouppresentsimilarbiomechanicalbehavior.
The objective of this study was to evaluate the repro-ducibilityoftheAO/ASIFclassificationwithoutdivisioninto subgroupsandtheTronzoclassification,fortranstrochanteric fractures,bymeansofconcordanceanalysisbetweenpairsof readingsmadebyobserversatdifferentstagesoftraining.
Materials
and
methods
Fiftypreoperativeradiographsinanteroposterior(AP)and lat-eral views on patients with diagnoses oftranstrochanteric fracturesofthefemurthatoccurredbetweenJanuary2012and December2012wereselected.Alloftheseindividualswere skeletallymature(overtheageof20years).
Patients with previous pathological conditions in their limbsthat possiblymodified the normalanatomy, such as previousfracturesinthecoxofemoralregion,malformations, infections and bone tumors were excluded from the case selection.Fromthesedata, amultiple-choicequestionnaire
Table1–Classificationofthestrengthofconcordance accordingtothekappacoefficient.
Kappacoefficient Strengthofconcordance
Lessthanzero Poor
0.00–0.20 Negligible
0.21–0.40 Low
0.41–0.60 Moderate
0.61–0.80 High
0.81–1.00 Almostperfect
Table2–Kappaindex,standarderrorandconcordance betweenthetworeadingsatdifferenttimes,fortheAO classification.
Comparisonbetween thereadings
Kappa SE Concordance
O1Avs.O1B 0.71 0.09 High
O2Avs.O2B 0.48 0.12 Moderate
O3Avs.O3B 0.13 0.11 Negligible
O4Avs.O4B 0.77 0.08 High
O5Avs.O5B 0.65 0.10 High
O6Avs.O6B 0.24 0.08 Low
O7Avs.O7B 0.71 0.10 High
O8Avs.O8B 0.41 0.11 Moderate
O9Avs.O9B 0.43 0.10 Moderate
O10Avs.O10B 0.71 0.09 High
O11Avs.O11B 0.64 0.10 High
O1toO11,observers;A,firstreading;B,secondreading;SE,standard error.
wasformulatedinordertoclassifythefracturesaccordingto theAOsystem(31.A1,31.A2and31.A3,withoutthesubgroups ofeachdivision)(Table1)andaccordingtotheclassification ofTronzo(1973)8(Table2).Aspacewasprovidedbeloweach figureand,foreachcolumn,onlyoneresponsewastobe indi-cated.
Elevenphysicianswerechosen.Amongthese,threewere first-yearresidents,threewerethird-yearresidentsofa med-icalresidencyprogramonorthopedicsandtraumatology,two wereorthopedistswithspecialisttitleswithupto5yearsof experienceandthreewereorthopedistswithspecialisttitles withmorethan5yearsofexperience.Thesephysicianswere identifiedsequentiallywithnumbersfrom1to11.Allthe eval-uatorsworkedinthesame orthopedicsserviceatatrauma referral hospital.Theclassificationswere reviewedwith all the participants individually, before the questionnaire was applied.
The radiographs were analyzed independently, without contactbetweentheevaluators,underidenticalconditionsfor alloftheseobservers.Therewasnotimelimitforanswering thequestionnaire.
Onemonthlater,thesameobserversevaluatedthesame radiographs,without anyknowledgeofwhattheresponses theymadepreviouslywere,oranyknowledgeofthedatafrom theotherevaluators.Noneoftheobservershadaccesstothe datarelatingtothesurgicaltreatmentoneachfracture.
Fig.2–AOclassificationaccordingtosubgroups.
observersbymeansofpairedanalyses.Theobserved propor-tionsofconcordancebetweentheobservers(Po)andwithin theobserverswerecompared.Thesevaluescouldvaryfroma resultoflessthan0(poor)to1(almostperfect).
Results
Theobservers analyzed 50 preoperative radiographs in AP andlateralviews,ontranstrochantericfracturesofthefemur andcategorizedthefracturesinaccordancewiththeAOand Tronzoclassifications.Eachobservermadetwoanalyseswith a1-monthintervalbetweenthem,withoutknowledgeofthe previous results and without priorcontact with the other observers.Theresultswereanalyzedbymeansofthekappa methodandtheresultsrelatingtothestrengthoftheintraand interobserver concordance were subdivided into six levels. Kappaindexvalueslessthan0wereclassifiedaspresenting poorstrengthofconcordance;valuesfrom0to0.2as negligi-ble;0.21to0.40aslow;0.41to0.60asmoderate;0.61to0.80as high;and0.81to1.0asalmostperfect.
Thepresentationofthekappaindex,standarderror(SE) and concordancebetweenthetworeadingsoftheAO/ASIF classificationmadebythe11observersattwodifferenttimes (Table2)showedthattheSErangedfrom0.9to1.2andthe kappaindexfrom0.13to0.77,withpredominanceinthe mod-eratetohighgroupofstrengthofconcordance(Fig.3).
Thepresentationofthekappaindex,SEandconcordance betweenthetworeadingsoftheTronzoclassificationmadeby
Kappa from AO classification
Table3–Kappaindex,standarderrorandconcordance betweenthetworeadingsatdifferenttimes,forthe Tronzoclassification.
Comparisonbetween thereadings
Kappa SE Concordance
O1Avs.O1B 0.26 0.08 Low
O2Avs.O2B 0.59 0.09 Moderate
O3Avs.O3B – – NA
O4Avs.O4B 0.55 0.08 Moderate
O5Avs.O5B 0.5 0.08 Moderate
O6Avs.O6B 0.24 0.08 Low
O7Avs.O7B 0.51 0.08 Moderate
O8Avs.O8B 0.22 0.08 Low
O9Avs.O9B – – NA
O10Avs.O10B 0.35 0.08 Low
O11Avs.O11B 0.26 0.08 Low
O1toO11,observers;A,firstreading;B,secondreading;SE,standard error.NA,notapplicablebecauseoftheasymmetryofthedata.
the11observersattwodifferenttimes(Table3)showedthat theSErangedfrom0.08to0.09andthekappaindexfrom0.22 to0.59.Twoobserverscouldnotbeincludedbecauseofgreat asymmetryofthe dataatthe two differentdata-gathering times.Thestrength ofconcordancewaspredominatelylow tomoderatefortheTronzoclassification(Fig.4).
The kappa index analysis comparing the two different readingsfortheAOandTronzoclassifications,madebythe observersatdifferenttimes,showedthatfortheAO classifi-cationthekappaindexwas0.53withSEof0.03,i.e.showing moderateconcordance.Ontheotherhand,theTronzo classifi-cationshowedakappaindexof0.36andSEof0.03,i.e.showing fairconcordance.
Theanalysis andcomparisonwere performedusingthe same statistical method, which correlated the observers accordingtotheirjobpositionsandexperience(Table4).Inthe analysisontheAOclassification,highkappaindexesand con-cordancewereseenamongthemoreexperiencedobservers, i.e.thosewithmorethan5yearssincecompletionof train-ing and those who had completed their training less than 5yearsago.Theobserverswhoweremedicalresidents pre-sentedlowervalues(Table4).
Thesameanalysisonthekappaindex,standarderrorand predominanceofconcordanceaccordingtojobpositionand experienceamongtheobserverswasperformedontheTronzo classification,asshowninTable5.
Kappa from Tronzo classification
Fig.4–Variationininterobserverkappaindexfromusing theTronzoclassification.
Table4–AOclassification,jobposition,kappaindex, standarderrorandconcordance.
Jobposition Comparison
betweenthe readings
Kappa SE Concordance
S>5y O1Avs.O1B 0.71 0.09 High
S>5y O11Avs.O11B 0.64 0.1 High
S>5y O7Avs.O7B 0.71 0.1 High
S<5y O4Avs.O4B 0.77 0.08 High
S<5y O5Avs.O5B 0.65 0.1 High
R3 O10Avs.O10B 0.71 0.09 High
R3 O2Avs.O2B 0.48 0.12 Moderate
R3 O8Avs.O8B 0.41 0.11 Moderate
R1 O9Avs.O9B 0.43 0.1 Moderate
R1 O6Avs.O6B 0.24 0.08 Low
R1 O3Avs.O3B 0.13 0.11 Negligible
O1toO11,observers;A,firstreading;B,secondreading;SE,standard error.
S>5y,specialistwithmorethan5yearsofexperiencesince train-ing;S<5y,specialist withlessthan5yearsofexperiencesince training.
R3,third-yearresident;R1,first-yearresident.
Discussion
Allfractureclassificationsystemshavetheobjectivesof guid-ingthetreatment,aidinginsurgicalplanningandhavingthe capacitytobereproducedwithhighconcordancebydifferent observersindifferentsituations.Thekappastatisticalsystem hasthecapabilitytonumericallytransmittherealcapacityof fractureclassificationsystems.
Schipperetal.12 studiedtheAOclassificationsystemfor transtrochantericfracturesofthefemurusing20X-rayimages thatwereanalyzedby15observers.FromtheAOclassification withsubgroups, theyreportedamean intraobserver kappa
Table5–AnalysisontheTronzoclassificationsystemin relationtotheobservers’experience.
Jobposition Comparison
betweenthe readings
Kappa SE Concordance
S>5y O1Avs.O1B 0.26 0.08 Low
S>5y O11Avs.O11B 0.26 0.08 Low
S>5y O7Avs.O7B 0.51 0.08 Moderate
S<5y O4Avs.O4B 0.55 0.08 Moderate
S<5y O5Avs.O5B 0.5 0.08 Moderate
R3 O10Avs.O10B 0.35 0.08 Low
R3 O2Avs.O2B 0.59 0.09 Moderate
R3 O8Avs.O8B 0.22 0.08 Low
R1 O9Avs.O9B – – NA*
R1 O6Avs.O6B 0.24 0.08 Low
R1 O3Avs.O3B – – NA*
R1 O3Avs.O3B 0.13 0.11 Negligible
O1toO11,observers;A,firstreading;B,secondreading;SE,standard error.
S>5y,specialistwithmorethan5yearsofexperiencesince train-ing;S<5y,specialist withlessthan5yearsofexperiencesince training.
indexvalueof0.48andaninterobservervalueof0.33.From theAOsystemwithoutsubgroups, theintraobserver kappa valuewas0.78andtheinterobservervaluewas0.67.A previ-ousstudyonfivepatientswithtranstrochantericfracturesof thefemuralsoconcludedthatusingtheAOclassificationwas unreliable.13
Neweyetal.14reportedthatthealphanumericsystemof theAOclassificationwasunnecessarilycomplicatedandthat itsuseinclinicalpracticefellshortofwhatwouldbedesirable andmadelittlecontributiontowardsurgicalplanning.
AccordingtoPervezetal.,2theresultsobtainedfromtheir studyconfirmedthatboththeAO/ASIFandtheJensen classi-ficationsystemwereunacceptable.
However,whentheAO/ASIFsystemwasdividedintoonly threegroups(31A1,31A2and31A3),itbecameacceptable.For thosewhofindthealphanumericterminologyconfusing, Per-vezetal.2recommendedthatthesegroupsshouldbenamed stabletrochantericfracture(31A1),unstabletrochanteric frac-ture(31A2)andtrochantericfracturewithreverseline(31A3). InastudythatcomparedtheAO/ASIFandJensen classi-fications,VanEmbdenetal.15foundthattheAOsystemhad poorreliabilityandtheJensensystemhadmoderatereliability. Theyconcludedthattherewasaneedtocreateanew classi-ficationortoimprovetheexistingclassificationsinorderto achievebettercategorizationandtreatmentproposals.
Wedidnotfindanystudiesintheliteraturethatanalyzed thereproducibilityoftheTronzoclassification.
Wefoundthatthemeanintraobserverkappaindexforthe AOclassificationwas0.53(0.13–0.71),withpredominanceof moderatetohighconcordance.Therewasgreatinequalityin the analysisin relationtothe job positionand experience ofthe observer,such thathigh concordancepredominated amongtheprofessionalswhohadalreadyachievedthetitle ofspecialist, withakappaindexof0.696 (range:0.64–0.77) andstandarderrorof0.8–1.Inouranalysisontheresidents (bothatR1 and atR3 level), therewas lower concordance, suchthatthemean kappaindexwas0.4(range:0.13–0.71), withpredominanceoflowconcordanceandastandarderror of0.8–1.2.
ThemeanintraobserverkappaindexfortheTronzo clas-sificationwas0.31,withpredominance oflowtomoderate concordance.Ontheotherhand,inrelationtotheAO/ASIF system, comparison of the job position and experience of theobserversshowedthatthekappaindexwas0.416forthe observers who already had specialist titles, with predomi-nanceofmoderateconcordance,whilethekappaindexwas 0.23forthelessexperiencedobservers.Inthegroupofless experiencedobservers,itshouldbehighlightedthatthedata gatheredin relationto the Tronzo systemby twoof these observerscould notbeincluded intheanalysisbecause of greatasymmetryofthedatafromonereadingtotheother.
Conclusion
Wefound that higher concordance predominated inusing theAO/ASIFclassification,inrelationtotheTronzo classifi-cation,bothinintraandinterobservercomparisons.Wealso observedthat in relationto bothclassifications, therewas
higherconcordanceamongthemoreexperiencedobservers (physicianswithspecialisttitles)thanamongtheless experi-encedobservers(residents).
ThepredominantconcordancelevelintheAO/ASIFsystem withoutdivisionswasonlymoderate,andthiswas compat-ible withstudiesfoundinthe literature.In thecaseofthe Tronzoclassification,lowconcordancewasfoundto predom-inate. TheAO/ASIFclassificationsystem wascharacterized asacceptableforclinicalpractice,albeitimperfect,giventhe higherconcordanceamongobserverswithgreaterexperience.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ThomasRusselA.Fraturasintertrocantéricas.In:BucholzRW, HeckmanJD,Court-BrownCM,TornettaPIII,McQueenMM, RicciWM,editors.FraturasemadultosdeRockwoodeGreen. 7thed.Barueri:Manole;2013.p.1597–640.
2.PervezH,ParkerMJ,PryorGA,LutchmanL,ChirodianN. Classificationoftrochantericfractureoftheproximalfemur: astudyofthereliabilityofcurrentsystems.Injury.
2002;33(8):713–5.
3.DeLeeJC.Fracturesanddislocationsofthehipinfractures. In:RockwoodCAJr,GreenDP,editors.Fracturesinadults.2nd ed.Philadelphia:JBLippincott;1984.
4.DaniW,AzevedoE,Fraturastranstrocanterianas:elementos básicosdiagnósticos.RBM[online].Availablefrom:http:// www.moreirajr.com.br/revistas.asp?fase=r003&idmateria= 3245
5.LimaALP,AzevedoAJ,AmaralNP,FranklinCE,GiordanoV. Tratamentodasfraturasintertrocanterianascomplacae parafusodeslizante.RevBrasOrtop.2003;38:271–9.
6.CantoRST,SakakiM,SusukiI,TucciP,BelangeroW,Kfuri JúniorM,etal.Fraturatranstrocanteriana.In:Projeto Diretrizes.SãoPaulo:SociedadeBrasileiradeOrtopediae Traumatologia;2007.
7.EvansEM.Thetreatmentoftrochantericfracturesoffemur.J BoneJointSurgBr.1949;31(2):190–203.
8.TronzoRG.Symposiumonfracturesofthehip.Special considerationsinmanagement.OrthopClinNorthAm. 1974;5(3):571–83.
9.BoydHB,GriffinLL.Classificationandtreatmentof trochantericfractures.ArchSurg.1949;58(6):853–66.
10.MüllerME,NazarianS,KochP,SchatzkerJ.The
comprehensiveclassificationoffracturesofthelongbones. NewYork:Springer-Verlag;1990.
11.JensenJS.Classificationoftrochantericfractures.ActaOrthop Scand.1980;51(5):803–10.
12.SchipperIB,SteyerbergEW,CasteleinRM,VanVugtAB. ReliabilityoftheAO/ASIFclassificationforpertrochanteric femoralfractures.ActaOrthopScand.2001;72(1):36–41.
13.DeBoeckH.Classificationofhipfractures.ActaOrthopBelg. 1994;60Suppl.1:106–9.
14.NeweyML,RickettsD,RobertsL.TheAOclassificationoflong bonefractures:anearlystudyofitsuseinclinicalpractice. Injury.1993;24(5):309–12.