ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Fixed-flexion
knee
radiography
using
a
new
positioning
device
produced
highly
repeatable
measurements
of
joint
space
width:
ELSA-Brasil
Musculoskeletal
Study
(ELSA-Brasil
MSK)
Rosa
Weiss
Telles
∗,
Luciana
Costa-Silva,
Luciana
A.C.
Machado,
Rodrigo
Citton
Padilha
dos
Reis,
Sandhi
Maria
Barreto
UniversidadeFederaldeMinasGerais,CentrodeInvestigac¸ãoELSA-BrasildeMinasGerais,FaculdadedeMedicina,BeloHorizonte,MG, Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18November2015 Accepted21October2016 Availableonline22December2016
Keywords:
Fixed-flexionradiography Jointspacewidth Repeatability Knee Osteoarthritis
a
b
s
t
r
a
c
t
Objective:Todescribetheperformanceofanon-fluoroscopicfixed-flexionPAradiographic protocolwithanewpositioningdevice,developedfortheassessmentofkneeosteoarthritis (OA)inBrazilianLongitudinalStudyofAdultHealthMusculoskeletalStudy (ELSA-Brasil MSK).
Materialandmethods:Atest–retestdesignincluding19adults(38kneeimages)was con-ducted.Feasibilityoftheradiographicprotocolwasassessedbyimagequalityparameters andpresenceofradioanatomicalignmentaccordingtointermargindistance(IMD)values. RepeatabilitywasassessedforIMDandjointspacewidth(JSW)measuredatthreedifferent locations.
Results:Approximately90%of kneeimages presented excellentquality.Frequencies of nearlyperfectradioanatomicalignment(IMD≤1mm)rangedfrom29%to50%,and satisfac-toryalignmentwasfoundinupto71%and76%oftheimages(IMD≤1.5mmand≤1.7mm, respectively).Repeatabilityanalysesyieldedthefollowingresults:IMD[SDofmean differ-ence=1.08;coefficientofvariation (%CV)=54.68%; intraclasscorrelationcoefficient(ICC) (95%CI)=0.59(0.34–0.77)];JSW[SDofmeandifference=0.34–0.61;%CV=4.48%–9.80%;ICC (95%CI)=0.74(0.55–0.85)–0.94(0.87–0.97)].AdequatelyreproduciblemeasurementsofIMD andJSWwerefoundin68%and87%oftheimages,respectively.
Conclusions:Despitethedifficultyinachievingconsistentradioanatomicalignmentbetween subsequentradiographsintermsofIMD,theprotocolproducedhighlyrepeatableJSW mea-surementswhentheseweretakenatmidpointand10mmfromthemedialextremityofthe medialtibialplateau.Therefore,measurementsofJSWattheselocationscanbeconsidered adequatefortheassessmentofkneeOAinELSA-BrasilMSK.
©2016PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗
Correspondingauthor.
E-mail:[email protected](R.W.Telles). http://dx.doi.org/10.1016/j.rbre.2016.11.010
A
radiografia
do
joelho
em
flexão
fixa
utilizando
um
novo
posicionador
produziu
medidas
da
largura
do
espac¸o
articular
com
alta
repetibilidade:
estudo
Elsa-Brasil
Musculoesquelético
(ELSA-Brasil
ME)
Palavras-chave:
Radiografiaemflexãofixa Larguradoespac¸oarticular Repetibilidade
Joelho Osteoartrite
r
e
s
u
m
o
Objetivo: Descreverodesempenhodeumprotocoloradiográficoemflexãofixasem fluo-roscopiaemincidênciaPAcomumnovoposicionador,desenvolvidoparaaavaliac¸ãoda osteoartritedejoelho(OA)noestudoELSA-BrasilME.
Materialemétodos: Fez-seumestudodetesteeretestequeincluiu19adultos(38imagens dejoelho).Aviabilidadedoprotocoloradiográficofoiavaliadapormeiodeparâmetrosde qualidadedaimagemepresenc¸adealinhamentoradioanatômicodeacordocomas medi-dasdadistânciaintermarginal(DIM).Avaliaram-searepetibilidadedosvaloresdeDIMea espessuradoespac¸oarticular(EA)emtrêslocaisdiferentes.
Resultados: Aproximadamente90%dasimagensdejoelhoapresentaramumaqualidade excelente.Asfrequênciasde imagenscomalinhamentoradioanatômicoquaseperfeito (DIM<1mm)variaramde29%a50%,edealinhamentosatisfatório(DIM<1,5mme<1,7mm) de 71%a 76%,respectivamente.Asanálisesde repetibilidadeproduziram os seguintes resultados:DIM[DPdamédiadasdiferenc¸as=1,08;coeficientedevariac¸ão(%CV)=54,68%; coeficientedecorrelac¸ãointraclasse(CCI)(IC95%)=0,59(0,34a0,77)];EA[DPdamédiadas diferenc¸as=0,34a0,61;%CV=4,48%a9,80%;CCI(IC95%)=0,74(0,55a0,85)a0,94(0,87a 0,97)].Encontraram-semedidasadequadamentereprodutíveisdeDIMeEAem68%e87% dasimagens,respectivamente.
Conclusões: Apesardadificuldadedeobterumalinhamentoradioanatômicoconsistente entreradiografiasrepetidasem termosdeDIM,oprotocoloproduziu medic¸õesde LEA altamenterepetíveisquandoessasforamtomadasnopontomédioea10mmda extrem-idademedialdoplatôtibialmedial.Portanto,asmedidasdeLEAnesseslocaispodemser consideradasadequadasparaaavaliac¸ãodaOAdejoelhonoestudoELSA-BrasilME.
©2016PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Conventionalknee radiography isthe mostwidely accessi-bleandleastexpensiveimagingtechniquefortheevaluation ofosteoarthriticalterationsinepidemiologicalstudies with long-termfollow-up.1,2Kneejointspacenarrowing(JSN), iden-tifiedbyreductionsinjointspacewidth(JSW)onserialknee radiographs, is considered an adequate proxy of cartilage damageandisfrequentlyusedasamarkerfortheprogression ofkneeosteoarthritis(OA).3,4
ThevalidityofinferencesontheprogressionofkneeOA basedonJSNrequirespreciseandreproduciblemeasurements ofJSW. This is generally achieved byspecific radiographic techniquesdesignedtofacilitateoptimalradioanatomic align-mentbetweenthemedialtibialplateau(MTP)andtheX-ray beam,andtoexposetheregionwherethecartilagedamageis mostnoticeable(i.e.,theposterioraspectoftibiaandfemoral condyle).5
The distance between the anterior and posterior mar-gins of the MTP, known as intermargin distance (IMD), is often used to quantify radioanatomic alignment. Perfect alignment would be present when the MTP and the X-ray beam are parallel, what produces a superimposition ofMTP margins on the radiographic image. Protocolsthat includefluoroscopic guidance are able toachieve a nearly perfectradioanatomicalignment,withIMDvalues≤1mm.6
However,the implementation offluoroscopicprocedures is not straightforward in epidemiological studies because of the limited availability of fluoroscopy in non-specialized radiology services, higher costs, longer examination time, and ahigher dose of ionizing radiation exposure.7 On the other hand, the non-fluoroscopic fixed-flexion PA proto-col is easier to implement and can produce acceptable radioanatomicalignment,withIMDvaluesofupto1.7mm.8 This protocol has also proved capable of providing repro-ducible JSW and IMD measurements.3,9,10 Thus, it is not surprisingthatthe non-fluoroscopic fixed-flexionPA proto-col has been the radiographic method of choice in large cohortsinvestigatingriskfactorsfortheprogressionofknee OA, including theMulticenter Osteoarthritis Study– MOST (http://most.ucsf.edu/studyoverview.asp)andthe Osteoarthri-tisInitiative–OAI(https://oai.epi-ucsf.org/datarelease).More recently,itwas alsochosenfortheassessmentofknee OA intheELSA-BrasilMusculoskeletalStudy(ELSA-BrasilMSK), whichisanancillarystudyoftheBrazilianLongitudinalStudy ofAdultHealth(ELSA-Brasil)aimingtoinvestigateriskfactors for the development and progression of multiple muscu-loskeletaldisorders.11,12Since2012,ELSA-BrasilMSKhasbeen monitoringasubcohortofapproximately2,900publiccivil ser-vants,agedbetween38and79yearsold[mean(SD)56.0(8.9)] atinception.13
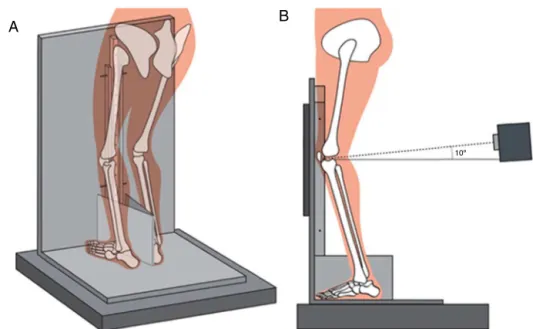
A
B
10º
Fig.1–Schematicillustrationofparticipantpositioningusingthenoveldevice.(A)Obliqueview;(B)lateralview.
cohort data. This includes testing the psychometric prop-erties (feasibility, repeatability, validity and so on) of instruments and examination procedures for the target population.14–20Herewedescribetheperformanceofthe non-fluoroscopic fixed-flexion PA protocol developed foruse in ELSA-BrasilMSK,with respectto feasibilityand repeatabil-ity ofIMD and JSWmeasurements. Thisprotocol included the use of a novel positioning device, and was tested before the start of baseline data collection in ELSA-Brasil MSK.
Material
and
methods
Studydesignandparticipants
The performance of the non-fluoroscopic fixed-flexion PA protocolwasevaluatedinatest–retestdesign.Theinterval betweenrepeated radiographicknee examinationswas7–9 days.Examinationswereperformedbyradiologytechnicians, whounderwentrigoroustraining andcertificationinimage acquisitionaccordingtostudyprocedures,underthe super-vision of an experienced radiologist. A trained radiologist performedradiographicreadingsandmeasurementsofIMD andJSWonadifferentoccasion.
We recruited a convenience sample of adult men and women. Individuals between the ages of 39 and 78 years were considered eligible for inclusion. Thisage range was selectedtoreflectthecharacteristicsofparticipantsincluded inELSA-BrasilMSKatcohortinception.13 Exclusioncriteria wereoccupationalexposuretoradiation(i.e.,reportof wear-ing apersonaldosimeter atwork),confirmed or suspected pregnancy,and participationinELSA-Brasilasastudy sub-ject. Thestudy was approved by the Ethics Committee of the Universidade Federal de Minas Gerais (Approval num-berCEP#1.160.939/CAAE0186.1.203.000-06).Writteninformed consentwasobtainedfromallofthosewillingtoparticipate inthestudy.
Radiographicprotocol
Digitalbilateralkneeradiographswereacquiredusing com-putedradiology(ADC-70;AgfaGevaertNV,Mortsel,Belgium). Focus-film distance was fixed at 72in., and mAs and kVp ranges were20–50and 65–72,respectively.TheX-raybeam was angled10◦ caudaland centeredbetweenthe knees,at the level ofarticular knee spaces (definedbythe popliteal skincrease).21TheangledisplayedontheX-raytubedialwas confirmedbyamagneticinclinometerplacedontopofthe X-raytube(LeeTools,model610056,Houston,US).Participants stood onanoveldevice madeofplexiglasanddesignedto standardizekneepositioninginapproximately20◦offlexion, whiletheanglesubtendedbetweentheinsideofthefeetwas fixedat10◦byav-shapedwedgetippedvertically.22Thedevice wasplacedontopofawoodplatformtoallowthekneestobe centeredonthebucky.Fig.1providesaschematicillustration ofparticipantpositioningusingthedevice.
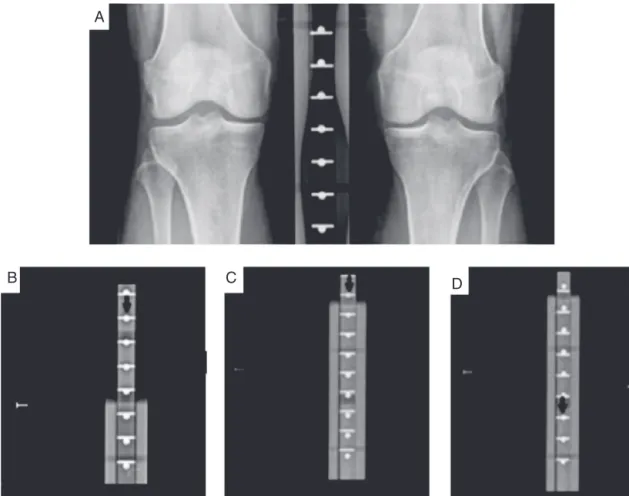
Thisnoveldevicehasadvantagesoverpositioningframes usedinpreviousstudies(e.g.,SynaflexerTMframe),suchasa moveablecomponentthatofferscomfortablepositioningfor adultsofshortstature,andtwosetsofradiopaquemarkers innovativelydistributedforeasierreal-timevisual confirma-tion(withouttheneedofsoftwareorotheraccessories)ofa 10◦ caudalX-raybeamangulationtangentialwiththe knee articular surface.For instance, thecoincidence ofapairof radiopaquemarkersatthearticularkneespacelevelis indica-tiveofproperangulationandcentralizationoftheX-raybeam. Fig.2showsthedistributionpatternofradiopaquemarkers duringadequate(A)andinadequate(B–D)X-raybeam angu-lationand/orcentralization.
Assessmentoffeasibility
A
C
B
D
Fig.2–Distributionofradiopaquemarkersinthenovelpositioningdevice.(A)X-raybeamtangentialtoarticularknee spaceat10◦caudalangulation;(B)X-raybeam2cmabovearticularkneespaceat10◦caudalangulation;(C)X-raybeam tangentialtoarticularkneespaceat12◦caudalangulation;(D)X-raybeamtangentialtoarticularkneespaceat8◦caudal angulation.InB–D,thecoincidenceofapairofradiopaquemarkers(arrow)awayfromthelevelofthearticularkneespace (representedby‘⊢’)isindicativeofinadequateangulationand/orcentralizationoftheX-raybeam.
sidemarker and anatomically relevant structures,(3) knee rotation,and(4)properangulationandcentralizationofthe X-raybeam.Thelatterwasconsidered adequateif device’s radiopaquemarkerscoincideduptoonelevelaboveorbelow thearticularkneespace.Imageswereratedasexcellent(all parameterswereadequate),satisfactory(≥1parameterwas inadequate,but imagecould stillbeanalyzed),or poor(≥1 parameter was inadequate and it was impossible to ana-lyzethe image).Second,the capability ofachieving proper radioanatomicalignment(i.e.,superimpositionbetweenthe anterior and posterior margins ofthe MTP)was evaluated accordingtothefollowingcut-offsforIMD8:1.0mm(nearly perfectorparallelalignment);1.5mmand1.7mm(acceptable alignment).
MeasurementofIMDandJSW
IMD and JSW of images from test and retest were man-ually measured by a single experienced radiologist using image-processing software (OsiriX v.3.9.1, Pixmeo SARL, Geneva, Switzerland). All measurements were performed twice,4-weekapart,withtheradiologistblindtoparticipants’ characteristics and image chronology.Digitalcalipers were placedonselectedlandmarks andthecomputercalculated
thedistanceinmm.IMDwasdefinedasthedistancebetween MTPmargins,measuredatmidpointofthemedial compart-ment (which was identified by the midpoint between two vertical lines: onedrawn at the extremity ofthe MTP and another between the twotibial spines).23 JSWwas defined astheinterbonedistancebetweenthedistalconvexmargin ofthe medialfemoral condyleand the MTP floor,atthree sitesalongthearticularmarginofthemedialcompartment23: perceivednarrowestpoint,midpoint,and10mmfrommedial extremityofMTP(Fig.3).Intra-raterrepeatabilityofIMD mea-surementswasassessedandfoundtobeexcellent(Table1).
Statisticalanalysis
Table1–Repeatabilityofintermargindistance(IMD)andjointspacewidth(JSW)measurements.
Intra-observer Test–retest
SDofmeandifference %CV ICC(95%CI) SDofmeandifference %CV ICC(95%CI)
IMD(mm) 0.16 8.58% 0.99(0.98–1.00) 1.08 54.68% 0.59(0.34–0.77)
JSW(mm)
Midpoint 0.30 3.86% 0.95(0.90–0.97) 0.34 4.48% 0.94(0.87–0.97)
10mm 0.43 6.27% 0.86(0.74–0.92) 0.42 6.29% 0.86(0.75–0.92)
Narrowestpoint 0.57 9.00% 0.77(0.60–0.87) 0.61 9.80% 0.74(0.55–0.85)
SD,standarddeviation;CV,coefficientofvariation;ICC,intraclasscorrelationcoefficient;CI,confidenceinterval.
A C
D
E B
Fig.3–Diagramofmedialtibiofemoralcompartment showingthesiteofmeasurement.Twoverticallineswere drawn,oneattheextremityofthemedialtibialplateau (LineA)andtheotherbetweenthetwotibialspines(Line B).Athirdline(C)wasdrawnatthemidpointbetween thesetwo.Midpointjointspacewidth(JSW)measurements weremadealongthislinebetweentwopointsdefinedas theintersectionbetweenthelineandthefemoralcondyle forthefirst,andthefloorofthetibialplateaufortheother. AdaptedfromRavaudetal.23
calculated. Assuming that an ICC of 0.50 indicates mod-eratereliability,andexpectingasubstantialtonearlyperfect reliability (ICC ≥0.80) of IMD and JSW measurements in thecurrentstudy,asamplesizeof18participants(36knee images)wasrequiredtoprovide astatisticalpowerof90%, witha5%significancelevel.27,28 Consideringapossibleloss of 5%, a sample of 19 participants (38 knee images) was recruited.
Results
Studyparticipants
Fourmenand15womenwereincluded.Thecharacteristics ofthestudysamplewereasfollows:meanage52.1(SD10.1)
years,meanheight164.8(SD7.9)cm,andmeanbodymass index(BMI)26.3(SD4.3)kg/m2.
Feasibilityanalyses
Thevastmajorityofkneeimageswereratedasexcellentby theradiologistateitherthetest(89.5%)ortheretest(84.2%). All theremainingimageswere ratedassatisfactorydueto excessivekneerotation.ThemeanIMDwas1.33(SD1.13)mm and1.38(SD1.14)mmattestandretest,respectively. Frequen-ciesofnearlyperfectradioanatomicalignment(IMD≤1.0mm) were 19 (50.0%)attest, 18 (47.4%)atretest, and11 (28.9%) atbothtime-points.Frequenciesofacceptableradioanatomic alignmentaccordingtolessconservativecut-offsforIMDwere as follows:1.5mm cut-off:24 (63.2%)at test, 27 (71.1%)at retest,and21(55.3%)atbothtime-points;1.7mmcut-off:29 (76.3%)ateithertestorretest,and26(68.4%)atboth time-points.
Test–retestrepeatabilityofIMDandJSWmeasurements
Overall,test–retestrepeatabilityparametersforIMD measure-mentwerefair.Forexample,theSDofmeandifferenceand %CV were 1.08 and 54.68%, respectively (Table 1). An ade-quatelyrepeatableIMD(i.e.,test–retestvariation≤1mm)was observedin68.4%oftheknees.
JSWrepeatabilityparametersweregoodtoexcellent.JSW measurements taken at midpoint of the medial compart-ment were consistently morerepeatable than those taken atother sites. For example,the SDofthe mean difference ofJSWmeasurementsbetweentestandretestwas0.08mm (23.5%)and0.27mm(79.4%)higherforJSWmeasured10mm fromthemedialextremityoftheMTPandatthenarrowest point ofthe medialcompartment,respectively, when com-paredtoJSWmeasured atmidpoint(Table1). Additionally, adequately repeatable JSW measurements were also more frequentwhentheyweretakenatmidpoint:i.e.,test–retest variations ≤0.5mmwere observed in86.9%ofknees when JSWwasmeasuredatmidpoint,84.2%ofkneeswhenitwas measuredat10mm,and78.9%ofkneeswhenmeasureswere takenatthenarrowestpoint.
Discussion
epidemiologicstudyonchronicnon-communicablediseases (NCDs) conducted in a Latin American country.29,30 We describedtheperformancethenon-fluoroscopicfixed-flexion PAprotocol selectedforthe assessmentofknee OA inthe ancillarystudyELSA-BrasilMSK.
Feasibilityoftheradiographicprotocolusingthenew posi-tioningdevicewasfoundtobeadequate,withapproximately 90%ofkneeimagesbeingratedasexcellentatanytime-point. Ontheotherhand,theprotocolwasabletoproduceaparallel alignmentbetweenMTPmargins(i.e.,IMD≤1mm)inonlyhalf ofthekneeimagesfromeitherthetestortheretest.Although disappointingatfirstglance,thisresultisinaccordancewith priorobservationsfromBotha-Scheepersandcolleagues,who foundparallelradioanatomicalignmentinupto51%ofimages acquiredbyasimilarradiographicprotocol.3Additionally,the frequencyofanearlyperfectalignmentatbothtime-points (testandretest)inourstudywaswithintherangedescribed intheliteratureforradiographicprotocolsofthekneewithout fluoroscopy:11%–42%.3,8,31Weconsiderthisaveryimportant findinggiventhatthequalityofMTPalignmentonserial radio-graphsisknowntoinfluencethecapabilityofidentifyingrisk factorsfortheprogressionofJSNinlongitudinalstudies inves-tigatingkneeOA.32
Thedifficulty in achieving parallelradioanatomic align-mentisinherenttonon-fluoroscopicprotocols.Forexample, priorstudies have found IMD valuestwice as largein the non-fluoroscopic fixed-flexion PA protocol when compared totheLyonSchussview.31Forthisreason,lessconservative cut-offs for IMD are considered acceptable in the absence offluoroscopy.8Wefound55%ofacceptableradioanatomic alignment at both test and retest when the cut-off was set at 1.5mm, a result superior to that reported in pre-vious studies: for example, an IMD lower than 1.5mm at both time-pointswas observed in only 12% ofthe images inthe study of Nevittand colleagues33 and in34% ofthe imagesinthestudyofLeGraverandandcolleagues.31Finally, when considering the 1.7mm cut-off foracceptable align-ment,achievingthisgoalatbothtime-pointswasalmost40% morefrequentinourstudythaninthestudyofVignonand colleagues.8
Althoughourprotocolwassomewhatsuperiorin produc-ing knee images with acceptable radioanatomic alignment when compared to non-fluoroscopic protocols used in previous studies, repeatability parameters for our IMD measurements were found to be fair. Nevertheless, IMD values classified as adequately repeated (test–retest varia-tion ≤1mm) were still more frequent in our study than inanother high-qualitycohort study investigatingrisk fac-torsfortheprogressionofkneeOA:ELSA-BrasilMSK68.4% versus Osteoarthritis Initiative 57.6%.25 It is possible that variationsofupto1mminIMD betweenconsecutiveknee radiographscompriseanexcessivelyconservativetargetfor non-fluoroscopicprotocols,whichwouldnotalwaysproducea relevantimpactonthereproducibilityofJSWmeasurements. Thisissupportedbyourfindings oftrivialtest–retest vari-ations(≤0.5mm)forthevast majority(approximately80%) of knee images. Although uncommon, a poor association betweenproper MTP alignmentand reproducibilityof JSW measurementshasbeenreportedbyafewstudies investigat-ingsimilarradiographicprotocols.33,34
Interestingly, JSW repeatability differed considerably accordingtothesiteofmeasurement.JSWmeasuredat mid-pointandat10mmfromthemedialextremityofMTPwere morerepeatablethanJSWmeasuredatthenarrowestpoint. Repeatability was particularly increasedfor JSW measures atmidpoint,andthismaybeexplainedbyamoreaccurate identification of relevant landmarks during the manual measurement of JSW at this site. Additionally, precision limitationsofthedigitalcalipersfromtheimage-processing softwaremayalsopredisposetogreatervariabilitywhenJSW is measured atthe narrowest point. Taken together, these findingsareofgreatimportanceforfuturestudiesconsidering manualmeasurementofJSWtoinferabouttheprogression ofkneeOA.
Our study has strengths and limitations that need to be acknowledged. First, the non-fluoroscopic fixed-flexion PA knee radiographs followed rigorous quality procedures, including theuseofpre-definedprotocolsforimage acqui-sition and reading, and ahighly trained staff.Second, our resultsprovidedsupportforthe use ofanoveldevice that standardizeskneepositioningduringtheexamination,while allowing areal-timeevaluationofkey radiographic param-eters.Theincorporationofthisrelativelylow-costdevicein studiesofosteoarthriticalterationsconductedinBrazilcould increasetheirscientificpotential,giventhattheaccesstothe importedtechnologiesalreadyavailableisnotstraightforward andcanbeextremelycostly.Themainlimitationofourstudy isthelackofinformationontheperformanceofthe radio-graphicprotocoloverlongerperiodsoftime.Forinstance,itis possiblethatfactorsrelatedtotheexaminersorparticipants (e.g.,changesinkneeanatomy,worseningofsymptoms)may impact the performanceofthe protocol inepidemiological studieswithalong-termfollow-up.33
Inconclusion,theperformanceofanon-fluoroscopic fixed-flexionPAprotocolwithanewpositioningdevicewasfound tobesatisfactoryformeasurementsofJSWtakenatmidpoint and10mmfromthemedialextremityoftheMTP.This pro-videssupportforthe incorporationofthesemeasurements during theassessment ofknee OA inthe ELSA-BrasilMSK cohort.Furtherinvestigationswithinthecohortwillbeable totesttheprecisionandaccuracyoftheradiographicprotocol overthelongterminalargerandmoreheterogeneoussample.
Funding
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthorswouldliketothankthemanagementandstaff oftheradiologyserviceClínicaRadiológicaJavertBarrosfortheir valuableassistanceinthisstudy,inspecialtoDr.EvandroBarros Naves.
r
e
f
e
r
e
n
c
e
s
1. GuermaziA,HayashiD,RoemerFW,FelsonDT.Osteoarthritis: areviewofstrengthsandweaknessesofdifferentimaging options.RheumDisClinNAm.2013;39:567–91.
2. NelsonAE,RennerJB,ShiXA,ShrefflerJH,SchwartzTA, JordanJM.Cross-sectionalcomparisonofextended
anteroposteriorandposteroanteriorfixedflexionpositioning toassessradiographicosteoarthritisattheknee:theJohnston CountyOsteoarthritisProject.ArthritisCareRes(Hoboken). 2010;62:1342–5.
3. Botha-ScheepersS,KloppenburgM,KroonHM,HellioLe GraverandMP,BreedveldFC,RavaudP,etal.Fixed-flexion kneeradiography:thesensitivitytodetectkneejointspace narrowinginosteoarthritis.OsteoarthrCartil.2007;15:350–3. 4. AltmanRD,FriesJF,BlochDA,CarstensJ,CookeTD,GenantH,
etal.Radiographicassessmentofprogressionin osteoarthritis.ArthritisRheum.1987;30:1214–25. 5. HellioLeGraverandMP,MazzucaS,DuryeaJ,BrettA.
Radiographicgradingandmeasurementofjointspacewidth inosteoarthritis.RheumDisClinNAm.2009;35:485–502. 6. Buckland-WrightJC,BirdCF,Ritter-HrncirikCA,ClineGA,
TonkinC,HangartnerTN,etal.X-raytechnologists’
reproducibilityfromautomatedmeasurementsofthemedial tibiofemoraljointspacewidthinkneeosteoarthritisfora multicenter,multinationalclinicaltrial.JRheumatol. 2003;30:329–38.
7. MazzucaSA,HellioLeGraverandM-P,VignonE,HunterDJ, JacksonCG,KrausVB,etal.Performanceofa
non-fluoroscopicallyassistedsubstitutefortheLyonSchuss kneeradiograph:qualityandreproducibilityofpositioning andsensitivitytojointspacenarrowinginosteoarthritic knees.OsteoarthrCartil.2008;16:1555–9.
8. VignonE,BrandtKD,MercierC,HochbergM,HunterD, MazzucaS,etal.Alignmentofthemedialtibialplateau affectstherateofjointspacenarrowingintheosteoarthritic knee.OsteoarthrCartil.2010;18:1436–40.
9. ReichmannWM,MaillefertJF,HunterDJ,KatzJN,Conaghan PG,LosinaE.Responsivenesstochangeandreliabilityof measurementofradiographicjointspacewidthin osteoarthritisoftheknee:asystematicreview.Osteoarthr Cartil.2011;19:550–6.
10.KothariM,GuermaziA,vonIngerslebenG,MiauxY,Sieffert M,BlockJE,etal.Fixed-flexionradiographyoftheknee providesreproduciblejointspacewidthmeasurementsin osteoarthritis.EurRadiol.2004;14:1568–73.
11.TellesRW,SilvaLC,MachadoLA,BarretoSM.Investigating osteoarthritisinasubcohortoftheBrazilianLongitudinal StudyofAdultHealth:theELSA-BrasilMusculoskeletalStudy (ELSA-BrasilMSK).OsteoarthrCartil.2016;24:S210–1. 12.AquinoEM,BarretoSM,BensenorIM,CarvalhoMS,ChorD,
DuncanBB,etal.BrazilianLongitudinalStudyofAdultHealth
(ELSA-Brasil):objectivesanddesign.AmJEpidemiol. 2012;175:315–24.
13.MachadoLAC,TellesRW,Costa-SilvaL,BarretoSM.Perfilda CoorteElsa-BrasilMusculoesquelético.BrazJRheumatol. 2015;56Suppl.1:S29–30.
14.NunesMA,AlvesMGM,ChorD,SchmidtMI,DuncanBB. Cross-culturaladaptationofCIS-R(ClinicalInterview Schedule-RevisedVersion)forthePortugueseinLongitudinal StudyofAdultHealth(ELSA).RevHCPA.2011;31:515–8. 15.GriepRH,AquinoEM,ChorD,KakeshitaIS,GomesAL,Nunes
MA.Test–retestreliabilityofthescalesilhouettesfiguresof bodyimageinBrazilianLongitudinalStudyofAdultHealth. CadSaúdePública.2012;28:1790–4.
16.ChorD,AlvesMG,GiattiL,CadeNV,NunesMA,MolinaMdel C,etal.QuestionnairedevelopmentinELSA-Brasil:
challengesofamultidimensionalinstrument.RevSaúde Pública.2013;47Suppl.2:27–36.
17.GriepRH,SantosSM,CardosoLdeO,FonsecaMdeJ,AlvesMG, SoutoEP,etal.SocialcapitalinELSA-Brasil:test–retest reliabilityoftheResourceGeneratorscale.RevSaúdePública. 2013;47Suppl.2:131–9.
18.MolinaMdelC,BensenorIM,CardosoLdeO, Velasquez-MelendezG,DrehmerM,PereiraTS,etal. ReproducibilityandrelativevalidityoftheFoodFrequency QuestionnaireusedintheELSA-Brasil.CadSaúdePública. 2013;29:379–89.
19.SantosSM,GriepRH,CardosoLO,AlvesMG,daFonsecaMdeJ, GiattiL,etal.Cross-culturaladaptationandreliabilityof measurementsonself-reportedneighborhoodcharacteristics inELSA-Brasil.RevSaúdePública.2013;47Suppl.2:122–30. 20.MachadoL,TellesR,Costa-SilvaL,BarretoS.Psychometric
propertiesofMultidimensionalHealthLocusofControl ScalesandtheGeneralSelf-EfficacyScale:theELSA-Brasil MusculoskeletalStudy(ELSA-BrasilMSK).BrazJPhysTher. 2016;20:451–60.
21.PeterfyC,LiJ,ZaimS,DuryeaJ,LynchJ,MiauxY,etal. Comparisonoffixed-flexionpositioningwithfluoroscopic semi-flexedpositioningforquantifyingradiographic joint-spacewidthintheknee:test–retestreproducibility. SkeletRadiol.2003;32:128–32.
22.MachadoL,Costa-SilvaL,BarretoS,TellesR,NavesE, CarneiroA.Positionerfortheacquisitionandqualitycontrol ofradiographicimagesofkneesinthefixedflexionposition (radiolfixer).InventionpatentINPIBR102013033625-4; InternationalapplicationnumberPCT/IB2014/067387;2014. 23.RavaudP,ChastangC,AuleleyGR,GiraudeauB,RoyantV,
AmorB,etal.Assessmentofjointspacewidthinpatients withosteoarthritisoftheknee:acomparisonof4measuring instruments.JRheumatol.1996;23:1749–55.
24.BlandJM,AltmanDG.Statisticalmethodsforassessing agreementbetweentwomethodsofclinicalmeasurement. Lancet.1986;1:307–10.
25.MercierC,PipernoM,VignonE,BrandtK,HochbergM,Hellio LeGraverandMP.Innormalknees,jointspacewidth(JSW)is correlatedwiththeintermargindistance(IMD),ameasureof medialtibialplateaualignment.VariationsinIMDexplain variabilityinJSWinserialradiographs.JtBoneSpine. 2013;80:183–7.
26.ClineGA,MeyerJM,StevensR,Buckland-WrightC,PeterfyC, BearyJF.Comparisonoffixedflexion,fluoroscopicsemi-flexed andMTPradiographicmethodsforobtainingtheminimum medialjointspacewidthofthekneeinlongitudinal
osteoarthritistrials.OsteoarthrCartil.2006;14Suppl.A:A32–6. 27.ZouGY.Samplesizeformulasforestimatingintraclass
correlationcoefficientswithprecisionandassurance.Stat Med.2012;31:3972–81.
29.DepartmentodeCiênciaeTecnologia–MinistériodaSaúde. ELSABrasil:thegreatestepidemiologicalstudyinLatin America.RevSaúdePública.2009;43:1–2.
30.SchmidtMI,DuncanBB,MillJG,LotufoPA,ChorD,Barreto SM,etal.Cohortprofile:longitudinalstudyofadulthealth (ELSA-Brasil).IntJEpidemiol.2015;44:68–75.
31.LeGraverandMP,VignonEP,BrandtKD,MazzucaSA,Piperno M,BuckR,etal.Head-to-headcomparisonoftheLyonSchuss andfixedflexionradiographictechniques.Long-term reproducibilityinnormalkneesandsensitivitytochangein osteoarthriticknees.AnnRheumDis.2008;67:1562–6. 32.Botha-ScheepersS,DougadosM,RavaudP,HellioLe
GraverandMP,WattI,BreedveldFC,etal.Effectofmedial
tibialplateaualignmentonserialradiographsonthecapacity topredictprogressionofkneeosteoarthritis.Osteoarthr Cartil.2008;16:272–6.
33.NevittMC,PeterfyC,GuermaziA,FelsonDT,DuryeaJ, WoodworthT,etal.Longitudinalperformanceevaluationand validationoffixed-flexionradiographyofthekneefor detectionofjointspaceloss.ArthritisRheum. 2007;56:1512–20.