Revista de Saúde Pública
I SSN 0034- 8910 versão im pressa
Rev Saúde Pública 2004; 38(1)
Maternal com plications associated with type of delivery in a
university hospital
Roseli Mieko Yam am ot o Nom ura, Eliane Aparecida Alves and Marcelo Zugaib
Clínica Obst ét r ica do Hospit al das Clínicas da Faculdade de Medicina da Universidade de São Paulo. São Paulo, SP, Brasil
ABSTRACT
Objective
To analy ze m at er nal com plicat ions associat ed t o t y pe of deliv er y , com par ing cesar ean ( c - ) sect ion w it h v aginal delivery.
M ETHODS
Ret r ospect iv e st udy of 1,748 deliv er ies car r ied out at a univ er sit y hospit al in t he cit y of São Paulo, Sout heast ern Brazil, in w hich t he new born w eighed m ore t han 500 g. Mat ernal com plicat ions occurred dur ing deliv er y as w ell as t hose diagnosed during puerperium t hat required furt her hospit al adm ission w er e analy zed. St at ist ical analy ses included St udent ’s t t est and Fisher ’s Ex act t est . Significance lev el w as set at 0 . 0 5 .
C- sect ions were perform ed on 988 pat ient s ( 56.5% ) . Hem orrhagic com plicat ions occurred in 1.2% of c - sect ions and in 0.8% of nor m al deliver ies, w it h no st at ist ically significant differ ence bet w een bot h groups. Endom et rit is was observed in 0.4% of c- sect ions and in 0.1% of vaginal deliveries, w it hout st at ist ically significant differ ence. Tw o cases of puer per al infect ion ev olv ed t o hy st er ect om ies, in t he c - sect ion gr oup. Ther e w er e no m at er nal deat hs r elat ed t o c - sect ion.
CONCLUSIONS
No associat ions w ere found bet w een m at ernal com plicat ions and t ype of delivery in t he period analyzed.
KEYWORD S
Cesar ean sect ion. Labor com plicat ions. Par t ur it ion. Puerperal infect ion. Puerperal com plicat ions.
INTRODUCTION
I n t he last few years, Brazil has had one of t he hig h est r at es of caesar ian ( c - ) sect ion deliv er y w orldw ide. This is relat ed t o a num ber of fact ors, w hich involve, m ainly, recent im provem ent s in sur gical and anest het ic t echniques, gr eat er av ailabilit y of pr opaedeut ic r esour ces t hat det ect r isk for t h e f et u s, t he incr ease in t he incidence of pr egnancies in pat ient s w it h pr ior c - sect ions, and sociocult ur al fact or s r elat ed t o t he gr eat er pr act icalit y of pr ogr am m ed deliv er y .1 1 Obviously, any sur gical pr ocedur e includes a level of r isk inher ent t o t he act it self. How ev er , t he possibilit y of av oiding a c- sect ion in em ergency sit uat ions, due t o m at ernal or fet al risk, has st im ulat ed discussions, sin ce cer t ain cir cu m st an ces su ggest elect iv e c- sect ions as an opt ion in t he cont ex t of t he dialog est ablished bet w een obst et r ician and pat ient .1 0
I n a st udy published in 1999, Belizán et al1 ( 1999) report a grow ing increase in c- sect ion r at es in a num ber of Lat in- Am erican count ries, especially Chile, wit h 40% and Brazil, wit h 27.1% ( 1994- 96) . How ev er , accor ding t o gov er nm ent al st at ist ics pr ov ided by t he Sist em a de I nfor m ações dos Nascidos Viv os ( Live - birt h I nform at ion Syst em - SI NASC) ,9 t h e c- sect ion r at e in 2000 in t he st at e of São Paulo was as high as 48.4% .
I n high- risk pregnancies, com plicat ions m ay frequent ly require t he prem at ure int errupt ion of gest at ion, producing an increase in c - sect ion r at es. The pr esent sur v ey w as conduct ed in an obst et r ical clinic of a univ er sit y hospit al. I n a univ er sit y env ir onm ent , t he pr ocedur es adopt ed t end t o follow pre- est ablished pr ot ocols,1 7 in which indicat ions for surgical procedures are based m ainly on t he clinical and obst et r ical aspect s of each case, in an at t em pt t o m inim ize c - sect ion incidence.
M ETHODS
The sur v ey w as car r ied out in t he obst et r ical clinic of a univ er sit y hospit al in t he cit y of São Paulo, char act er ized by it s st at us as a r efer ence cent er for sev er e cases, t hus r eceiv ing a significant body of high- r isk pat ient s w it h int er cur r ent clinical and obst et r ic condit ions. The pr ofile of t his populat ion incr eases t he r isk of abnor m al occur r ences dur ing pr egnancy and labor , as w ell as t he r isk of fet al suffering, t hus increasing t he proport ion of c - sect ion s.
Bet w een 1 Apr il and 31 Decem ber 2001, 2,410 pat ient s were adm it t ed t o t he facilit y. Early in 2001 a com put erized program designed t o st ore in- and out pat ient per sonal and clinical dat a, including dat a relat ed t o t he newborn, was im plem ent ed in t he clinic. Adm ission files in t he pat ient ’s m edical r ecor ds, as w ell as deliv er y files and dischar ge r epor t s w er e pr int ed using t his soft w ar e. I n or der t o ensur e t he effect iv e inclusion of all deliv er ies car r ied out in t his clinic, elect r onic dat asheet s w er e check ed on a m ont hly basis, com paring dat a from t he soft ware wit h t he delivery regist rat ion j ournal, kept by t he nur sing ser vice of t he obst et r ics clinic. Dur ing t he per iod analyzed, a t ot al 1,748 deliver ies were carried out in which t he newborn weighed m ore t han 500 g. Dat a were analy zed r et r ospect iv ely based on t he inst it ut ion’s dat abase.
Clinical diagnoses m ost frequent ly observed am ong t he populat ion analyzed are present ed in Table 1.
Table 1 – Most frequently observed clinical diagnoses in gravida population.
Diagnosisóstico N %
Hypertensive syndromes 307 17.6 Premature amniorrhexis 177 10.1
Diabetes 168 9.6
Cardiopathies 126 7.2
Infections 123 7
Fetal malformations 111 6.4
A large num ber of ot her diagnoses were observed wit h lesser frequency. 357 pregnant wom en did not pr esent int er cur r ent clinical or obst et r ic condit ions, or 20.4% of t he analyzed populat ion.
Mat ernal age varied bet w een 12 and 44 years, w it h m ean age 27.6 years, 6.9 years st andard deviat ion and 27.1 year s m edian value. I n t er m s of obst et r ical hist or y, 694 were nulliparae, or 39.7% of cases. Ant enat al car e w as pr ov ided at t he sam e healt h facilit y for 1,173 pat ient s ( 67% ) .
Due t o it s being a universit y hospit al, m ost surgical procedures in t he inst it ut ion are perform ed by r esident t r ainee st udent s, under dir ect super v ision of assist ant doct or s belonging t o t he depar t m ent ’s clinical t eam . Accor ding t o t his classificat ion, 1,706 deliv er ies w er e done by r esident t r ainees, or 97. 6% of analy zed cases.
Clinical and/ or obst et rical indicat ions for t he t erm inat ion of gest at ion by c - sect ion ar e list ed in Table 2.
Table 2 – Clinical and/or obstetric indications leading to c-sections.
Indications for c-section N %
Fetal suffering 207 21
Labor dy st ocia 123 12.5
Severe maternal pathology 87 8.8
Meconium in amniotic fluid 75 7.6
Fetal-pelvic disproportion 61 6.2
Breech present at ion 52 5.3
Oligohydramnion 45 4.6
Twin gestation 33 3.3
Fetal Malformation 31 3.1
Intra-uterine growth restriction 21 2.1
Maternal HIV infection 21 2.1
Premature membrane rupture 15 1.5
Premature placental detachment 10 1 Other diagnoses with frequencies below 1.0% 33 3.3
*Characterized as the c-section performed when the patient presented a history of two or previous more c-sections
The condit ions list ed in Table 2 cor r espond t o t hose consider ed t o be t he m ain indicat ion for t he c-sect ion in each case, ev en if m or e t han one pr oblem w as diagnosed. The occur r ence of m at er nal com plicat ions in cases in w hich c- sect ions w ere perform ed w as com pared t o t ha t of cases of v aginal delivery ( norm al or forceps) . Com plicat ions st udied included t hose occurred during t he surgical pr ocedur e, as w ell as t hose occur r ed dur ing puer per ium t hat r equir ed r ehospit alizat ion. The infect ious com plicat ion invest igat ed w as puerp eral infect ion, defined as t he infect ion originat ed in t he genit al appar at us aft er r ecent deliv er y . Endom et r it is w as char act er ized as an infect ion of t he placent al im plant at ion sit e w it h concom it ant fever and pain, soft ening, and insufficient involut ion of t he ut er us, r equir ing t r eat m ent w it h specific ant ibiot ic t her apy. Abdom inal w all infect ion at t he sit e of sur gical incision w as only consider ed in t his analy sis in case t her e w as t he need for r ehospit alizat ion for rest it ching purposes. Hem orrhagic consequences analy zed included t he occur r ence of hy pot onic m yom et r ium or ut er ine at ony in w hich excessive bleeding and inefficient cont r act ilit y of t he ut er us required supplem ent ary int ravenous/ int ram uscular oxyt ocin adm inist rat ion and ut erine m assage. Placen t a accr et a w as char act er ized w hen placent al v illi w as at t ached t o t he m y om et r ium , w it h abnorm ally firm adherence t o t he ut erine wall. I n at t em pt ing at m anual det achm ent , part ial or t ot al absence of a cleav age w as obser v ed.
Quant it at iv e v ar iables w er e analy zed descript ively t hrough t he observat ion of m inim um and m axim um values and m ean, m edian, and st andard deviat ion calculat ions. For qualit at ive variables, absolut e and r elat ive fr equencies w er e calculat ed. Com par ison of m eans w as car r ied out using St udent ’s t t est f or non- pair ed sam ples. Com par ison of pr opor t ions w as evaluat ed using Fisher ’s Exact Test . Significance lev el w as set at 0 . 0 5 (α= 5% ) . Hence, descript ive ( p- ) lev els below t his t hr eshold w er e consider ed as significant ( p< 0.05) .
RESULT S
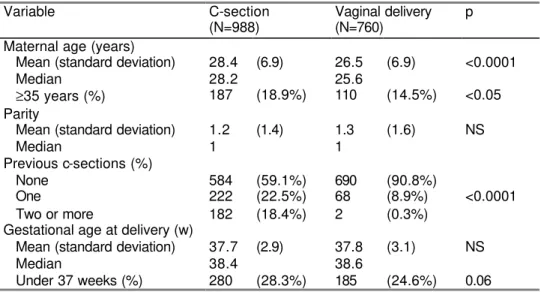
Table 3 – Characteristics of gestation according to type of delivery. April-December 2001.
Variable C-section Vaginal delivery p
(N=988) (N=760)
Maternal age (years)
Mean (standard deviation) 28.4 (6.9) 26.5 (6.9) <0.0001
Median 28.2 25.6
≥35 years (%) 187 (18.9%) 110 (14.5%) <0.05 Parity
Mean (standard deviation) 1.2 (1.4) 1.3 (1.6) NS
Median 1 1
Previous c-sections (%)
None 584 (59.1%) 690 (90.8%)
One 222 (22.5%) 68 (8.9%) <0.0001
Two or more 182 (18.4%) 2 (0.3%)
Gestational age at delivery (w)
Mean (standard deviation) 37.7 (2.9) 37.8 (3.1) NS
Median 38.4 38.6
Under 37 weeks (%) 280 (28.3%) 185 (24.6%) 0.06
Table 4 pr esent s dat a r efer ent t o t he m at er nal com plicat ions obser v ed, accor ding t o t h e t y p e of deliver y. Ther e w er e no st at ist ically significant differ ences in t er m s of hem or r hagic or infect ious com plicat ions, bot h of w hich occur r ed only in a sm all pr opor t ion of cases. Ut er ine at ony and hypot onic m yom et rium were t he m ost frequent am ong hem or r hagic com plicat ions. How ever , t hey w er e not r elat ed t o t y pe of deliv er y . Am ong t he cases t hat ev olv ed t o hem or r hagic com plicat ions, sev en r equir ed hyst er ect om y due t o excessive bleeding, six of w hich w er e fr om t he c- sect ion gr oup. Ot her com plicat io ns pr oper of each t y pe of pr ocedur e w er e also obser v ed. The pr olongat ion of hy st er ot om y is an ev ent obser v ed only in c- sect ion deliveries, w hereas perineal lacerat ions are proper of vaginal deliver y.
Table 4 – Maternal complications according to type of delivery. April to December 2001.
Variable c-section Vaginal delivery p
(n=988) (n=760)
Hemorrhagic complications
Uterine atony and hypotonia 7 (0.71%) 5 (0.66%) 0.87
Placenta accreta 4 (0.41%) 1 (0.13%) 0.40
Hypocoagulation (HELLP syndrome) 1 (0.10%) 0 (0%) 1.00
Total 12 (1.22%) 6 (0.79%) 0.53
Cases of hemorrhagic complications that evolved to
hysterectomy 6* (0.61%) 1** (0.13%) 0.15
Infectious complications
Endometritis 4 (0.41%) 1 (0.13%) 0.40
Infection-related hysterectomy 2 (0.20%) 0 (0%) 0.51
Incision deiscence with new abdominal wall closure 5 (0.51%) 2 (0.26%) 0.71
Total 11 (1.11%) 3 (0.40%) 0.16
Other complications
Prolongation of hysterotomy 7 (0.71%) -*** -*** -
Vesical lesion 1 (0.10%) 0 (0%) -
Perineal laceration
2nd degree rupture -*** -*** 16 (2.11%) -
*Indication: Atony (2 cases), HELLP syndrome (1 case), and placenta accreta (3 cases).
**Indication: Atony (1 case).
***Complication not pertinent to the respective type of delivery
No m at er nal deat hs dir ect ly r elat ed t o t he analyzed obst et r ical pr ocedur e w er e obser ved dur ing t he pr esent st udy .
D ISCUSSION
Th e h ig h in cid en ce of c- sect ions ( 56.5% ) in t he facilit y inv est igat ed r eflect s t he lar ge pr opor t io n ( 80% ) of pat ient s w it h int ercurrent clinical and/ or obst et ric condit ions am ong it s populat ion. This lim it s t he value of c - sect ion rat e com parisons w it h low - risk populat ions. Yazlle et al,1 5 in an analysis of deliver ies t aken place bet w een 1986 and 1995 in Ribeirão Pret o report a 48.4% c - sect ion r at e. Gov er nm ent al st at ist ics show a 48.4% c- sect ion r at e for t he st at e of São Paulo in 2000.9 These lev els are acknowledgedly higher t han t hose encount ered in t he US and Europe. Dobson5 r epor t s r at es as high as 21 .5% in England and Wales in 2000. Rat es in t he US varied bet ween 21 and 22% in t he 1989- 98 period.4 How ev er , a high incidence of c- sect ions in high - r isk pr egnancies is expect ed, and cont r ibut es t ow ar ds an incr ease in t hese r at es in univ er sit y hospit als,1 4 t o w hich m or e sev er e cases are referred. Sim ilarly, Turnbull et al1 3 r epor t ed a 43.9% c- sect ion rat e am ong high- risk pregnancies in Adelaide, Aust ralia, despit e t he count ry’s 19.5% nat ional rat e.
I n high risk pregnancies, clinical or obst et ric com plicat ions oft en require gest at ion t erm inat ion. I n such cases, som e part icularit ies usually prevent vaginal delivery. Pret erm birt h, which occurred in 26.6% of cases in t he pr esent st udy, hinder s t he induct ion of labor , especially in cases in w hich cer vical m at ur at ion has not yet been achieved, t hus pr om ot ing an incr ease in t he num ber of c-sect ions. Lik ew ise, t he induct ion of labor is not r ecom m ended in t he pr esence of ut er ine scar s. Thus, it er at iv e c- sect ions – w hen t he pat ient has a hist ory of t w o or m ore previous c - sect ions – ar e fr equent in Br azil. I n t he pr esent sur v ey , of t he pat ient s t hat under w ent c- sect ion delivery, as m any as 40% had a hist ory of prior c - sect ion s.
Mean m at ernal age w as low er am ong pregnancies t hat progressed t o vaginal deliveries. Pat ient s aged ≥35 years also present ed a higher c- sect ion r at e. The occur r ence of clinical abnor m alit ies is k now n t o be dir ect ly pr opor t ional t o age, oft en influencing t he r at e of c- sect ions. Bobrowski & Bot t om s2 ( 1995) found a relat ionship bet ween m at ernal age and int er cur r ent clinical condit ions such as chr onic ar t er ial hy per t ension and diabet es. These aut hor s also descr ibed an im por t ant incr ease in c- sect ion r at es in > 35 years nulliparae ( 48.5% ) .
An analy sis of t he incidence of c- sect ion- relat ed m at ernal com plicat ions show s a gr eat er absolut e num ber of com plicat ions involving t his procedure. How ever, t here w as no significant associat ion bet w een com plicat ions and t y pe of deliv er y ; it should also be not ed t hat t he fr equency of each com plicat ion w as low , w it h v alues below 1% .
t hat 5 . 1 4 % of cases of c - sect ion deliv er y pr esent ed infect ious com plicat ions char act er ized by fev er on t w o consecut iv e day s. This pr opor t ion w as significant ly higher t han t hat obser v ed aft er v aginal deliv er y ( 0.29% ) . How ev er , t he aut hor s did not include specific dat a on endom et r it is. Ot her st udies, r epor t gr eat er endom et r it is r at es of c- sect ions. Spinnat o et al1 2 ( 2000) report endom et rit is in 4.7% of non- elect iv e c- sect ions. Mah et al8 ( 2001) , in an analysis of risk fact ors for infect ions follow ing sur gical incision found t his t ype of com plicat ion in 2.8% of c- sect ions, and report ed independent risk fact or s such as sur ger y dur at ion and nonuse of pr ophy lact ic ant ibiot ic t her apy . How ev er , t he aut hor s again did not specifically discrim inat e endom et rit is.
Despit e t he lack of st at ist ical significance, t he pr esent sur v ey included t w o cases of hy st er ect om y due t o puerperal post - c- sect ion infect ion, which m ight have been avoided if a vaginal delivery had been carried out . Such sit uat ions are usually charact erized by a high risk of m at ernal m ort alit y, especially w hen accom panied by generalized infect ion or sept icem ia.
An im por t ant effect of hem or r hagic com plicat ions is t he need for hy st er ect om y , since t his pr ocedur e definit ely im pairs t he pat ient ’s reproduct ive life. I n t he present st udy, hem orrhage- r elat ed hy st er ect om y w as r equir ed for less t han 1% of cases. Few st udies include in- dept h analy ses of t he hem or r hagic com plicat ions r elat ed t o c- sect ions. Lov er r o et al6 ( 2001) evaluat ed blood loss during labor indirect ly, t hrough an analysis of t he need for blood t ransfusion during int ra - and post - delivery per iods. The aut hor s found no st at ist ically significant differ ences in t he per cent age of cases r equir ing int ra- delivery blood t ransfusion, which ranged from 0.1% in vaginal deliveries t o 0.4% in c- sect ion s. I n t he post - delivery period, a significant ly higher proport ion of t ransfused pat ient s w as observed am ong c- sect ion subj ect s ( 1.9% ) w hen com par ed t o t he vaginal deliver y gr oup ( 0.39% ) . Com bs et al3 ( 1991) report ed 6.4% incidence of hem orrhagic com plicat ions in 3,052 c- sect ion s, ch ar act er ized by = 10 point hem at ocrit reduct ions or t he need for blood t ransfusion. The aut hors also analyzed 9,598 vaginal deliveries, finding 3.9% incidence of t ransfusions.
Post - sur gical m or bidit y in obst et r ical pr ocedur es is influenced by t he cir cum st ances in w hich t hese pr ocedur es t ak e place. Ther e w er e no cases of c- sect ion- r elat ed m at er nal deat h in t he pr esent sam ple. Lydon- Rochelle et al7 ( 2001) consider ed c- sect ions not as a risk fact or for m at ernal m ort alit y, but as a m arker for preexist ent m orbidit y. Em ergency c- sect ions, as w ell as t hose indicat ed aft er t he onset of labor inv olv e condit ions not alw ay s adequat e for t he per for m ance of sur gical pr ocedur es. Tim e since m em brane rupt ure, num ber of pelvic exam inat ions, chorioam nionit is, and int ra - delivery fet al m onit or ing ar e som e of t he fact or s t hat m ay incr ease post - deliv er y infect ion incidence. St udies com paring elect ive and em ergency c - sect ions and vaginal delivery m ay aid in t he analy sis of com plicat ions r elat ed t o t hese pr ocedur es. The infor m at ion pr ovided t o t he couple m ust include, in a sim ple and obj ect iv e w ay , t he benefit s and r isk s of each t y pe of deliv er y , w it h em phasis on t he safet y of each pr ocedur e as w ell as it s associat ed com plicat ions, so t hat t he couple m ay m ak e a conscious decision concer ning t he t y pe of deliv er y t o be car r ied out .9 , 1 0
I n conclusion, no significant associat ions bet w een t he occur r ence of m at er nal com plicat ions and t y pe of delivery w ere obser ved dur ing t he analyzed per iod. The cont inuit y of r esear ch in t his healt hcar e unit , along wit h furt her st udies in low - r isk populat ions in t he pr ivat e and public healt hcar e sect or s pose new challenges t hat will aid in t he evaluat ion of t he risk of com plic at ions de fact o r elat ed t o t his surgical procedure.
REFEREN CES
1 . Bélizan JM, Alt habe F, Bar r os FC, Alexander S. Rat es and im plicat ions of caesar ean sect ions in Lat in Am er ica: ecological st udy . BMJ 1999; 319: 1397- 402.
2 . Bobrowski RA, Bot t om s SF. Underappreciat ed risks of t he elderly m ult ipara. Am J Obst et Gy necol 1995; 172: 1764- 70.
3 . Com bs CA, Murphy EL, Laros Jr RK. Fact or s associat ed w it h hem or r hage in cesar ean deliv er ies.
Obst et Gy necol 1991; 77: 77- 82.
4 . Cunningham FG, Gant NF, Leveno KJ, Gilst rap I I I LC, Haut h JC, Wenst rom KD. Cesarean delivery and post part um hyst erect om y. I n: Cunningham FG, Gant NF, Leveno KJ, Gilst rap I I I LC, Haut h JC, Wenst rom KD, edit ors. William s obst et rics. 21s t ed. New York: McGraw Hill; 2001. p. 537 -63.
5 . Dobson R. Caesarean sect ion rat e in England and Wales hit s 21% . BMJ 2001; 323: 951.
6 . Loverro G, Greco P, Vim ercat i A, Nicolardi V, Varcaccio- Garofalo G, Salvaggi L. Mat ernal com plicat ions associat ed w it h cesar ean sect ion. J Perinat Med 2001; 29: 322- 6 .
7 . Lydon- Rochelle M, Holt VL, East erling TR, Mart in DP. Cesarean delivery and post part um m ort alit y am ong prim iparas in Washingt on St at e, 1987 - 1996. Obst et Gy necol 2001; 97: 169- 74.
8 . Mah MW, Pyper AM, Oni GA, Mem ish ZA. I m p act of ant ibiot ic pr ophy lax is on w ound infect ion aft er cesar ean sect ion in a sit uat ion of ex pect ed higher r isk . Am J I nfect Cont r ol 2001; 29: 85 - 8 .
9 . Minist ério da Saúde. Sist em a de I nform ações de Nascidos Vivos ( SI NASC) . At ualização ano 2000: algum as inform ações sobre a saúde da m ulher [ on line] . Brasília ( DF) ; 2001. Disponível em
< URL: ht t p: / / www.saude.sp.gov.br/ dsaude/ inform es/ 7saude_m ulher/ ht m l/ saude_m ulher.ht m > [ 2002 abr 13]
10. Pat erson - Br ow n S. Should doct or s per for m an elect iv e caesar ean sect ion on req u est ? Yes, as long as t he wom an is fully inform ed. BMJ 1998; 317: 462 - 3 .
11. Rezende J. Aspet os m édico- legais e ét icos da obst et r ícia. I n: Rezende J, edit or . Obst et r ícia. 9t h ed. Rio de Janeiro: Guanabara Koogan; 2002. p.1435- 74.
12. Spinnat o JA, Youkilis B, Cook VD, Piet rant oni M, Clark AL, Gall SA. Ant ibiot ic prophylaxis at cesar ean deliv er y . J Mat er n Fet al Med 2000; 9: 348- 50.
13. Turnbull DA, Wilkinson C, Yaser A, Cart y V, Svigos JM, Robinson JS. Wom en's role and sat isfact ion in t he decision t o hav e a caesar ean sect ion. Med J Aust 1999; 170: 580 - 3 .
14. Whit sel AI , Capeless EC, Abel DE, St uart GS. Adj ust m ent for case m ix in com parisons of cesarean delivery rat es: universit y versus com m unit y hospit als in Verm ont . Am J Obst et Gy necol
15. Yazlle MEHD, Rocha JSY, Mendes MC, Pat t a MC, Mar colin AC, Azev edo GD. I ncidência de cesár eas segundo font e de financiam ent o da assist ência ao par t o. Rev Saúde Pública 2001; 35: 202- 6. 16. Yokoe DS, Christ iansen CL, Johnson R, Sands KE, Livingst on J, Sht at land ES, Plat t R. Epidem iology of and surveillance for post part um infect ions. Em er g I nfect Dis 2001; 7: 837 - 41.
17. Zugaib M, Bit t ar RE. Pr ot ocolos assist enciais da Clínica Obst ét r ica da Faculdade de Medicina da USP. São Paulo: At heneu; 1996.
AD D RESS T O CORRESPONDENCE
Roseli Mieko Yam am ot o Nom ura
Rua General Canavarro, 280 Bairro Cam pest re 09070 - 440 Sant o André, SP, Brazil
E- m ail: roseli.nom ura@t erra.com .br
Received on 10/ 11/ 2002. Reviewed on 10/ 7/ 2003. Approved on 5/ 8/ 2003.
© 2 0 0 3 Fa cu lda de de Sa ú de Pú blica da U n iv e r sida de de Sã o Pa u lo
Ave nida D r . Ar na ldo, 7 1 5 0 1 2 4 6 - 9 0 4 Sã o Pa ulo SP Br a zil
Te l./ Fa x : + 5 5 1 1 3 0 6 8 - 0 5 3 9