BrazJOtorhinolaryngol.2017;83(6):723---725
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
CASE
REPORT
A
case
of
bilateral
congenital
middle
ear
cholesteatoma
夽
,
夽夽
Um
caso
de
colesteatoma
congênito
bilateral
em
orelha
média
Mihael
Ries
a,∗,
Mirjana
Kosti´
c
b,
Jakov
Ajduk
a,
Robert
Troti´
c
a,
Vladimir
Bedekovi´
c
aaUniversityofZagreb,UniversityHospitalCenter‘‘SestreMilosrdnice’’,SchoolofMedicine,DepartmentofENTHeadandNeck
Surgery,Zagreb,Croatia
bUniversityofZagreb,CroatianHealthInsuranceFund,SchoolofMedicine,Zagreb,Croatia
Received31July2015;accepted29September2015 Availableonline17December2015
Introduction
Bilateral middle ear congenital cholesteatoma (CC) is an extremelyraredisease.1---3
Middle ear CC growsfrom birth behind the intact ear
drum,withnosymptoms.Usually,itisdetectedbythe
pedi-atricianatthetimeofaroutinevisit.1---3Undetected,itmay
growforyearsuntilbecomingquitelarge.
Etiology of middle ear CC is still controversial, but it
seemsthatanembryologicoriginisthemostacceptable.1---3
Progressivehearinglossandsofttissuedensitymasswithin
themiddleearcavityusuallydifferentiatetheCCfromother
pathologies that includehearing loss and intacttympanic
membrane.4 Treatment of CC requires early surgery and
夽
Please cite this article as: Ries M, Kosti´c M, Ajduk J, Troti´cR, Bedekovi´c V.A caseofbilateralcongenital middleear cholesteatoma.BrazJOtorhinolaryngol.2017;83:723---5.
夽夽
Institution:UniversityofZagreb,SchoolofMedicine, Depart-mentof ENTHead and Neck Surgery,UniversityHospitalCenter ‘‘SestreMilosrdnice’’,Zagreb,Croatia.
∗Correspondingauthor.
E-mail:[email protected](M.Ries).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileirade OtorrinolaringologiaeCirurgiaCérvico-Facial.
long-termfollow-up.5SpreadandlocationofCCinfluences
theoutcomeofsurgery.
Recently,twocasesof CCspontaneousregressionwere
described.6
Case
report
A3-year-oldboywasadmittedtothehospitalduringhisfirst
episodeofright-sidedacuteotitismedia(AOM),
accompa-niedbydiscretefacialnervepalsy(House-BrackmannGrade
II)onthesideoftheinvolvedear.
Otomicroscopy showed a red, bulging tympanic
mem-brane on the right side, without perforation. The left
tympanic membrane was normal. Myringotomy was
per-formed as a medical urgency, with no preoperative
radiologicexam.Duringmyringotomy,alargecholesteatoma
wasdiscovered in the middle ear cavity. For a complete
surgical removal of the cholesteatoma and facial nerve
decompressionacanalwalldown(CWD)techniquewas
nec-essary.Facialnervehasimprovedaftersixmonths.
Afteroneyear,routineotoscopicfollow-upshoweda
nor-malpostoperativefindingontheright ear,butonthe left
ear,awhite pearlin theanterosuperior quadrant,behind
theintacttympanicmembrane,wasdetected.Again,there
wasnohistory of otitismedia or evidence of anytrouble
withtheboy’sleftear.
http://dx.doi.org/10.1016/j.bjorl.2015.09.003
724 RiesMetal.
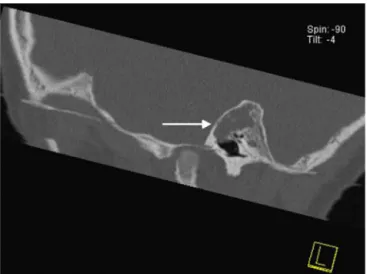
Figure1 CoronalMDCTscanofthelefttemporalbone show-ingaerated mesotympanum andthe soft tissuemass around malleusheadandincusbody(arrow).
Multidetectorcomputedtomography(MDCT)scanofthe
temporal bone confirmed that there was no sign of
dis-ease recurrence on the right side. On the left side, a
massintheepitympanumsuspiciousofcholesteatomawas
discovered (Figs. 1---4). Surgery confirmed the diagnosis,
Figure2 AxialMDCTscanofthelefttemporalboneatthe levelofthehorizontalportionofthefacialnerve(arrow), show-ingthesofttissuemassintheatticandantrum.
Figure3 SagittalMDCTscanofthelefttemporalboneatthe levelofmalleushandle,showingthesofttissuemassintheattic (arrow).
and cholesteatoma was removed through retroauricular
approach,canalwalluptechnique(CWU).
Discussion
Bilateral middle ear CC is a very rare disease. The most
common symptom of a conventional cholesteatoma is a
purulenteardischargewithastrongodororbleeding.Most
frequent signs of complication include vertigo, tinnitus,
sensorineuralhearinglossandfacialnervepalsy.1---3Surgery
is necessary.1---5 Spread of the disease and presence of
potentialcomplicationsdictatethefinaloutcome.
Our patient had no history of previous ear infection,
traumaorearsurgery.Theright-sidedAOMmasked,andat
thesametimerevealed,alargemiddleearcholesteatoma.
Thefacialnervepalsyonthesideoftheinvolvedearwasa
resultofthefacialnervedamagecausedbycholesteatoma
pressureaccentuatedbyinflammatoryedema.
Urgent surgery was necessary to prevent permanent
facial nerve damage. Removal of the cholesteatoma was
donebyCWDtechnique.Thisunpopulartechniquewas
cho-sen because the disease presented itself already through
a complication, so any future unrecognized recurrence
could lead to irreparable facial nerve damage. The
dis-ease haseroded ossicles andthe bonycanal of thefacial
nerve in its horizontal segment, above the stapes
foot-plate.Cholesteatomaspreadtotheauditorytube,anterior
attic, antrum, and posteriorly and medially to the
lat-eral semicircular canal, threatening with inner ear and
intracranialcomplications.Thiscaseconfirmedthefactthat
the otomicroscopy is insufficientfor detecting middle ear
cholesteatoma,especiallywhenthereisnoeardrum
perfo-rationornearbybonydefect.
Contralateral middle ear CC was detected by a
post-operative MDCT,performed onthegroundsof asuspicious
otomicroscopyfindingduringtheregularfollow-up.The
dis-ease could be removed by CWU technique, for it was of
amuchsmaller extentcomparedtothecontralateralear.
Pathologywaslocatedmostlyintheattic,aroundtheincus
Acaseofbilateralcongenitalmiddleearcholesteatoma 725
Figure4 Sagittalscanofthelefttemporalboneshowingthe softtissuemassintheatticandaeratedmesotympanum.
tympanior facialrecess.Theossicularchainandtympanic
membraneremainedintact. Norecurrenceof diseasewas
notedduringa36-monthfollow-up.
Had theMDCTbeendone beforeorsoon afterthefirst
surgery, thebilateral diseasewouldhave been discovered
muchearlier. On the other hand, MDCTis notand should
notbeperformedasaroutineinpatientswithAOMwhoare
candidatesforurgentmyringotomy,butitshouldbea
rou-tine inpatients with CC.Nevertheless, MDCT is surelyan
importantbutunder-indicateddiagnosticprocedurethatis
soveryusefulfor surgicalplanning.Manysurgeonsrelyon
experienceand routineinmiddle earoperations. By
indi-catingmoreradiologicexaminationsofthetemporalbone
surgeonscouldpreparethemselvesbetterforsurgeryand,
atthesametime,keepradiologiststrainedininterpreting
thiscomplexanatomyandpathology.
Conclusion
Bilateralmiddleearcongenitalcholesteatomaisaveryrare
entity.
ItisimportanttonotethatafterthediscoveryofCCon
oneear,bilateraldiseasemustberuledout.CC,justasthe
acquiredcholesteatomadoes,requiresathoroughsurgical
removalandalong-termfollow-up.Extensionandlocation
ofthedisease dictates thetypeof surgeryandfunctional
outcome.MDCTisamethodofchoicefordiagnosingahidden
bilateralmiddleearCC.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Potsic WP, Korman SB, Samadi DS, Wetmore RF. Congenital cholesteatoma:20years’experienceatTheChildren’sHospital ofPhiladelphia.OtolaryngolHeadNeckSurg.2002;128:810---4.
2.Bennett M, Warren F, Jackson GC, Kaylie D. Congenital cholesteatoma:theories,factsand53patients.OtolaryngolClin NorthAm.2006;39:1081---94.
3.Koltai PJ,Nelson M,CastellonRJ, Garabedian EN, Triglia JM, RomanS,etal.Thenaturalhistoryofcongenitalcholesteatoma. ArchOtolaryngolHeadNeckSurg.2002;128:804---9.
4.KimSH,ChoYS,ChuHS,JangJY,ChungWH,HongSH.Open-type congenital cholesteatoma: differential diagnosis for conduc-tive hearing loss with a normal tympanic membrane. Acta Otolaryngol.2012;132:618---23.
5.El-BitarMA,ChoiSS,EmamianSA,VezinaLG.Congenitalmiddle earcholesteatoma:needforearlyrecognition---roleofcomputed tomographyscan.IntJPediatrOtorhinolaryngol.2003;67:231---5.