Descriptive study of breast cancer cases in Goiânia between 1989
Descriptive study of breast cancer cases in Goiânia between 1989
Descriptive study of breast cancer cases in Goiânia between 1989
Descriptive study of breast cancer cases in Goiânia between 1989
Descriptive study of breast cancer cases in Goiânia between 1989
and 2003
and 2003
and 2003
and 2003
and 2003
Estudo descritivo dos casos de câncer de mama em Goiânia, entre 1989 e 2003
Estudo descritivo dos casos de câncer de mama em Goiânia, entre 1989 e 2003
Estudo descritivo dos casos de câncer de mama em Goiânia, entre 1989 e 2003
Estudo descritivo dos casos de câncer de mama em Goiânia, entre 1989 e 2003
Estudo descritivo dos casos de câncer de mama em Goiânia, entre 1989 e 2003
R
ODRIGOD
ISCONZIN
UNES1; E
DESIOM
ARTINS2; R
UFFOF
REITAS-J
UNIOR, TCBC-GO
3; M
ARIAP
AULAC
URADO4; N
ILCEANAM
AYAA
IRESF
REITAS5;
J
OSÉC
ARLOSDEO
LIVEIRA2A B S T R A C T
A B S T R A C T
A B S T R A C T
A B S T R A C T
A B S T R A C T
Objective Objective Objective Objective
Objective: To describe cases of breast cancer in women living in Goiânia from 1989-2003. MethodsMethodsMethodsMethods: We conducted aMethods retrospective, descriptive stud, which included all cases of breast cancer occurring in residents of Goiânia, identified by the Population-Based Cancer Registry of Goiânia (RCBPGO) in the period from 1989 to 2003. The variables were: age, method of diagnosis, topographic location, morphology and extent of breast cancer. We used frequencies and percentage rates, and Poisson regression to determine the annual percentage change (APC). ResultsResultsResultsResultsResults: We identified 3204 cases of breast cancer. The most frequent topographic location was the superior-lateral quadrant (53.7%). Infiltrating ductal carcinoma (IDC) was the most frequent, with 2582 cases (80.6%), followed by infiltrating lobular carcinoma (ILC), with 155 cases (4.8%). There was a significant increase of both the IDC and the ILC, with APCs of 11.0% and 15.4%, respectively. The ratio between IDC and ILC was not influenced by age (p = 0.98). As for tumor extent at diagnosis, 45.6% were located in the breast, and the APC was 16.1% (CI = 12.4 to 20.0, p <0.001). There was a trend of APC reduction of metastatic cases (-3.8, CI = -8.6 to 1.2, p = 0.12). ConclusionConclusionConclusionConclusionConclusion: The topographical location and histological type of breast cancer in the city of Goiania followed the pattern of other countries. The main morphological types were not influenced by age. There was a large increase in initial cases.
Key words Key words Key words Key words
Key words: Breast neoplasms. Women. Cross sectional studies. Incidence. Epidemiology.
Work conducted by the Goiás Mastology Research Network, Goiás, Brazil.
1. Master’s Degree, Health Sciences, Postgraduate Program in Health Sciences, Faculty of Medicine, Federal University of Goiás - GO-BR; 2. Epidemiologist, Goiânia Population-based Cancer Registry, Association Against Cancer of Goiás-GO-BR; 3. Associate Professor, Department of Obstetrics and Gynecology, Federal University of Goiás -GO-BR; 4. Head, Department of Descriptive Epidemiology - International Agency for Research on Cancer (IARC); 5. Radiologist, Service of Radiation Oncology, Araujo Jorge Hospital, Association Against Cancer of Goiás-GO-BR.
INTRODUCTION
INTRODUCTION
INTRODUCTION
INTRODUCTION
INTRODUCTION
T
he incidence of breast cancer has been decreasing in
recent years in some developed countries including the
United States
1. In Brazil and other developing countries, its
incidence continues increasing
2-5.
In Brazil, for the year 2010, 49,240 new cases
were estimated
3, representing an incidence of 49 cases for
every hundred thousand women
2, with a growth trend,
especially for women between 40 and 59 years
5.
Breast cancer is the leading cause of cancer death
among Brazilian women, with mortality rates showing a
trend to stabilization
6. In Goiania, the standardized mortality
rate for world population of Segi
7was 14.87/100,000 in
1988, rising to 18.18/100 000 women in 2002
8.
Invasive ductal carcinoma (IDC) and invasive
lobular carcinoma (ILC) are the most common types of
breast cancer
9, and its morphology tends to follow an
international standard
10-12.
Although it is well established that early diagnosis
and treatment affect mortality rates and prevalence of the
neoplasia
11,13, there are few data available regarding the
descriptive epidemiology of breast cancer in Brazil.
The absence of such information makes both
the assessment of screening programs for breast cancer
and for comparison with other regions difficult. Thus, we
proposed to describe some epidemiological characteristics
of breast cancer in the female population of the city of
Goiânia in the period from 1989 to 2003, according to
variables collected by the Population-Based Cancer
Registry.
METHODS
METHODS
METHODS
METHODS
METHODS
of women with malignancies of the breast in Goiânia, Goiás
State, Brazil.
The cases were identified in the database of the
Population-Based Cancer Registry of Goiânia (RCBPGO) and
collected in the period from 1989 to 2003. The variables
analyzed were patient age at diagnosis; diagnostic basis,
which is the form in which case information is collected
(either by cytology or histology). When these tests were
absent, data were collected by imaging or clinical data
described by the doctor.
We used the topography and morphology, as the
O3 ICD (International Classification of Diseases for
Oncology, 3rd ed.)
14. The tumors with squamous cell
carci-noma (SCC) histological type were withdrawn from the
study because the topography was originated from the skin
of the breast.
We also analyzed the extent of disease. We
considered as an in situ”lesion when the histology returned
as such, without invasion of the basement membrane;
“localized”, the invading tumor, in which histological
examination showed no axillary lymph node status and
the patient did not have detectable metastases by clinical
examination or by imaging; “regional”, when there was
reference to lymph node involvement described in histology
or, in the absent of that, there was clinically palpable
axillary lymph nodes described by the attending physician
at the staging phase; “metastasis”, when the clinical
report, imaging or histological examination showed the
presence of metastatic disease outside the breast and
ipsilateral axilla.
The eligibility criteria for inclusion of cases
followed the methodology of RCBPGO. Eligibility for
inclusion included all cancer cases diagnosed annually in
women who were residents in the municipality of Goiânia.
To avoid selection bias of patients who came from other
places to be treated in Goiania, a diagnosis of cancer should
arise in a date later than the one on which the patient fix
her residence in the city, and, for purposes of registration,
the time taken for housing the patients before the start of
treatment was six months.
We used the software SPSS ® (Statistical
Package for the Social Sciences), version 15.0, for the
making of the database. Frequencies for all variables and
analysis of central tendency were observed to determine
the mean and median age.
We used Poisson regression to calculate the
annual percentage change (Statistical Research and
Applications Branch Division of Cancer Control and
Population Sciences, National Cancer Institute, USA).
RESULTS
RESULTS
RESULTS
RESULTS
RESULTS
We collected, by RCBPGO, 3204 cases of breast
cancer in the period from 1989 to 2003. The average age
was 56 years, with a median of 53 years and standard
deviation of ± 16 years. Also in relation to age, 15.2% of
women were 40 years or less and 57% were over 50
years.
Of the total of 3204 cases diagnosed between
1989 and 2003, in 857 the topographic location could be
known. Of these, the most common location was superior
lateral (SLQ), with 53.7% (n = 461), followed by the
supe-rior medial (SMQ) in 15.8% (n = 136) and the infesupe-rior
late-ral (ILQ) 12.1% (n = 104). For other topographic locations,
the values were: inferior medial quadrant (IMQ) in 11.4%
(n = 98), overlapping lesion of the breast (OLB) in 5.01% (n
= 43), nipple-areola 1.63% (n = 14) and 0.11% in the
axillary extension (n = 1).
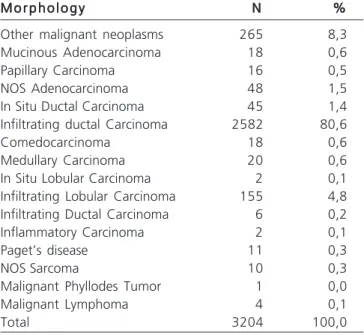
The most common morphology was infiltrating
ductal carcinoma, with 2582 cases (80.6%), followed by
infiltrating lobular carcinoma (4.8%). The extranodal
lymphomas and sarcomas comprised less than 1% of
ca-ses (Table 1). The analysis of trends over time showed that
both the average percentage change for invasive ductal
and invasive lobular carcinomas increased significantly
during the study period (Table 2). There was an equal
distribution of morphological types of cancer among the
age groups (Table 3).
Regarding the extent of disease, it was shown
that 45.60% of the cases were found, 19.70% had tumor
with regional extension and 10.20% had distant metastases
at diagnosis; only 4.20% (133) were in situ tumors. In this
analysis, 20.30% of cases had no information about the
extent of disease at diagnosis.
Table 1 Table 1 Table 1 Table 1
Table 1 - Absolute and relative frequencies of patients with breast cancer in Goiânia (1989-2003), according to morphology (n = 3204).
M o r p h o l o g y M o r p h o l o g y M o r p h o l o g y M o r p h o l o g y
M o r p h o l o g y NNNNN %%%%%
Other malignant neoplasms 265 8,3
Mucinous Adenocarcinoma 18 0,6
Papillary Carcinoma 16 0,5
NOS Adenocarcinoma 48 1,5
In Situ Ductal Carcinoma 45 1,4
Infiltrating ductal Carcinoma 2582 80,6
Comedocarcinoma 18 0,6
Medullary Carcinoma 20 0,6
In Situ Lobular Carcinoma 2 0,1
Infiltrating Lobular Carcinoma 155 4,8
Infiltrating Ductal Carcinoma 6 0,2
Inflammatory Carcinoma 2 0,1
Paget’s disease 11 0,3
NOS Sarcoma 10 0,3
Malignant Phyllodes Tumor 1 0,0
Malignant Lymphoma 4 0,1
Total 3204 100,0
The rate of in situ cases was zero in 1989,
increasing to 9.80% in 2003. In contrast, we observed that
patients with advanced disease decreased from 25.38% to
6.37%. The percentage distribution of all cases, according
to tumor extension and by year of diagnosis, is shown in
figure 1. By Poisson regression, we found that the annual
percentage change was 16.1% (95% CI = 12.4 to 20.0)
for cases of localized tumors (p <0.001). For those cases
with metastases at diagnosis, there was a non-significant
reduction of the percentage average change, which was
-3.83 (95% CI = -8.6 to 1.2) (p = 0.12).
DISCUSSION
DISCUSSION
DISCUSSION
DISCUSSION
DISCUSSION
This study showed that the average age of
women diagnosed with breast cancer in Goiânia was 56
years and median of 53 years, corroborating other studies
15-17. This result confirms that breast cancer is more common
in women over 50 years of age
5,18, stressing that prevention
programs should prioritize risk age groups.
During the study period there was an increase in
the absolute number of cases of breast cancer, possibly
due to the constant changes occurring in the lifestyle of
some Goiânia women, proven by data from the Surveillance
of Risk and Protective Factors for Chronic Diseases Phone
Survey (VIGITEL), including the increased use of alcohol
and increased intake of foods with polyunsaturated fats
19.
Other factors that should possibly have contributed to the
increased number of cases was improving coverage of
screening mammography in the state of Goiás, which is
increasing for women over 40 years
20,21, in addition to
increasing and aging of the Goiânia population
22.
Confirmation of the diagnosis by histopathology,
over 90% of cases, ensures the quality of information
generated by RCBPs
23, for of the 3204 patients with breast
cancer enrolled in RCBPGO, 94.7% were confirmed by
histopathology, with a increase of 10% in the last five years.
The results confirm that the SLQ of the breast is
the anatomical location of greatest involvement for breast
cancer, followed by the SMQ, corroborating data from other
authors
24,25. However, this information should be viewed
with caution, since in 73% of cases there was no reference
to location.
Infiltrating ductal carcinoma was the most
frequently reported tumor morphology by this study,
followed by infiltrating lobular carcinoma, these findings
are similar to other works’
24,25. It was also possible to
obser-ve the significant increase of the two most common
morphological types, and the average percentage increase
of ILC was numerically greater than the one of IDC.
Although it was previously observed that age can somehow
influence the histological type
9, in the present study we
observed that the distribution of the morphological types
was not influenced by age. This finding, although
Table 2 Table 2Table 2 Table 2
Table 2 – Analysis of the evolution of the annual percentage change of the most frequent morphological types.
H i s t o l o g y H i s t o l o g yH i s t o l o g y H i s t o l o g y
H i s t o l o g y % Initial% Initial% Initial% Initial% Initial % Final% Final% Final% Final% Final APC (CI 95%)APC (CI 95%)APC (CI 95%)APC (CI 95%)APC (CI 95%) PPPPP
Invasive ductal Carcinoma 3.37 12.66 11% (9.6 - 12.4) <0.001
Invasive lobular Carcinoma 1.29 18.71 15.4% (9.2 - 22.1) <0.001
% Initial = percentage rate of the total number of cases in the year 1989; % Final = percentage rate of the total number of cases in the year 2003; APC = average percentage change; CI = confidence interval.
Table 3 Table 3Table 3 Table 3
Table 3 – Distribution of the main morphological types of breast cancer, according to age groups.
H i s t o l o g y H i s t o l o g yH i s t o l o g y H i s t o l o g y
H i s t o l o g y Age (years)Age (years)Age (years)Age (years)Age (years) T o t a lT o t a lT o t a lT o t a lT o t a l up to 39
up to 39up to 39
up to 39up to 39 40 to 5940 to 5940 to 5940 to 5940 to 59 >>>>>6 06 06 06 06 0 N
N N N
N %%%%% NNNNN %%%%% NNNNN %%%%% NNNNN %%%%%
Invasive ductal Carcinoma 395 94 1302 94 885 94 2582 94
Invasive lobular Carcinoma 24 6 77 6 54 6 155 6
x2 = 0,3; p = 0,98.
Figure 1 Figure 1Figure 1
controversial, was also observed in a previous study
26.
Regarding the extent of the disease, in 2002 Miller
et al.
27reported that in the United States tumors localized
only in the breast were more frequent, ranging from 54%
to 72% of cases, followed by tumors with regional extension
(axillary lymph nodes ), between 23% and 38%. For tumors
with distant metastases at diagnosis, they found rates of
3% to 9%. Unlike the statistics of developed countries, our
study showed that 45% of cases of breast cancer were
reported to be localized, 10% regional and that
approximately 20% of cases were diagnosed with distant
metastases.
The low percentage of regional tumors reported
is due to RCBPGO’s late beginning to report cases of
regionalization of breast cancer, in 1994. Probably, in
previous years, the tumors have been registered as
regio-nal metastatic tumors, justifying the difference from the
literature
28. Despite this high percentage rate of patients
with metastases at diagnosis as a whole, we observed an
important change in the Brazilian statistics from other
studies, which suggest rates of up to 70% of the diagnosis
of breast cancer in advanced stages
29,30. The results
presented are relevant, since they are based on information
from a population of approximately 674,692 female
inhabitants
22.
We observed an increase of carcinomas in situ
and of localized extension carcinomas, which was significant.
This change suggests that government, private and third
sector actions, in combination, may have generated benefits
for the population at risk of breast cancer, allowing early
diagnosis
21.
With the present study we observed that there
was a growing number of new cases of breast cancer among
the residents of Goiania in the 15 analyzed years, and finally,
the most valuable information presented, the profile
suggests that breast cancer diagnosis in the city of Goiânia
is changing, with a substantial increase in the initial
diagnosis of cases over a reduction in advanced ones.
R E S U M O
R E S U M O
R E S U M O
R E S U M O
R E S U M O
Objetivo: Objetivo: Objetivo: Objetivo:
Objetivo: Descrever os casos de câncer de mama nas mulheres residentes em Goiânia no período 1989-2003. Métodos: Métodos: Métodos: Métodos: Métodos: Estudo retrospectivo, descritivo, que incluiu todos os casos de câncer de mama ocorridos nas moradoras de Goiânia, identificados pelo Registro de Câncer de Base Populacional de Goiânia (RCBPGO), no período de 1989 a 2003. As variáveis estudadas foram: idade, método de diagnóstico, localização topográfica, morfologia e extensão do câncer de mama. Foram utilizadas frequências e taxas percentuais, além da regressão de Poisson para determinação da mudança percentual anual (MPA). Resultados: Resultados: Resultados: Resultados: Resultados: Foram identifi-cados 3204 casos de câncer de mama. A localização topográfica mais frequente foi o quadrante superior lateral (53,7%). O carcinoma ductal infiltrante (CDI) foi o mais freqüente, com 2582 casos (80,6%), seguido pelo carcinoma lobular infiltrante (CLI), com 155 casos (4,8%). Houve aumento significante tanto do CDI quanto do CLI, sendo a MPA de 11,0% e de 15,4%, respectivamente. A proporção entre CDI e CLI não foi influenciada pela idade (p=0,98). Quanto à extensão do tumor ao diagnóstico, 45,6% dos casos eram localizados na mama, sendo que a MPA foi de 16,1% (IC= 12,4 a 20,0; p<0,001). Houve tendência de redução da MPA dos casos metastáticos (-3,8; IC= -8,6 a 1,2; p=0,12). Conclusão: Conclusão: Conclusão: Conclusão: Conclusão: A localização topográfica e o tipo histológico do câncer de mama, na cidade de Goiânia, seguem o padrão de outros países. Os principais tipos morfológicos não foram influenciados pela idade. Houve grande aumento de casos iniciais.
Descritores Descritores Descritores Descritores
Descritores: Neoplasias da mama. Mulheres. Estudos transversos. Incidência. Epidemiologia.
REFERENCES
REFERENCES
REFERENCES
REFERENCES
REFERENCES
1. Jemal A, Siegel R, Xu J, Ward E. Cancer statistics 2010. CA Cancer J Clin 2010; 60(5):277-300.
2. Jemal A, Center MM, DeSantis C, Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev 2010; 19(8):1893-907.
3. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Insti-tuto Nacional de Câncer Coordenação de Prevenção e Vigilância de Câncer. Estimativa 2010: Incidência de câncer no Brasil [online]. Rio de Janeiro: INCA, 2010. [acessado em 08 out. 2010]. Disponível em: http://www.inca.gov.br/estimativa/2010/index.asp?link= tabelaestados.asp&UF=BR
4. Freitas-Junior R, Freitas NM, Curado MP, Martins E, Moreira MA, e Silva CM. Variations in breast cancer incidence per decade of life (Goiania, GO, Brazil): 16-years analysis. Cancer Causes Control 2008; 19(7):681-7.
5. Freitas Jr R, Freitas NM, Curado MP, Martins E, Silva CM, Rahal RM, et al. Incidence trend for breast cancer among young women in Goiânia, Brazil. Sao Paulo Med J 2010; 128(2):81-4.
6. Fonseca LA, Eluf-Neto J, Wunsch Filho V. Cancer mortality trends in Brazilian state capitals, 1980-2004. Rev Assoc Med Bras 2010; 56(3):309-12.
7. Segi M. Graphic presentation of cancer incidence by site and by area and population. Nagoya, Japan: Segi Institute of Cancer Epidemiology; 1977.
8. Freitas NMA, Freitas Junior R, Curado MP, Martins E, Bandeira e Silva CM, Moreira MAR, et al. Tendência da incidência e da mor-talidade do câncer de mama em Goiânia: análise de 15 anos (1988-2002). Rev bras mastologia 2006; 16(1):17-21.
9. Albrektsen G, Heuch I, Thoresen SØ. Histological type and grade of breast cancer tumors by parity, age at birth, and time since birth: a register-based study in Norway. BMC Cancer 2010; 10:226. 10. Dutra MC, Rezende MA, Andrade VP, Soares FA, Ribeiro MV, Paula EC, et al. Imunofenótipo e evolução de câncer de mama: comparação entre mulheres muito jovens e mulheres na pós-menopausa. Rev Bras Ginecol Obstet 2009; 31(2):54-60. 11. Simon S, Bines J, Barrios C, Nunes J, Gomes E, Pacheco F, et al.
– The Amazone Project of the Brazilian Breast Cancer Study Group (GBECAM). Cancer Res 2009; 69 (24 Suppl):Abstract nr3082. 12. Hemminki K, Granström C. Morphological types of breast cancer
in family members and multiple primary tumours: is morphology genetically determined ? Breast Cancer Res 2002; 4(4):R7. 13. Nelson HD, Tyne K, Naik A, Bougatsos C, Chan BK, Humphrey L, et
al. Screening for breast cancer: an update for the U. S. Preventive Services Task Force. Ann Intern Med 2009; 151(10):727-37. 14. Fritz A, Percy C, Jack AShanmugaratnam K, Sobin L, Parkin DM,
Whelan S, editors. International classification of diseases of oncology. Genebra:WHO; 2000.
15. Mendonça GAS, Silva AM, Caula WM. Características tumorais e sobrevida de cinco anos em pacientes com câncer de mama admi-tidas no Instituto Nacional do Câncer, Rio de Janeiro, Brasil. Cad Saúde Pública 2004; 20(5):1232-9.
16. Moraes AB, Zanini RR, Turchiello MS, Riboldi J, Medeiros LR. Estu-do da sobrevida de pacientes com câncer de mama atendidas no hospital da Universidade Federal de Santa Maria, Rio Grande do Sul, Brasil. Cad Saúde Pública 2006; 22(10):2219-28.
17. Arpino G, Bardou VJ, Clark GM, Elledge RM. Infiltrating lobular carcinoma of the breast: tumor characteristics and clinical outcome. Breast Cancer Res 2004; 6(3):R149-56.
18. Hadjisavvas A, Loizidou MA, Middleton N, Michael T, Papachristoforou R, Kakouri E, et al. An investigation of breast cancer risk factors in Cyprus: a case control study. BMC Cancer 2010; 10:447.
19. Brasil. Portal da saúde. Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico (VIGITEL) [online]. Brasília: Ministério da Saúde. [acessado em 08 out. 2010]. Disponí-vel em: http://portal.saude.gov.br/portal/saude/profissional/ visualizartexto.cfm?idtxt=30864&janela=1
20. Brasil. IBGE – Instituto Brasileiro de Geografia e Estatística. Direto-ria de Pesquisas. Acesso a utilização de serviços de saúde 2003. PNADSaúde, 2003 [online]. [Acessado em 08 out. 2010]. Disponí-vel em http://www.ibge.gov.br/home/estatistica/populacao/ trabalhoerendimento/pnad2003/saude/
21. Freitas-Junior R, Corrêa RS, Peixoto JE. Desigualdade na cobertu-ra mamográfica no estado de Goiás, Bcobertu-rasil. Jornada Paulista de Radiologia, 2010, São Paulo. [acessado em: 08 out. 2010]. Dispo-nível em: http://www.spr.org.br/jpr2010_trabalhos.
22. Brasil. Departamento de informática do SUS (DATASUS) [online]. Brasília: Ministério da Saúde. [acessado em: 08 out. 2010]. Dispo-nível em: http://tabnet.datasus.gov.br/cgi/deftohtm.exe? ibge/cnv/ popgo.def.
23. Parkin DM, Whelan SL, Ferlay J, Teppo L, Thomas DB, editors. Cancer incidence in five continents. Lyon, France: IARC Scientific; 2002.
24. Eisenberg ALA, Koifman S. Aspectos gerais dos adenocarcinomas de mama, estadiamento e classificação histopatológica com des-crição dos principais tipos. Rev bras cancerol 2000; 46(1):63-77. 25. Tavassoli FA. Pathology of the breast. 2a ed. Stanford: Appleton
and Lange; 1999.
26. Lee JH, Park S, Park HS, Park BW. Clinicopathological features of infiltrating lobular carcinomas comparing with infiltrating ductal carcinomas: a case control study. World J Surg Oncol 2010; 8:34. 27. Miller BA, Hankey BF, Thomas TL. Impact of sociodemographic factors, hormone receptor status, and tumor grade on ethnic differences in tumor stage and size for breast cancer in US women. Am J Epidemiol 2002; 155(6):534-45.
28. Martins E, Freitas-Junior R, Curado MP, Freitas NM, De Oliveira JC, Silva CM. Temporal evolution of breast cancer stages in a population-based cancer registry in the Brazilian central region. Rev Bras Ginecol Obstet 2009; 31(5):219-23.
29. Cezar Jr OP. Carcinoma de mama em Bragança Paulista – Expe-riência de uma década. Ginec Obstet Atual 1996; 5(1):9-13. 30. Freitas-Junior R, Silveira-Junior LP, Carneiro AB, Ribeiro LFJ, Queiroz
GS. Fatores Associados à perda de seguimento das pacientes tra-tadas de câncer de mama. Rev Bras Mastol 1997; 7(1):58-63.
Received: 20/08/2010
Accepted for publication: 22/10/2010 Conflict of interest: none
Source of funding: partly funded (Research Support Foundation of the State of Goiás (FAPEG) Protocol. 200710267000252, and the Institute Avon.
How to cite this article: How to cite this article:How to cite this article: How to cite this article:How to cite this article:
Nunes RD, Martins E, Freitas-Junior R, Curado MP, Freitas NMA, de Oliveira JC. Descriptive study of breast cancer cases in goiânia between 1989 and 2003.Rev Col Bras Cir. [periódico na Internet] 2011; 38(4). Disponível em URL: http://www.scielo.br/rcbc