w w w . r b o . o r g . b r
Original
Article
Preliminary
analysis
on
the
MD-4
®
plasma-sprayed
titanium
acetabular
component
夽
Elmano
de
Araújo
Loures,
Leandro
Furtado
Simoni,
Isabel
Cristina
Gonc¸alves
Leite,
Daniel
Naya
Loures
∗,
Clarice
Naya
Loures
UniversidadeFederaldeJuizdeFora,JuizdeFora,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12February2014 Accepted24February2014 Availableonline19March2015
Keywords: Osseointegration Hiparthroplasty Hipprosthesis
a
b
s
t
r
a
c
t
Objectives:Toevaluatetheshort-termperformanceofatypeofimplantmanufacturedin Brazil.
Methods:This study analyzed a cohort of 60 patients who underwent implantation of MD-4® acetabular components during primary hip arthroplasty procedures performed
betweenJanuary1,2010,andAugust1,2012.Thepatientswerestudiedretrospectivelywith regardtoclinicalbehavior,stabilityandradiologicalosseointegration.Thepatientswere fol-lowedupforaminimumof12monthsandamaximumof42months(mean:27)andwere evaluatedbymeansoftheHarrisHipScore,SF-36questionnaireandserialconventional radiographs.
Results:Allthecomponentswereradiologicallystable,withoutevidenceofmigrationor progressiveradiolucencylines.Onaverage,theHarrisHipScoreevolvedfrom36.1to92.1 (p<0.001)andtheSF-36showedsignificantincreasesinallitsdomains(p<0.001).No dif-ferenceswereobservedamongpatientswithosteoarthrosis,osteonecrosis,hipdysplasiaor otherconditions.
Conclusions:The short-term results showed clinical and radiological signs of stability andosseointegrationoftheimplants,whichmayrepresentapredictivefactorregarding medium-termsurvivalofthisacetabularcomponent.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Análise
preliminar
do
componente
acetabular
de
titânio
plasma-spray
MD-4
®Palavras-chave: Osteointegrac¸ão Artroplastiadequadril Prótesedequadril
r
e
s
u
m
o
Objetivos:avaliarodesempenhoemcurtoprazodeumtipodeimplantefabricadonoBrasil. Métodos:estudo deumacoorte de 60pacientesquetiveram componentesacetabulares MD-4®implantadosduranteartroplastiasprimáriasdoquadril,entre1dejaneirode2010e
1deagostode2012,eforamestudadosretrospectivamentecomrelac¸ãoaocomportamento
夽
WorkdevelopedattheUniversityHospital,UniversidadeFederaldeJuizdeFora,JuizdeFora,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.N.Loures). http://dx.doi.org/10.1016/j.rboe.2015.03.003
clínico,àestabilidadeeàosteointegrac¸ãoradiológica.Osindivíduosforamacompanhados por12mesesnomínimoenomáximo42(média:27)eavaliadospormeiodoHarrisHip Score,doquestionárioSF-36ederadiografiasconvencionaisseriadas.
Resultados: todososcomponentesestavamradiologicamenteestáveis,semevidênciade migrac¸ãooudelinhasderadioluzênciaprogressivas.Emmédia,oHarrisHipScoreevoluiude 36,1para92.1(p<0,001)eoSF-36mostrouincrementosignificativoemtodososdomínios(p <0,001).Nenhumadiferenc¸afoiobservadaentrepacientescomosteoartrose,osteonecrose, displasiadoquadrilououtrascondic¸ões.
Conclusões: osresultadosdecurtoprazomostraramsinaisclínicoseradiológicosde estabil-idadeedeosteointegrac¸ãodosimplantes,oquepoderepresentarumfatorpreditivoquanto àsobrevivênciaemmédioprazodocomponenteacetabularconsiderado.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Over the last 20 years, a large variety of porous surfaces and metallic materialshave been used to achieve fixation bymeansofbonegrowth(ingrowth)intotaljointprostheses forthehipandotherjoints.Theonesmostcommonlyused arecomposedoftitaniumortitaniumalloys,rough-surfaced chromium–cobalt metal alloysand woven metal fiber. The externalcoatingsofthecupspresentmacroor microporos-ity,suchasthatobtainedthroughsprayingthesurfacewith titanium(plasmaspray)or,morerecently,throughusing tra-beculatedmetal.1
Studies on animal models, clinical studies and evi-dencefromimplantsremovedpostmortem(retrievals)have demonstrated the capacityof porous surfacesfor favoring bone growth through ingrowth and generating osseointe-gration. They are effective for supplementing or ensuring the primary mechanical stability that is achieved through introducingtheimplantunderpressure(i.e.press-fittingit), with or without adjuvant screws.2 Weller and Volkmann3 found that pores of diameters between 50 and 200m favored bone ingrowth and noted that spraying with titaniumisamethodcapableofreproducingthese parame-ters.
Absence of early translation of the metal cup is con-sidered to be indicative of good medium and long-term results.4,5 Bone growth on the porous external surface of the implant is influenced by the size of the pores, properties inherent to the materials and close proximity between the bone and implant.6 Surface roughness and osteoconductivity of the titanium coating have been cor-related with the primary and secondary stability of the implants.4
Theprimary objectives of the present analysis were to investigatethe clinicalperformance,stability and presence of short-term radiological signs of osseointegration of the acetabularcomponentanalyzed,andwhethertheremightbe anyassociationbetweenthestabilityandfixationofthecup andthevariablesofetiologicaldiagnosis,age,positioningand primarystabilityoftheimplant.Therearenostudiesinthe literatureontheperformanceofthe acetabularcomponent analyzedinthisseries.
Materials
and
methods
Thisstudywasapprovedbyourinstitution’sresearchethics committeeunder the number CEP408.719.All the individ-ualsselectedexplicitlyagreetoparticipatethroughafreeand informedconsentstatement.
Thiswasanobservationalclinicalstudythatexaminedan initialgroupof62individuals,fromwhichacohortof60 indi-vidualswasretrospectivelyevaluatedforaminimumperiodof 12monthsandamaximumof42months(mean:27).The MD-4®acetabularcomponent(MDTInd.Com.Imp.Exp.Implantes Ltda.)wasusedunderuniformconditionsbythesamesurgeon ataregionalteachingandreferralhospitalbetweenJanuary 2010andAugust2012.Theacetabularcomponentwasused togetherwithapolishedcementedfemoralnailwitha cen-tralizerandaplugtooccludethefemoralcanal,whichwere allmanufacturedinBrazil.Asecond-generationcementation techniquewasused.7Alltheindividualsreceivedtwo adju-vant titanium screws.Onlytwo caseswere lostduring the follow-up.
TheMD-4®acetabularcomponentiscomposedofa hemi-sphericalcupthatismanufacturedusingthe6Al–4Vtitanium alloy.8Theexternalcoatingofplasma-sprayedtitaniumhas ameanthicknessof150mandameanporesizeof224m. Thecomponenthasthreeperipheralholesforinserting adju-vanttitaniumfixationscrewsandonecentral(polar)holefor theimpactionguide.Theinsertofultra-highmolecularweight polyethyleneismoldedbymeansofamachiningprocess.It has18notchesandanedgeraisedby10◦,anditissterilized bymeansofgammaraysforusewithfemoralheadsof22mm (onlyforcupsof44–48mm)and28mm(forother measure-ments).
N=60 Osteoarthrosis secondary
to developmental dysplasia of the hip
5 (8%) Osteoarthrosis secondary
to femoroacetabular impingement
4 (7%)
Osteonecrosis of the femoral head
8 (13%)
Sequelae of fractures
3 (5%) (rheumatoid arthrosis)Collagenosis 2 (3%)
Severe dysplasia 3 (5%)
Idiopathic avascular necrosis 4 (7%)
Primary osteoarthrosis 31 (52%)
Fig.1–Etiologicaldistributionofthestudysample.
physicianbutwasnotinvolveddirectlywiththeprovisionof carefortheindividualsunderanalysis.Conventional radio-graphswereobtainedinanteroposteriorandlateralviewsof theproximalfemurandcoxofemoraljoint,withmagnification ofapproximately 15%.Theclinicaland functionalvariables wereevaluatedbymeansofaspecificinstrument,i.e.the Har-risHipScore(HHS),10whichwasusedinassociationwiththe SF-36questionnaire.11TheHarrisHipScore(excellent:90–100 points;good:80–90;satisfactory:70–79;andpoor:lowerthan 70)andtheSF-36questionnairewereappliedbeforethe oper-ationandatthesix-monthfollow-up.Thestandarddeviation wascalculatedforeachiteminvestigated,beforeandafterthe operation.TheMann–Whitneytestwasusedforpaired com-parisonswhen thedata werenormally distributedand the Wilcoxontestwasusedfornonparametricdata.The signifi-cancelevelwassetasp<0.05.Thedataanalysiswasdeveloped usingthe StatisticalPackageforthe SocialSciences(SPSS), version15.0(Chicago,IL,USA).
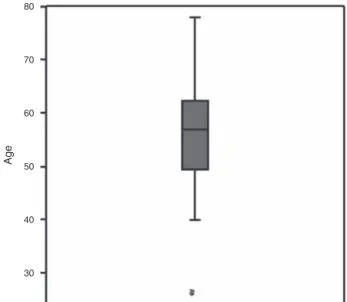
TheetiologiesofthecasesaredescribedinFig.1andthe agegroupsoftheindividualsareshowninFig.2.
Themodified Hardingelateral hipaccess12 wasused in lateraldecubitus.Acephaliccomponentofdiameter22mm was used in only one case of a cup of size 44mm, in a patientwithdevelopmentaldysplasiaofthehip.Alltheother casesreceivedaninterchangeableheadof28mmin diame-ter.Second-generationcephalosporinwasusedasprophylaxis against infection, for the entire sample: 2g immediately beforethe operationand then1gevery 8h. Thiswas con-tinueduntilthevacuumdrainwasremoved,nomorethan 48h after the procedure. For prophylaxis against throm-boembolism,theapproachrecommendedbySalvattietal.13 was used, consisting of use of elastic stockings, stimula-tion ofearly movement and useof aspirin:300mg/day for 30 days, startingfrom the second day afterthe operation. Useofenoxaparin(40mg/dayfor21days)was reservedfor
cases with a high risk of thromboembolism (16.8% of the individuals).
Shavers2mmsmallerthan theexternaldiameterofthe cupwereused.Theexternaldiameterhadbeenselected pre-viouslybymeansoftransparencies(templates),withaview toensuringagoodpressfit.Allthecystsidentifiedduringthe surgicalprocedurewerecurettedandpastyautologousspongy graftwasapplied.Thiswasobtainedfromthefinalshaving andfromthefemoralhead.Amassiveautologousgraftfrom thefemoralhead,fixedwithspongyscrews,wasusedintwo hipstocorrectacetabulardysplasia.INimplantingthe compo-nent,theaimwastorestoretheanatomicalcenterofrotation ofthe hip and theorientationofthe so-calledsafety zone ofLewinneket al.,14 i.e.abduction of40±10◦ and antever-sionof15±10◦.Theprimarystabilityofthecupwastested
80
70
60
50
Age
40
30
intraoperativelyandavisualcheckwasmadetoseewhether therewasanylevelofmovementafterthefinalimpaction. Fromthethirdpostoperativeday,partialweight-bearingusing forearmcrutcheswasauthorized,and thiswasmaintained untilthe45thday,whenfullweight-bearingontheoperated limbwasallowed.
The radiographs obtained after six weeks of evolution formedtheinitialparameterforidentifyingcysts,failuresat thebone-implantinterface,radiolucentlinesandmigrationof thecomponent.
AsrecommendedbyMalizosetal.,6inthezonesinwhich thesurfaceofthecomponentwasnotinclosecontactwiththe boneonthereferenceradiograph,thisfindingwasclassified asa“flaw”(gap).Thiswasdonetoestablishadistinctionin relationtoradiolucentlinesthatmightappearonsubsequent radiographs,inareaswherenoflawsexistedinitially.The sub-chondralcystswereidentifiedandmonitored.Toevaluatethe migrationofthecomponent,weusedthecriterionofNunn etal.,15whichisrecommendedforearlyevaluationsinwhich thepolyethyleneinsertisnotexpectedtohavebecomeworn. Inthismethodology,thereferencepointsaretheteardrop,the centeroftheheadandthehorizontalandverticaldistances betweenthecenteroftheheadandtheipsilateraland con-tralateralteardrops.Thefollowingfindingswereconsidered tobeindicativeoflooseningandinstability:acircumferential radiolucentzone>2mminvolvingmorethan50%ofthe bone-implantinterface;andverticalorhorizontalmigrationgreater thanorequalto2mm.Thereferencepointsconsideredwere theteardrop andthe distancesfrom thisto theupperand medialedgesoftheacetabulumandtothecenterofthecup16 and/orchangestotheinclinationofthecupof4◦.17
Theradiological parameters that have been reported to beindicativeoffailureoffixationandofosseointegrationof theimplantconsistofobservationofprogressiveand/or com-pleteradiolucentlinesatthebone-implantinterfaceandthe presenceofflaws(gaps)atthebone-metalinterfaceandbone cyststhatdonotfilloverthecourseoftime,withorwithout associatedmigration of the component. According to sev-eralauthors,thisparameterconstitutesdefinitiveevidenceof instabilityandloosening.18,19
Thelocalizationoftheradiologicalfindingswasbasedon theclassificationofDeLeeandCharnley.20
Results
Satisfactory stability (withpress fit) was obtained, as veri-fied during the operation, in 53 individuals (88.3%). Three acetabularcomponentspositionedwithanabductionangle of more than 50◦ were observed. These were among the sevenindividuals(11.7%)inwhomtheinitialpress-fitstability was unsatisfactory. The mean angle of inclination (abduc-tion)oftheacetabularcomponentwas45.5◦(minimumof35◦ andmaximumof56◦).Sixcases(10%)presentedradiolucent linesof1or2mmintwozonesatthesix-monthfollow-up, buttherewasnoradiographicprogressionand/ormigration and/orinstabilityoftheimplantatthefollow-ups12and18 monthsaftertheoperation.Anapparentincreaseinbone den-sitywasobservedin13cases(21.6%),inDeLeeandCharnley’s zones1and2.20
Sixoutofthe12subchondralcyststhathadbeen identi-fieddecreasedinsizebetweenthe thirdand sixthmonths, andfourofthemshowedsubtotalfillingafterninemonthsof evolution.Theothersixcontinuedtopresentthesame appear-ance.Asmallboneflaw(gap)wasdetectedinthepolarregion infourcases(6.6%)inthisseries,withpartialfillingafter18 monthsofobservationinthreecasesandtotalfillinginone case.
Thecomplicationsobservedwereasfollows:onecaseof neuropraxia of the fibular portion of the sciatic nerve, in whichthelimbstretchingreached2.5cm,withpartial recov-eryseenaftersixmonthsofevolutionandfullrecoveryafter18 months;oncecaseofsuperficialinfectionwithfavorable reso-lutionandretentionoftheimplant;andonecaseofdeepvein thrombosis.Therewerenocasesofinstability/dislocationor heterotopicossification.Itwasalsoobservedfromthe radio-graphiccontroldonesixmonthsaftertheoperationthatatiny fragmenthadbecomedetachedfromthegreatertrochanter intwo cases,withmarked osteopenia.Bothofthesecases evolvedtoboneconsolidation,withoutanyclinical repercus-sions.
Allthecementedfemoralcomponentswerefoundtohave remainedfixed,withoutanysignsofsubsidenceor radiolu-centlines,andwithintacthomogenouscementlayers.They wereclassifiedbytheobserversaswellpositioned,exceptin twocases,inwhichslightvarusdeviationofthenailwasseen. Inthepresentstudy,therewasdiscordancebetweenthe twoobserversin14cases(23.3%)withregardtothepresence ofdiscontinuityofthebone-metalinterface(presenceofgaps orradiolucencygreaterthan2mm),fromwhichlow interob-serverconcordancewasinferred.Aconsensuswasreached atasecondcombinedevaluationwithrepetitionofthe radio-graphs.
Apositiveassociationwasobservedinthisseriesbetween absenceofsatisfactoryprimarypress-fitstabilityand position-ingoftheacetabularcomponentatanangleoutsideofthe safetyzone(p<0.001).However,thisdidnotcompromisethe secondarystability.
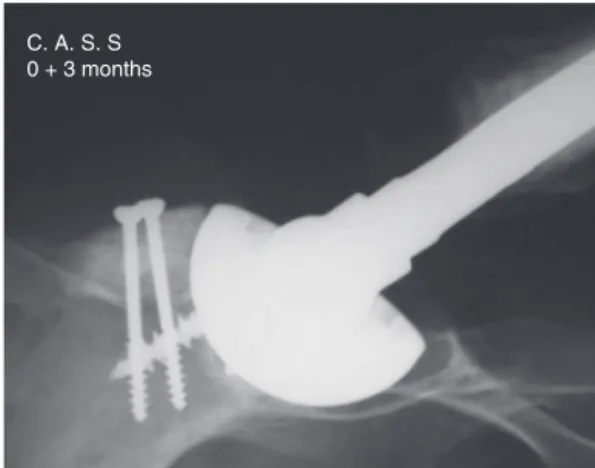
During the postoperative follow-up, no occurrences of acetabularor femoralosteolyticlesionswere detected.Nor wasthereanymeasurablewearonthepolyethyleneinsert. Therefore,giventhecriteriausedandtakingimplantrevision foranyreasonasanoutcome(Kaplan–Meyeranalysis),100%of theacetabularcomponentswerestableandfunctionalatthe timeofthelastradiologicalcontrol(Tables1and2,Figs.3–6).
Discussion
Implant performance can be evaluated through a variety ofclinicalmethodsand throughimaging.Hirakawaetal.21 emphasized that the performance of an implant and its osseointegration can bemeasured byperformingtests and clinicalassessments,butthatthedefinitivejudgmentshould be made after postmortem examination of the implants (retrievals).ThisviewwascorroboratedbyCuckler.22
Table1–MeanscoresfortheeightdomainsthatconstitutetheSF-36andHarrisHipScore(HHS)andtheirstatistical significance(p-value).
Variables Beforeoperation Afteroperation p
Mean(SD) Mean(SD)
SF-36
Functionalcapacity 12.9(15.1) 52.6(27.7) <0.010
Limitationduetophysicalaspects 7.9(19.9) 47.1(41.0) <0.001
Pain 23.6(18.5) 62.3(25.7) <0.002
Generalstateofhealth 55.9(23.1) 71.0(22.5) <0.001
Vitality 41.6(23.1) 69.1(21.8) <0.001
Socialaspects 41.8(24.2) 73.9(25.1) <0.001
Emotionalaspects 22.9(35.0) 66.7(37.0) <0.001
Mentalhealth 54.6(26.8) 80.3(17.8) <0.001
HHS 36.4(15.1) 92.3(5.7) <0.001
L.L.S.–P.O. 18 months
Fig.3–Radiologicalosseointegration,18monthsafterthe operation.
easeofaccess,andthefamiliarityofobserverswiththe tech-nique,stimulateitsroutineuseuniversally.Radiostereometry
techniques provide greater accuracy in evaluating implant
translation and rotation, but theyare not readily available inoursetting.23Gruenetal.24reportedontheradiographic resultsfromevaluatinganacetabularcomponentinan exten-sivemulticenter study thatused conventional radiography. Althoughno consensushasbeen reached, some investiga-tors have assessed the accuracy of simple radiographs in relation to the state of fixation of uncemented acetabular componentsandhavereportedthatsequentialradiographsin
M.C.O.A.-P.O. 12 months
Fig.4–Radiologicalosseointegration,12monthsafterthe operation.
0+9 months Z. F. L.
Fig.5–Partialfillingofcyst,ninemonthsafterthe operation.
anteroposteriorandlateralviewshavehighsensitivity(94%) andspecificity(100%),witha100%positivepredictionvalue foridentifyingthestatusofporoushemisphericalacetabular cups.25
Someauthorshavetakentheviewthatalterationstothe positionoftheimplantof1mmoverthefirstyearsprobably reduceitsusefullife,whileothershavebelievedthat migra-tionofupto2mmwouldnotbeadefinitivesignofaseptic loosening.26,27Althoughthepresenceofcompleteradiolucent linesissuggestiveofloosening,migrationofthecomponent isconsideredtobetheonlysafecriterionforassertingthat theacetabularcomponenthasloosenedandnotbecome inte-grated.Therefore,determiningthisiscriticalforthediagnosis andrequiresstandardizedserialradiographsbasedoncorrect anatomicalreferencepoints.19
C. A. S. S 0 + 3 months
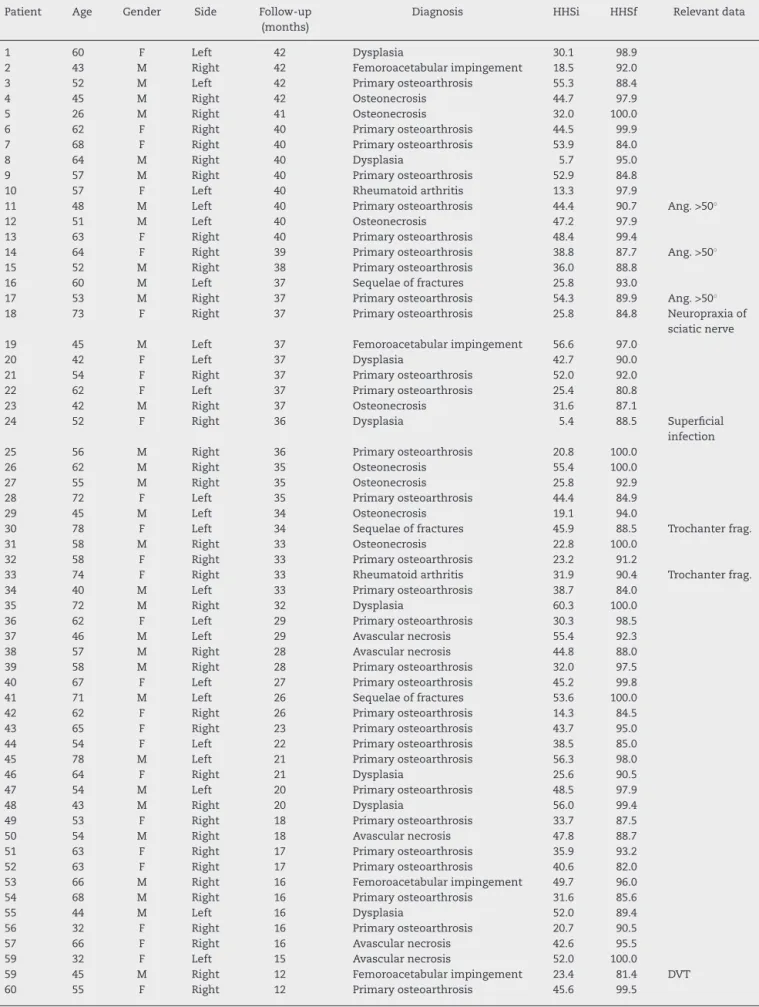
Table2–Demographicsandsummarydescriptionofthecasesandradiologicalfindings.
Patient Age Gender Side Follow-up (months)
Diagnosis HHSi HHSf Relevantdata
1 60 F Left 42 Dysplasia 30.1 98.9
2 43 M Right 42 Femoroacetabularimpingement 18.5 92.0
3 52 M Left 42 Primaryosteoarthrosis 55.3 88.4
4 45 M Right 42 Osteonecrosis 44.7 97.9
5 26 M Right 41 Osteonecrosis 32.0 100.0
6 62 F Right 40 Primaryosteoarthrosis 44.5 99.9
7 68 F Right 40 Primaryosteoarthrosis 53.9 84.0
8 64 M Right 40 Dysplasia 5.7 95.0
9 57 M Right 40 Primaryosteoarthrosis 52.9 84.8
10 57 F Left 40 Rheumatoidarthritis 13.3 97.9
11 48 M Left 40 Primaryosteoarthrosis 44.4 90.7 Ang.>50◦
12 51 M Left 40 Osteonecrosis 47.2 97.9
13 63 F Right 40 Primaryosteoarthrosis 48.4 99.4
14 64 F Right 39 Primaryosteoarthrosis 38.8 87.7 Ang.>50◦
15 52 M Right 38 Primaryosteoarthrosis 36.0 88.8
16 60 M Left 37 Sequelaeoffractures 25.8 93.0
17 53 M Right 37 Primaryosteoarthrosis 54.3 89.9 Ang.>50◦
18 73 F Right 37 Primaryosteoarthrosis 25.8 84.8 Neuropraxiaof
sciaticnerve
19 45 M Left 37 Femoroacetabularimpingement 56.6 97.0
20 42 F Left 37 Dysplasia 42.7 90.0
21 54 F Right 37 Primaryosteoarthrosis 52.0 92.0
22 62 F Left 37 Primaryosteoarthrosis 25.4 80.8
23 42 M Right 37 Osteonecrosis 31.6 87.1
24 52 F Right 36 Dysplasia 5.4 88.5 Superficial
infection
25 56 M Right 36 Primaryosteoarthrosis 20.8 100.0
26 62 M Right 35 Osteonecrosis 55.4 100.0
27 55 M Right 35 Osteonecrosis 25.8 92.9
28 72 F Left 35 Primaryosteoarthrosis 44.4 84.9
29 45 M Left 34 Osteonecrosis 19.1 94.0
30 78 F Left 34 Sequelaeoffractures 45.9 88.5 Trochanterfrag.
31 58 M Right 33 Osteonecrosis 22.8 100.0
32 58 F Right 33 Primaryosteoarthrosis 23.2 91.2
33 74 F Right 33 Rheumatoidarthritis 31.9 90.4 Trochanterfrag.
34 40 M Left 33 Primaryosteoarthrosis 38.7 84.0
35 72 M Right 32 Dysplasia 60.3 100.0
36 62 F Left 29 Primaryosteoarthrosis 30.3 98.5
37 46 M Left 29 Avascularnecrosis 55.4 92.3
38 57 M Right 28 Avascularnecrosis 44.8 88.0
39 58 M Right 28 Primaryosteoarthrosis 32.0 97.5
40 67 F Left 27 Primaryosteoarthrosis 45.2 99.8
41 71 M Left 26 Sequelaeoffractures 53.6 100.0
42 62 F Right 26 Primaryosteoarthrosis 14.3 84.5
43 65 F Right 23 Primaryosteoarthrosis 43.7 95.0
44 54 F Left 22 Primaryosteoarthrosis 38.5 85.0
45 78 M Left 21 Primaryosteoarthrosis 56.3 98.0
46 64 F Right 21 Dysplasia 25.6 90.5
47 54 M Left 20 Primaryosteoarthrosis 48.5 97.9
48 43 M Right 20 Dysplasia 56.0 99.4
49 53 F Right 18 Primaryosteoarthrosis 33.7 87.5
50 54 M Right 18 Avascularnecrosis 47.8 88.7
51 63 F Right 17 Primaryosteoarthrosis 35.9 93.2
52 63 F Right 17 Primaryosteoarthrosis 40.6 82.0
53 66 M Right 16 Femoroacetabularimpingement 49.7 96.0
54 68 M Right 16 Primaryosteoarthrosis 31.6 85.6
55 44 M Left 16 Dysplasia 52.0 89.4
56 32 F Right 16 Primaryosteoarthrosis 20.7 90.5
57 66 F Right 16 Avascularnecrosis 42.6 95.5
59 32 F Left 15 Avascularnecrosis 52.0 100.0
59 45 M Right 12 Femoroacetabularimpingement 23.4 81.4 DVT
60 55 F Right 12 Primaryosteoarthrosis 45.6 99.5
In aradiological study that evaluated cups coated with trabecularmetal,Macheras et al.28 demonstrated thatover a24-weekfollow-upperiod,itcouldclearlybeseenthatthe flawsinthebone-implantinterfacehadbeenfilledandthat osseointegrationofthecupshadoccurred.Overthelongterm, noneoftheseimplantspresentedasepticloosening.Itis possi-bletoinferfromthesestudiesthatconventionalradiographic methodscontinuetobethestandardmostusedroutinelyfor followingupandevaluatinghipprostheses.
Komarasamyet al.29and Mulieret al.30 reportedresults withfollow-upsof32 monthsand46 months,respectively. Mulier found that the density of spongy bone in zone I increasedin79%ofthecasesandthatinzoneIII,itincreased in58%ofthe24hipsthatreachedcompleteradiological eval-uations.
Thesamefindingwasseenintheradiologicalevaluations after12and18monthsoffollow-up,in13cases(21.6%)ofthe presentsample.
Clinical-radiological analyses on implants with micro-porouscoatingssuchasPlasmapore®,31,32whichisequivalent towhatisusedonthe MD-4® acetabularcomponent, have highlightedtheimportanceofearlybone-implantinteraction anditsinfluenceonthelong-termsurvivaloftheprosthetic replacement.Thetypeofcoating,the porosityand thesize oftheporesarecrucialfactorsinrelationtoosseointegration andsecondarystability.
Whilethelimitationsofthepresentstudy(duetothesmall numberofpatientsandtheshortdurationofthefollow-up) needtobeborneinmind,thesamplewashomogenous in relation to the diverse variables considered. The observed earlyevidenceofradiologicalosseointegrationofthe acetab-ularcomponentbecomesimportantwithinthecontextofthe absenceofrecentpublisheddataonimplantsmanufactured inBrazilintheindexedmedicalliterature.
Conclusion
The short-term clinical and radiological results obtained demonstratedthatalltheimplantswerestable.Inmostcases, the acetabularcomponents evaluated showed radiographic signs ofosseointegration.These resultswere equivalent to theperformanceofsimilarproductsundersimilarconditions, whichmayconstituteapredictivefactorwithregard tothe medium-termsurvivalofthecomponent.
Long-termfollow-upofalargernumberofindividualsand analysisonpostmortemspecimensareessentialfordefinitive conclusionstobeobtainedregardingthebehaviorofthistype ofimplant.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. D’AngeloF,MurenaL,CampagnoloM,ZattiG,CherubinoP. Analysisofboneingrowthonatantalumcup.IndianJ Orthop.2008;42(3):275–8.
2.StallforthH,BlömerW.Biomechanicalandtechnological aspectsofcementlesshipimplants.In:WellerS,VolkmannR, editors.Thebicontacthipimplantsystem.NewYork:Thieme Stuttgart;1994.p.2–11.
3.WellerS,VolkmannR,editors.Thebicontacthipimplant system.NewYork:ThiemeStuttgart;1994.
4.EnghCA,BobynJD,GlassmanAH.Porouscoatedhip replacement:factorsgoverningboneingrowth,stress shieldingandclinicalresults.JBoneJointSurgBr. 1987;69(1):45–55.
5.RohrlSM,NivbrantB,SnorrasonF,KarrholmJ,NilssonKG. Porous-coatedcupsfixedwithscrews:a12yearclinicaland radiostereometricfollow-upstudyof50hips.ActaOrthop. 2006;77(3):393–401.
6.MalizosKN,BargiotasK,PapatheodorouL,HantesM, KarachailosT.Survivorshipofmonoblocktrabecularmetal cupsinprimaryTHA:midtermresults.ClinOrthopRelatRes. 2008;466(1):159–66.
7.BarrackRL,MulroyRDJr,HarrisWH.Improvedcementing techniquesandfemoralcomponentlooseninginyoung patientswitharthroplasty:a12yearradiographicreview.J BoneJointSurgBr.1992;74(3):385–9.
8.ASTMInternational.ASTMF136-08e1standardspecification forwroughttitanium-6aluminum-4vanadiumELI(extralow interstitial)alloyforsurgicalimplantapplications(UNS R56401).WestConshohocken:ASTMInternational;2008. 9.KellgrenJH,LawrenceJS.Radiologicalassessmentof
osteoarthrosis.AnnRheumDis.1957;16(4):494–502. 10.GuimarãesRP,AlvesDPL,SilvaGB,BittarST,OnoNK,Honda
E,etal.Traduc¸ãoeadaptac¸ãotransculturaldoinstrumento deavaliac¸ãodoquadrilHarrisHipScore.ActaOrtopBras. 2010;18(3):142–7.
11.QuintanaJM,EscobarA,AguirreU,LafuenteI,ArenazaJC. Predictorsofhealth-relatedquality-of-lifechangeaftertotal hiparthroplasty.ClinOrthopRelatRes.2009;467(11): 2886–94.
12.HardingeK.Thedirectlateralapproachtothehip.JBone JointSurgBr.1982;64(1):17–9.
13.SalvatiEA,SharrockNE,WestrichG,PotterHG,ValleAG, SculcoTP.The2007ABJSNicolasAndryAward:threedecades ofclinical,basic,andappliedresearchonthromboembolic diseaseafterTHA:rationaleandclinicalresultsofa multimodalprophylaxisprotocol.ClinOrthopRelatRes. 2007;459:246–54.
14.LewinnekGE,LewisJL,TarrR,CompereCL,ZimmermanJR. Dislocationsaftertotalhipreplacementarthroplasties.JBone JointSurgAm.1978;60(2):217–20.
15.NunnD,FreemanMA,HillPF,EvansSJ.Themeasurementof migrationoftheacetabularcomponentofhipprostheses.J BoneJointSurgBr.1989;71(4):629–31.
16.LakemeierS,AurandG,TimmesfeldN,HeyseTJ,
Fuchs-WinkelmannS,SchoferMD.Resultsofthecementless Plasmacupinrevisiontotalhiparthroplasty:aretrospective studyof72caseswithanaveragefollow-upofeightyears. BMCMusculoskeletDisord.2010;11:101.
17.LatimerHA,LachiewiczPF.Porous-coatedacetabular componentswithscrewfixation.Fivetoten-yearresults.J BoneJointSurgAm.1996;78(7):975–81.
18.RabelloBT,CabralFP,FreitasE,PenedoJ,CuryMB,RinaldiER, etal.Artroplastiatotaldoquadrilnãocimentadaem pacientescomartritereumatoide.RevBrasOrtop. 2008;43(8):336–42.
19.WhiteREJr.Evaluationofthepainfultotalhipreplacement. In:CallaghanJJ,RosenbergAG,RubashHE,editors.Theadult hip.2nded.Philadelphia:Lippincott-Wilkins;2007.p.1343–8. 20.DeLeeJG,CharnleyJ.Radiologicaldemarcationofcemented
21.HirakawaK,JacobsJJ,UrbanR,SaitoT.Mechanismsoffailure oftotalhipreplacements:lessonslearnedfromretrieval studies.ClinOrthopRelatRes.2004;(420):10–7.
22.CucklerJM.Ifhipimplantretrievalscouldspeak.Whatwould theytellus?JBoneJointSurgBr.2012;9411Suppl.A: 11–3.
23.ThannerJ.Theacetabularcomponentintotalhip
arthroplasty.Evaluationofdifferentfixationprinciples.Acta OrthopScandSuppl.1999;286:1–41.
24.GruenTA,PoggieRA,LewallenDG,HanssenAD,LewisRJ, O’KeefeTJ,etal.Radiographicevaluationofamonoblock acetabularcomponent:amulticenterstudywith2-to5-year results.JArthroplasty.2005;20(3):369–78.
25.BozicKJ,RubashHE.Thepainfultotalhipreplacement.Clin OrthopRelatRes.2004;(420):18–25.
26.KärrholmJ,HerbertsP,HultmarkP,MalchauH,NivbrantB, ThannerJ.Radiostereometryofhipprostheses.Reviewof methodologyandclinicalresults.ClinOrthopRelatRes. 1997;(344):94–110.
27.StocksGW,FreemanMA,EvansSJ.Acetabularcupmigration. Predictionofasepticloosening.JBoneJointSurgBr.
1995;77(6):853–61.
28.MacherasGA,PapagelopoulosPJ,KaterosK,KostakosAT, BaltasD,KarachaliosTS.Radiologicalevaluationofthe metal-boneinterfaceofaporoustantalummonoblock acetabularcomponent.JBoneJointSurgBr.2006;88(3):304–9. 29.KomarasamyB,VadiveluR,BruceA,KershawC,DavisonJ.
Clinicalandradiologicaloutcomefollowingtotalhip arthroplastywithanuncementedtrabecularmetal
monoblockacetabularcup.ActaOrthopBelg.2006;72(3):320–5. 30.MulierM,RysB,MokeL.Hedroceltrabecularmetal
monoblockacetabularcups:mid-termresults.ActaOrthop Belg.2006;72(3):326–31.
31.BraunA,PappJ,ReiterA.Theperiprostheticbone
remodellingprocess–signsofvitalbonereaction.IntOrthop. 2003;27(Suppl1):S7–10.