SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Evaluation
of
body
mass
index
as
a
prognostic
factor
in
osteoarthrosis
of
the
knee
夽
Fabrício
Bolpato
Loures
a,∗,
Rogério
Franco
de
Araújo
Góes
a,
Pedro
José
Labronici
a,
João
Maurício
Barretto
b,
Beni
Olej
caHospitalSantaTeresa,Petrópolis,RJ,Brazil
bInstitutoNacionaldeTraumatologiaeOrtopedia(Into),RiodeJaneiro,RJ,Brazil
cUniversidadeFederalFluminense,Niterói,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27July2015
Accepted31August2015
Availableonline26May2016
Keywords:
Osteoarthrosis Obesity Knee Arthroplasty
a
b
s
t
r
a
c
t
Objective:Toevaluatetherelationshipbetweenpatients’bodymassindex(BMI)andthe
degreeofradiographicseverityofkneeosteoarthrosis.
Method:117patientswithgonarthrosiswereevaluatedprospectively.Thepatients’BMIwas
calculatedandtheirkneearthrosiswasclassifiedinaccordancewiththemodifiedAhlbäck
criteria.Kruskal–Wallisanalysisofvariance(ANOVA)wasusedtoevaluatetherelationship
betweenthesetwovariables.
Results:ThegroupclassifiedasAhlbäckgradeVhadsignificantlyhigherBMIthantheothers.
Conclusion:ThereisadirectrelationshipbetweenBMIandthedegreeofradiographicseverity
ofgonarthrosis.Obesityappearstobedirectlyrelatedtotheprogressionofknee
osteoarthro-sis.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Avaliac¸ão
do
índice
de
massa
corporal
como
fator
prognóstico
na
osteoartrose
do
joelho
Palavras-chave:
Osteoartrose Obesidade Joelho Artroplastia
r
e
s
u
m
o
Objetivo:Avaliararelac¸ãodoíndicedemassacorporal(IMC)dopacientecomograude
gravidaderadiográficadaosteoartrosedojoelho.
Método:Foramavaliados,de formaprospectiva,117pacientesportadores degonartrose.
Ospacientestiveramseusíndicesdemassacorporalcalculadoseaartrosedojoelhofoi
classificadasegundooscritériosdeAhlbäckmodificados.Usou-seaAnovadeKruskal–Wallis
paraavaliararelac¸ãoentreessasduasvariáveis.
夽
StudyconductedatHospitalSantaTeresa,Petrópolis,RJ,Brazil.
∗ Correspondingauthor.
E-mail:fbolpato@gmail.com(F.B.Loures).
http://dx.doi.org/10.1016/j.rboe.2016.05.002
2255-4971/©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
Resultados: OgrupoclassificadocomograuVdeAhlbäckapresentouumIMC
significativa-mentemaiordoqueosdemais.
Conclusão:Existerelac¸ãodiretaentreoIMCeograudegravidaderadiográficodagonartrose.
Aobesidadepareceestardiretamenterelacionadaàprogressãodaosteoartrosedojoelho.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Osteoarthrosis(OA),osteoarthritis,orarthrosisistheleading
causeofmusculoskeletaldisabilityworldwide1andthemain
physicallimitingfactorintheelderlypopulation.2This
seri-ousglobalpublichealthissue1affects5.2%ofthepopulation
over19yearsofage(about10millionpeople).Thisnumberis
expectedtogrowto12.4millionby2015.3
Traditionally,this disease isconsidered a cartilage joint
degenerationcausedbymechanical,genetic,hormonal,bone,
andmetabolicfactors,whichresultinanimbalancebetween
thedegradationandsynthesisofarticularcartilage.4OAis
cur-rentlyrecognizedasadiseasethataffectsalltissuesofthe
joint.5
The pathology arises from a combination of host and
environmentalfactors.6Obesityisoneofthemainelements
directlylinkedtokneeOApathogenesis.7Anincreaseinthe
bodymassindex(BMI)isalsoassociatedwithprogressionof
thedisease,degreeofdisability,evolutiontoarthroplasty,and
poorclinicaloutcomeaftersurgery.2
Obesityreachesitspeakincidenceinthesixthdecadeof
life,8aperiodthatcoincideswiththeworseningofthe
symp-tomsofdegenerative diseases.Itisanepidemicdisease in
Brazil.Thecountrynowranksfifthworldwideinthenumber
ofobeseindividuals.9
Thisstudyaimedtoassesstherelationshipofthepatient’s
BMIandthedegreeofkneeOAradiographicseverity,according
totheAhlbäckclassificationmodifiedbyKeyesetal.10
Material
and
methods
Afterapprovalofthestudyprotocolbytheethicscommittee
ofthe institution,117individualswho wouldundergototal
kneearthroplasty(TKA)betweenAugust2012andSeptember
2013wereselectedbyconvenience.Allpatientswhoagreedto
participatebysigningthefreeandinformedconsentformand
whohadaclinicalandradiographicdiagnosisofgonarthrosis
wereincluded. Patientswithhistoryoffractureorprevious
surgery in the studied knee, inflammatory diseases, bone
defectsrequiringgrafting,orvarusorvalgusdeformitygreater
than15◦wereexcluded.
Inthepre-operativeconsultation,patientshadtheirheight
and body massmeasured in amechanical anthropometric
scale, Micheletti® brand, MIC 2 model, accuracy class III,
withmass capacity of300kg and heightof 1.95m. During
thatassessment,patientsworeonlyadisposablegownand
underwear.Weightwasdocumentedinkilogramsandheight
inmeters. TheBMIwascalculatedbydividingbody weight
byheightsquared.Thisratiowasrecordedinkilogramsper
squaremeters(kg/m2),asdescribedbyAdolpheQuelet.11
Kneeradiographswereperformedwithloadand
monopo-dalsupportintheanteroposteriorincidence(AP)andprofile
with 30◦ of flexion, with 35cm×43cm film for AP and
24cm×30cmfilmforprofile,thepatientat110cm fromthe
lightbulb,andthebeamcenteredontheinferiorpoleofthe
patella. Super 100®X-rayequipment (Philips®, Brazil) was
used,calibratedto50kVand31mA.Thestudieswere
eval-uatedbythemaininvestigatorregardingimagequality,and
wererepeatedifnecessary.
The preoperative evaluation protocol was completed in
ordertostandardizedatacollection.Subjectswerecategorized
byBMI,asrecommendedbytheWorldHealthOrganization12
(Table1).
Knee OA was classified by the main investigator using
theAhlbäckcriteriamodifiedbyKeyesetal.10(Table2).This
classificationwas done blindly inrelationtopatient’s BMI.
Subsequently,dataweresenttothestatistician, whomade
thegroupingaccordingtothedegreeofarthrosis.
Kruskal–Wallisanalysisofvariance(ANOVA)wasusedto
assess whetherthegroupsdifferedinageand BMI.Dunn’s
multiplecomparison(nonparametric) wasappliedat5%to
Table1–Weightclassificationperbodymassindex
(BMI).
Classification BMI(kg/m2)
Underweight <18.5
Normalweight 18.5–24.9
Overweight 25.0–29.9
ObeseclassI 30.0–34.9
ObeseclassII 35.0–39.9
ObeseclassIII ≥40.0
Source:WHO.12
Table2–Ahlbäckclassification,modifiedbyKeyesand
Goodfellow.
GradeI Jointspacenarrowing GradeII Jointspaceobliteration
GradeIII AP=tibialplateauattrition<5mm
Profile=posteriorpartofthetibialplateauintact GradeIV AP=5–10mmtibialplateauattrition
Profile=extensiveattritiontheposteriorpartofthe tibialplateau
GradeV AP=Severesubluxationofthetibia Profile=anteriortibialsubluxation>10mm
identifythosegradesthatdifferedsignificantlyamong them-selves.
Theage ofthe groups was analyzed by calculating the
mean, median, minimum, and maximum; Kruskall–Wallis
ANOVAwasusedtoassessthehomogeneityofthegroups.
Results
Theanthropometriccharacteristicsofthesample,suchasage,
bodyweight,height,andBMI,weredescribedandareshown
inTable3.
Afterclassificationofeachkneeaccordingtothemodified
Ahlbäckcriteria,patientsweredividedintogroupsandtheir
BMIswereusedtocalculatethemean,median,standard
devi-ation,minimum,andmaximumofeachgroup.Kruskal–Wallis
ANOVAshowedasignificantdifferenceinBMIamonggroups
(p=0.047).ThesevaluesareshowninTable4.
Inordertodeterminewhichgroupsweredifferent,Dunn’s
multiple comparisons test at the level of 5% was used,
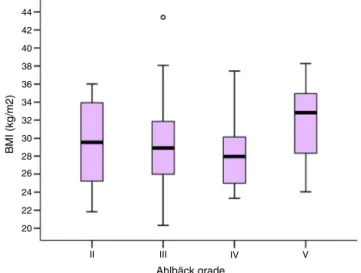
revealingthat thegroup classifiedas AhlbäckgradeVhad
significantlyhigherBMIthangradesIIIandIV(p=0.047),as
showninFig.1.ThegroupclassifiedasAhlbäckgradeIIhad
asmallnumberofpatients(n=10),whichreducesreliability
forinclusionintheanalysis.Nostatisticallysignificant
differ-encesatthelevelof5%wereobservedamongtheotherpairs
ofgroups.
The age of the groups was also compared with
Kruskal–WallisANOVA.Themeanvalues,median,standard
deviation,maximum,andminimumofeachgroupareshown
inTable5. Statisticalanalysisshowedthatthe samplewas
homogeneous regardingage, and the differences were not
significant(p=0.20).
Amongpatientswho hadarthrosis classifiedasAhlbäck
gradeV,61%(11)hadaBMIgreaterthan30kg/m2andwere
classifiedasobese.Thisnumberwasloweringroupsdegrees
ofarthrosisIIIandIV,42% and27%(25andeightpatients),
respectively.Amongthe117operatedpatients,only20(17.1%)
Table3–Anthropometriccharacteristics.
Variable Mean SD Median Minimum Maximum
Age(years) 68.9 7.1 68.5 53 84
Weight 77.3 13.4 77 53 120
Height(m) 1.6 0.1 1.62 1.4 1.9
BMI(kg/m2) 29.3 4.5 28.7 20.3 43.4
Source:Datafromtheinstitution.
SD,standarddeviation;BMI,bodymassindex
Table4–ComparisonofBMIgroupsafterdivisionby
Ahlbäckclassification.
Grade Number Mean SD Median Minimum Maximum p-Valuea
II 10 29.3 5.3 29.5 21.8 36.0 0.047
III 59 29.2 4.6 28.9 20.3 43.4
IV 30 28.2 3.6 28.0 23.3 37.4
V 18 31.9 4.3 32.8 24.0 38.3
Source:Datafromtheinstitution.
SD,standarddeviation;BMI,bodymassindex
a Kruskal–WallisANOVA.
44
42
40
38
36
34
32
30
28
BMI (kg/m2)
26
24
22
20
II III IV
Ahlbäck grade
V
Fig.1–ComparisonamongAhlbäckgroups.
Table5–Comparisonofagegroupsafterdivisionby
Ahlbäckclassification.
Grade Number Mean SD Median Minimum Maximum p-Valuea
II 10 65.0 7.0 64.5 55 74 0.20
III 59 69.0 6.8 68.5 55 82
IV 30 68.8 6.0 68 58 79
V 18 70.7 9.2 73 53 84
Source:Datafromtheinstitution.
SD,standarddeviation;BMI,bodymassindex
a Kruskal–WallisANOVA.
hadnormalweight,accordingtoWorldHealthOrganization
standards.
Discussion
Thefirstepidemiologicalstudythatdescribedtherelationship
ofobesitywithkneeOAwastheFraminghanstudy,7which,
after40yearsoffollowup,definedobesityasaprecedent
con-ditiontoosteoarthrosis. Otherrisk factorsdescribed inthe
study were female sex, aging,and geneticinheritance, but
theseareimmutable.
Obesityisacontemporarydiseasethatisepidemicinthe
UnitedStates:themajorityofadultsinthatcountryare
over-weightorobese,accordingtotheWorldHealthOrganization
standards.InBrazil,thenumberofoverweightindividualshas
tripledinthelast30years:62.5%ofmenand64.9%ofwomen
areoverweightorobese.13Thisplacesthecountryasfifthin
theworldrankingofobesity.9
BMIhasan excellentcorrelation withthepercentageof
bodyfatinmostofthepopulation14andactsasapredictor
ofobesity,althoughitiscontroversialinobviouslyextreme
cases. Itisa simpleand reliablemeasurement thatcanbe
usedforriskassessmentofkneeosteoarthrosis.15
Bodyweighthasbeenshowntobeanimportantrisk
fac-torinthegenesisofosteoarthrosis,8andthemainaffected
joint istheknee.16 Therearenumeroustheoriestoexplain
thecausalrelationshipbetweenobesityandkneeOA,ranging
frommechanicaltometabolicfactors.6TheincidenceofOA
inobese individuals istwicethatfoundinthose with
patientshavea38%increaseinOAprevalence.Obese
individ-ualshavea200%higherchance,whileinthemorbidlyobese
grouptheprevalenceis400%higher.
Knowing the naturalhistory and the factors that
influ-encetheevolutionofthedisease iscrucialtoitstreatment
andprognosis.18 TheassociationbetweenBMIand
progres-sionofkneeosteoarthrosisisnotclearyet.Fewstudieshave
triedtodifferentiate the factors involvedin thegenesis of
thedisease from those relatedto itsprogression; although
preventingitsprogressionmay bemoreeffectiveasa
pub-lic health strategy than trying to inhibit its emergence.19
Cooper et al.,19 after a five-year follow-up of 354 patients
withameanof75.8years,observedthatobesityisarisk
fac-torforboth incidenceand radiographicprogression ofOA,
althoughits greatestinfluenceisonthegenesisofthe
dis-ease.Sharmaetal.20studied292kneeswithOA154withvarus
and115withvalgusalignment.Theyfoundadirect
relation-shipbetweenBMIandradiographicseverityofthediseasein
patientswithvarusalignment,butnotinpatientswith
val-gusknee,highlightingthatobesitymustbeassociatedwith
otherfactorstodeterminetheevolutionofthedisease.After
asystematicreviewoftheliterature,Beloetal.21concluded
thattheassociationbetweenBMIandOAprogressionis
uncer-tain.
Thepresent studyshowedadirectrelationshipbetween
thepatient’sBMIandradiographicseverityofkneeOA,which
is in agreement with findings in the literature.18–20,22 The
meanageofthegroupscouldbeaconfoundingfactor,asthe
diseaseisprogressiveandolderpatientstendtohavehigher
jointwear.22,23Statisticaltestsrevealedthatthegroupswere
homogeneousregardingage,showingthatthisfactordidnot
influencetheassociationobserved.
Agoodratingsystemshouldbesimple,reproducible,and
abletogroupdifferentstagesofaninjuryinhomogeneous
subgroups, allowing for comparisonsand indicating
treat-mentandprognosis.Ratingsthatassessthereductioninjoint
spacearebetterforevaluatingtheprogressionofa
degener-ativekneedisease.18,24TheauthorsbelievethattheAhlbäck
classification,modifiedbyKeyesetal.,10meetsthese
prereq-uisites.Albuquerque et al.24 observeda poorinterobserver
correlationforthemodifiedAhlbäckclassification;however,
Gallietal.25havereportedthatphysiciansexperiencedinknee
surgerycansafelyusethisclassification.Themain
investiga-torisamemberoftheBrazilianSocietyofOrthopedicsand
Traumatology(SociedadeBrasileiradeOrtopedia e
Trauma-tologia[SBOT]), amember ofthe Brazilian Society ofKnee
Surgery(SociedadeBrasileiradeCirurgiadoJoelho[SBCJ])and
holdsaMaster’sdegreeinthearea,consideredexperiencedin
kneesurgeryandthereforeabletomaketheclassifications.
Petersonet al.26 reported a good correlation inthis
classi-fication, both interobserver and in relationto the Kellgren
and Lawrenceclassification.27 Theprevalenceofjoint pain
isstronglyrelated tothe radiographicclassification.19 Most
patientsinthepresentstudywereclassifiedasAhlbäckgrade
III,astageinwhichclinicaltreatmentusuallyceasestobe
effectiveandsurgerybecomesanoption.
IntheUnitedStates,approximately450,000knee
arthro-plasties were performed in 2005. Projections indicate that,
according to the aging population and the growth of
obe-sity,thesenumbersareexpectedtoreach3.5millionTKAsby
2030.28TherearenoofficialstatisticsforBrazil,butitis
esti-matedthatover70,000totalkneeprosthesesareperformed
peryear.29Thecountrynowranksfifthintheworldranking
ofobesity;projectionsoftheBrazilianInstituteofGeography
and Statistics(InstitutoBrasileiro deGeografia eEstatística
[IBGE])indicatethat,by2030,thecountrywillhavethesixth
largest elderlypopulationworldwide.30 Thecombinationof
thesetwofactorsallowsforthepredictionthattherewillbean
exponentialgrowthofosteoarthrosisinBrazil.Understanding
whysomepatientsdevelopneedforarthroplasty,while
oth-ersremainwithstablediseaseforlongperiods,maybethe
solutiontocontrolthismajorpublichealthproblem.
Besidesbeinganimportantfactorinthegenesisand
sever-ity ofknee osteoarthritis,1,7 asshown inthe presentstudy,
Guiaetal.16haveshownthatoverweightindividualsare1.5
timesmorelikelyandthatobeseindividualsarethreetimes
morelikelytoundergoarthroplastywhencomparedwiththeir
normalweight peers.Theassociation betweenobesity and
outcome aftersurgeryisambiguous. Bakeret al.31
demon-strated that outcome after TKA was satisfactory in obese
patients, but therateofsurgicalwoundcomplicationswas
higherinthisgroup.Samsonetal.,32afteraliteraturereview,
showed thatthecomplicationrateinpatientswithmorbid
obesitywas 10–30%higherthan inthecontrolgroup.Deep
infection was threeto nine times morefrequent. Kremers
etal.,33afterstudying8129patientsundergoingprimaryTKA
(6475)orTKArevision(1654),demonstratedthatthefinal
hos-pitalcostsinpatientswithaBMIabove30kg/m2was250–300
dollarshigherinprimaryarthroplastiesand600–650dollars
higherinrevisionarthroplasty.
The present study had some limitations. The modified
Ahlbäckclassificationisthemostpopularamongsurgeons,
but its usehinderedcomparisonwithother studies,which
mostlyusedtheKellgreenandLawrenceclassification.27The
verticalstudydesigndidnotallowforafollow-upofthe
tem-poralevolutionofthepatients.
Conclusion
There is a direct relationship between BMI of the patient
andtheradiographicseverityofkneeosteoarthrosis.Obesity
appearstobeassociatedwiththeprogressionofthisdisease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ScottW.Norman.Insall&Scottsurgeryoftheknee.5thed. Philadelphia:ElsevierChurchillLivingstone;2012.
2.CentersforDiseaseControlandPrevention(CDC).Prevalence ofdoctor-diagnosedarthritisandarthritis-attributable activitylimitation–UnitedStates,2010–2012.MMWRMorb MortalWklyRep.2013;62(44):869–73.
4. CamanhoGL,ImamuraM,Arendt-NielsenL.Gênesedador naartrose.RevBrasOrtop.2011;46(1):14–7.
5. NeogiT.Clinicalsignificanceofbonechangesin
osteoarthritis.TherAdvMusculoskeletDis.2012;4(4):259–67.
6. DohertyM.Riskfactorsforprogressionofkneeosteoarthritis. Lancet.2001;358(9284):775–6.
7. FelsonDT.Theepidemiologyofkneeosteoarthritis:results fromtheFraminghamOsteoarthritisStudy.SeminArthritis Rheum.1990;203(Suppl.1):42–50.
8. FehringTK,OdumSM,GriffinWL,MasonJB,McCoyTH.The obesityepidemic:itseffectontotaljointarthroplasty.J Arthroplasty.2007;226(Suppl.2):71–6.
9. KhanA.AmericaTopsListof10MostObeseCountries.
USNEWS.2014.Availablein:http://health.usnews.com/
health-news/health-wellness/articles/2014/05/28/america-tops-list-of-10-most-obese-countries[Accessedin12.08.2014]. 10.KeyesGW,CarrJA,MillerRK,GoodfellowJW.Theradiographic
classificationofmedialgonarthrosis.ActaOrthopScand. 1992;63(5):497–501.
11.EknoyanG.AdolpheQuetelet(1796–1874)–theaverageman andindicesofobesity.NephrolDialTranspl.2008;23(1):47–51.
12.Obesity:preventingandmanagingtheglobalepidemic.
ReportofaWHOconsultation.WorldHealthOrganTechRep
Ser.2000;894:i-xii,1-253.
13.Brasil.InstitutoBrasileirodeGeografiaeEstatística.Síntese
deindicadoressociais.Umaanálisedascondic¸õesdevidada
populac¸ãobrasileira2010.RiodeJaneiro,Brasil.Availablein:
http://www.ibge.gov.br/home/estatistica/populacao/
condicaodevida/indicadoresminimos/sinteseindicsociais2010/ SIS2010.pdf.
14.SeidellJC,FlegalKM.Assessingobesity:classificationand epidemiology.BrMedBull.1997;53(2):238–52.
15.AbbateLM,StevensJ,SchwartzTA,RennerJB,HelmickCG, JordanJM.Anthropometricmeasures,bodycomposition, bodyfatdistribution,andkneeosteoarthritisinwomen. Obesity(SilverSpring).2006;14(7):1274–81.
16.deGuiaN,ZhuN,KeresteciM,ShiJE.Obesityandjoint replacementsurgeryinCanada:findingsfromtheCanadian JointReplacementRegistry(CJRR).HealthcPolicy.
2006;1(3):36–43.
17.MokdadAH,FordES,BowmanBA,DietzWH,VinicorF,Bales VS,etal.Prevalenceofobesity,diabetes,andobesity-related healthriskfactors,2001.JAMA.2003;289(1):76–9.
18.SchoutenJS,vandenOuwelandFA,ValkenburgHA.A12year followupstudyinthegeneralpopulationonprognostic factorsofcartilagelossinosteoarthritisoftheknee.Ann RheumDis.1992;51(8):932–7.
19.CooperC,SnowS,McAlindonTE,KellingrayS,StuartB, CoggonD,etal.Riskfactorsfortheincidenceandprogression ofradiographickneeosteoarthritis.ArthritisRheum. 2000;43(5):995–1000.
20.SharmaL,LouC,CahueS,DunlopDD.Themechanismofthe effectofobesityinkneeosteoarthritis:themediatingroleof malalignment.ArthritisRheum.2000;43(3):568–75.
21.BeloJN,BergerMY,ReijmanM,KoesBW,Bierma-ZeinstraSM. Prognosticfactorsofprogressionofosteoarthritisoftheknee: asystematicreviewofobservationalstudies.Arthritis Rheum.2007;57(1):13–26.
22.IsbagioH.Factorsaffectingradiographicprogressionofknee osteoarthritis.ActaMedIndones.2004;36(2):87–92.
23.AlbuquerqueRP,FernandesRSC,BarrettoJM,CarvalhoACP, MoraesMB,AbreuT.Associac¸ãoentreosteoartrosedojoelho eoíndicedemassacorporal.RevCientFMC.2009;4(1): 10–8.
24.AlbuquerqueRP,GiordanoV,SturmL,AzevedoJúniorV,Leão A,AmaralNP.Análisedareprodutibilidadedetrês
classificac¸õesparaosteoartrosedojoelho.RevBrasOrtop. 2008;43(8):329–35.
25.GalliM,DeSantisV,TafuroL.Reliabilityofradiographic gradingofkneeosteoathritis.OsteoarthritisCartilage. 2003;11(8):580–4.
26.PeterssonIF,BoegårdT,SaxneT,SilmanAJ,SvenssonB. Radiographicosteoarthritisofthekneeclassifiedbythe AhlbäckandKellgren&Lawrencesystemsforthe tibiofemoraljointinpeopleaged35–54yearswithchronic kneepain.AnnRheumDis.1997;56(8):493–6.
27.KellgreenJH,LawrenceJS.Radiologicalassessmentof osteoarthrosis.AnnRheumDis.1957;16(4):494–502.
28.KurtzS,OngK,LauE,MowatF,HalpernM.Projectionsof primaryandrevisionhipandkneearthroplastyintheUnited Statesfrom2005to2030.JBoneJointSurgAm.
2007;89(4):780–5.
29.SaladeImprensa.Artroplastiaéparaalíviodador.Available
in:http://www.boehringer.com.br/conteudoimprensa texto.asp?conteudo=12&texto=988[Accessedin:02.06.2014].
30.Brasil.InstitutoBrasileirodeGeografiaeEstatística.
Indicadoressociodemográficos-prospectivosparaoBrasil
1991–2030.RiodeJaneiro:IBGE;2006.[cited2008May13].
Availablein:www.ibge.gov.br/home/estatistica/populacao/
projecaodapopulacao/publicacaoUNFPA.pdf.
31.BakerP,PetheramT,JamensonS,GreggPaulDeehanD.The associationbetweenbodymassindexandtheoutcomesof totalkneearthroplasty.JBoneJointSurgAm.
2012;94(16):1501–8.
32.SamsonAJ,MerecerGE,CampbellDG.TotalKnee
replacementinthemorbidlyobese:aliteraturereview.ANZJ Surg.2010;80(9):595–9.
33.KremersMH,VisscherSL,KremersKW,NaessensJM, LewallenDG.Theeffectofobesityondirectmedicalcostsin totalkneearthroplasty.JBoneJointSurgAm.