www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Significant
association
between
osteoporosis
and
hearing
loss:
a
systematic
review
and
meta-analysis
夽
Sikarin
Upala
a,b,
Pattara
Rattanawong
c,
Wasawat
Vutthikraivit
c,
Anawin
Sanguankeo
a,b,∗aBassettMedicalCenterandColumbiaUniversityCollegeofPhysiciansandSurgeons,DepartmentofInternalMedicine,
Cooperstown,UnitedStates
bMahidolUniversity,FacultyofMedicineSirirajHospital,DepartmentofPreventiveandSocialMedicine,Bangkok,Thailand cUniversityofHawaii,DepartmentofInternalMedicine,Honolulu,UnitedStates
Received23May2016;accepted22August2016 Availableonline12September2016
KEYWORDS
Osteoporosis; Hearingloss; Meta-analysis
Abstract
Introduction:Thereisinconclusiveevidencewhetherosteoporosisincreasesriskofhearingloss incurrentliterature.
Objective:We conducted this meta-analysis to determine whether there is an association betweenhearinglossandosteoporosis.
Methods:Thissystematicreviewandmeta-analysiswasconductedfromstudiesofMEDLINE, EMBASE,andLILACS.OsteoporosiswasdefinedashavingabonemineraldensitywithaT-score oflessthan−2.5standarddeviation.Theoutcomewashearinglossasassessedbyaudiometry
orself-reportedassessment.Random-effectsmodelandpooledhazardratio,riskratio,orodds ratioofhearinglosswith95%confidenceintervalswerecomparedbetweennormalbonemineral densityandlowbonemineraldensityorosteoporosis.
Results:Atotalof16articlesunderwentfull-lengthreview.Overall,therewasastatistically sig-nificantincreasedoddsofhearinglossinthelowbonemineraldensityorosteoporosisgroupwith oddsratioof1.20(95%confidenceintervals1.01---1.42,p=0.04,I2=82%,P
heterogeneity=0.01).
However,thestudyfromHelzneretal.reportedsignificantlyincreaseoddsofhearinglossin thelowbonemineraldensityinparticularareaandpopulationincludedfemoralneckofblack men1.37(95%confidenceintervals1.07---1.76,p=0.01)andtotalhipofblackmen1.36(95% confidenceintervals1.05---1.76,p=0.02).
Conclusion:Ourstudyproposedthefirst meta-analysisthatdemonstratedaprobable associ-ationbetween hearinglossandbonemineraldensity. Osteoporosiscouldbeariskfactorin hearinglossandmightplayanimportantroleinage-relatedhearingloss.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽
Pleasecitethisarticleas:Upala S,RattanawongP,VutthikraivitW,SanguankeoA.Significantassociationbetweenosteoporosisand hearingloss:asystematicreviewandmeta-analysis.BrazJOtorhinolaryngol.2017;83:646---52.
∗Correspondingauthor.
E-mail:[email protected](A.Sanguankeo).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.08.012
Osteoporosisandhearingloss 647
PALAVRAS-CHAVE
Osteoporose; Perdaauditiva; Metanálise
Associac¸ãosignificativaentreosteoporoseeperdaauditiva:umarevisãosistemática
emetanálise
Resumo
Introduc¸ão: Háevidênciasinconclusivassobreseaosteoporoseaumentaoriscodeperda audi-tivanaliteraturaatual.
Objetivo: Realizamosestametanáliseparadeterminarseexisteumaassociac¸ãoentreperda auditivaeosteoporose.
Método: Revisão sistemáticaemetanálise foramrealizadas apartirde estudosdoMedline,
Embase e Lilacs.A osteoporose foidefinida como tendouma densidade mineralóssea com
umescoreTdemenosque-2,5DP.Odesfechofoiaperdaauditiva,avaliadaporaudiometria ouavaliac¸ãoautorrelatada.Omodelodeefeitosaleatórioseriscocombinado,razãoderisco eoddsratiodeperdaauditivacomIntervalosdeConfianc¸ade95%foramcomparadosentre densidademineralósseanormaledensidademineralósseabaixaouosteoporose.
Resultados: Nototal,16artigosforamsubmetidosarevisãocompleta.Emgeral,houveaumento estatisticamentesignificativodaprobabilidadedeperdaauditivanogrupodebaixadensidade mineralósseaounogrupodeosteoporosecomoddsratiode1,20(intervalodeconfianc¸ade95% 1,01-1,42,p=0,04,p=82%,Pheterogeneidade=0,01).Noentanto,oestudodeHelzneretal.relatou
aumentosignificativodaprobabilidadedeperdaauditivanadensidademineral ósseabaixa, emdeterminadaáreaepopulac¸ãoqueincluiucolofemoraldehomensnegros1,37(intervalo deconfianc¸ade95%1,07-1,76,p=0,01) equadriltotaldehomensnegros1,36(intervalode confianc¸ade95%1,05-1,76,p=0,02).
Conclusão:Nossoestudopropôsaprimeirametanálisequedemonstrouumaprovávelassociac¸ão entreperdaauditivaedensidademineralóssea.Aosteoporosepodeserumfatorderiscopara perdaauditivaepodedesempenharumpapelimportantenaperdadeaudic¸ãorelacionadacom aidade.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Hearing lossis acommonchronic condition ofa disability estimatedat24.9millionpeopleworldwide.Itwasreported by The World Health Organization as one of the leading causesofyearslivedwithdisability.1Theestimated preva-lenceofhearinglosswas30%inthepopulationover65years oldand50%inthepopulationover75yearsold.2,3Moreover, hearinglossisalsoassociatedwithdecreasingqualityoflife andfunctionaloutcomesincludingsocialisolation, depres-sion,safetyissues,mobilitylimitations,reducedincomeand employmentopportunities.4---7 Riskfactorsinfluencetothe degree and rate of deterioration of hearing loss include aging,geneticsusceptibility,ototoxicmedicationexposure, otologicaldisorders,smoking,andoccupationalandleisure noiseexposure.6,8---10
Osteoporosishasalsobeenidentifiedinsomestudiesas a risk factor of hearing loss. The underlying mechanism of hearing loss in osteoporosis is complex and undeter-mined. Some studies purposed that a possible underlying mechanism is systemic demineralization of the skeletal systeminosteoporosisincludestemporalbone,which con-tains thecochlea capsule andthe conductivesystem.11---13 However,therewerecontroversiesandinconsistentresults fromotherstudies thatshowednon-significantassociation betweenosteoporosisandhearingloss.Theaccuracyofthe results was limited due to the sample sizes of the study populations.2Therefore,weconductedthismeta-analysisto determinewhetherthereisanassociationbetweenhearing lossandlowbonemassorosteoporosis.
Materials
and
methods
This systematic review and meta-analysis was conducted and reported according to the Meta-analysis Of Observa-tionalStudies in Epidemiologystatement14 andwas regis-teredinPROSPERO(registrationnumber:CRD42015024987).
Searchstrategy
Two authors (AS, SU) independently searched published studies indexed in the MEDLINE, EMBASE, and LILACS (Literatura LatinoAmericanaem CiênciasdaSaúde) from theirdateofinceptiontoNovember2015.Referencesofall selectedstudies were also examined. The following main search terms were used: osteoporosis, osteopenia, bone density, bone mass, bone loss, hearing loss, audiometry, otoacoustic. The full search strategy was detailed in Appendix1.
Inclusionandexclusioncriteria
lowBMD or osteoporosis andhearingloss wasreportedas either adjusted or unadjusted hazard ratios (HRs), rela-tive risks (RRs), or odds ratios (ORs) with associated 95% confidenceintervals(CIs),orhearingsensitivityindecibels. Exclusioncriteriawere(1)reviews,casereports,abstracts, andunpublished studies,(2) studieswithout specific sam-pleorigins,(3)datainthestudywasnotpresentedclearly enough,and(4)participantswithknownotosclerosis.
Osteoporosiswasdefinedashavingabonemineral den-sity(BMD)withaT-scoreoflessthan−2.5SDasmeasured bydual-energyX-rayabsorptiometryorotherstandard tech-nique at anatomical bone sites including lumbar spine, femoralneck,andtotalhip.Themainoutcomeofthisstudy washearinglossasassessedbyaudiometryorself-reported assessment.Weusedthedefinitionofhearingloss (conduc-tive,sensorineural,ormixed)asdescribedbyeachstudy.
Dataextraction
Twoauthors(ASandSU)independentlyreviewedtitlesand abstracts of all citations that were identified. After all abstracts were reviewed, data comparisons between the twoinvestigators wereconductedtoensurecompleteness and reliability. The inclusion criteria were independently applied to all identified studies. Differingdecisions were resolvedbyconsensus.
Full-text versions of potentially relevant papers iden-tified in the initial screening were retrieved. If multiple articlesfromthesamestudy werefound, onlythe article with the most complete data was included. Data con-cerningstudydesign,participantcharacteristics,sourceof data,comorbidities,methodsofassessingBMDandhearing impairment,outcomeassessment, andfactorsadjusted in multivariableanalysiswereindependentlyextracted.
Assessmentofquality
Asubjectiveassessmentofmethodologicalqualityfor obser-vationalstudieswasevaluatedbytwoauthors(ASandSU) usingtheNewcastle---OttawaScale(NOS).TheNOSisa qual-ity assessment tool for non-randomized studies. The NOS includeseightitems,categorizedintothreedimensionsof selection,comparability,andoutcome.Foreachdimension, alistofresponseoptionsisprovided.Scoringisbasedona semi-quantitativeassessmentofstudy quality.The highest qualitystudiesarescoredamaximumofonepointforeach item.However,thereis an exception ofthe item related tocomparabilitythatallowstheassignmentoftwopoints. The range of NOS is between zero up to nine points.15 A totalscoreof 3orlesswasconsideredpoor,4---6 was con-sidered moderate, and 7---9 was deemed high quality. We excluded studies fromour meta-analysisif theyhad poor quality.Discrepantopinionsbetweenauthorswereresolved byconsensus.
Statisticalanalysis
Weperformed meta-analysisof theincluded studies using Comprehensive Meta-Analysis 3.3 software from Biostat, Inc. We used a random-effects model if there was high
heterogeneity(I2>50%)andfixed-effectsmodeliftherewas
lowheterogeneity(I2<50%).WecalculatedpooledHR,RR,
orORofhearinglosswith95%confidenceintervals(CI) com-paringbetweenparticipantswithnormalBMDandwithlow BMD or osteoporosisat each anatomicalsiteandwithany anatomicalsites.Wealsocalculatedpooledmeandifference (MD) with95% CI of hearingsensitivity in each frequency comparing between the normal BMD group and the low BMD group. We excluded studies from meta-analysis and only presentedthe resultwithnarrativedescription when therewerenotsufficientcomparabledataavailablefor out-comeofinterest.Theheterogeneityofeffectsizeestimates acrossthesestudieswasquantifiedusingtheQstatistic,its p-value, and I2 (p<0.10 was considered significant).
Sub-group analysis by site of BMD was performed to find the sourceofheterogeneity.Publicationbiaswasassessedusing funnelplotandEgger’sregressiontest.
Results
Descriptionofincludedstudies
The initial search yielded 83 articles (Fig. 1); 67 articles wereexcludedbecausetheywerenotoriginalobservational studies (23articles), didnothave BMD data (12articles), didnothavehearinglossdata(6articles),ordidnot mea-sureassociationbetweenBMDandhearingloss(26articles).
Records identified through
database searching (n=127)
Medline=41
Embase=42
Lilacs=44
Records after duplicates removed
(n=83)
Records screened (n=83)
Full-text articles assessed for eligibility
Studies included in
qualitative synthesis
Records excluded
(n=67)
Full-text articles excluded,
with reasons
(n=9)
Data not available (n=2)
Non-observational study
(n=1)
No association assessment
(n=2)
No outcome (n=2)
Letter (n=2) Studies included in
quantitative synthesis (meta-analysis)
Osteoporosisandhearingloss 649 Study name Clark, 1995 Helzner, 2005 Helzner, 2005 Helzner, 2005 Helzner, 2005 Helzner, 2005 Helzner, 2005 Helzner, 2005 Helzner, 2005 Kahveci, 2014 Mendy, 2014 Yeh, 2015 Total
Femoral neck bone density Femoral neck-black men Femoral neck-black women Femoral neck-white men Femoral neck-white women Total hip-black men Total hip-black women Total hip-white men Total hip-white women Femur or spine Head
Spine, hip, or forearm
1.90 1.37 0.83 0.92 0.92 1.36 0.91 0.86 0.98 4.50 2.08 1.76 1.20 1.37 1.07 0.67 0.77 0.77 1.05 0.73 0.72 0.82 1.82 1.33 1.33 1.01 2.63 1.76 1.03 1.09 1.09 1.76 1.13 1.03 1.17 11.13 3.24 2.33 1.42 0.00 0.01 0.09 0.35 0.34 0.02 0.40 0.10 0.82 0.00 0.00 0.00 0.04 0.1 0.2
More hearing loss in normal BMD
More hearing loss in low BMD/osteoporosis
0.5 1 2 5 10
7.79 8.78 9.24 9.72 9.74 8.73 9.20 9.66 9.72 2.73 6.31 8.38
Subgroup Statistics for each study Odda ratio and 95% CI
Relative weight Odds ratio Lower limit Upper limit p-Value
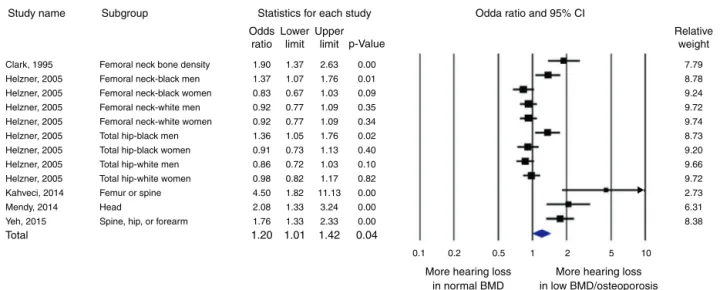
Figure2 Forestplotofstudiescomparingoddsofhearinglossinpatientswhohadlowbonemineraldensityorosteoporosisand control.Adiamonddatamarkerrepresentstheoveralloddsratiosandits95%CI.
A total of 16 articles underwent full-length review. Data wereextractedfromeightstudies involving52,828 partic-ipants who had bone mineral density and hearing status assessed.2,12,13,16---20
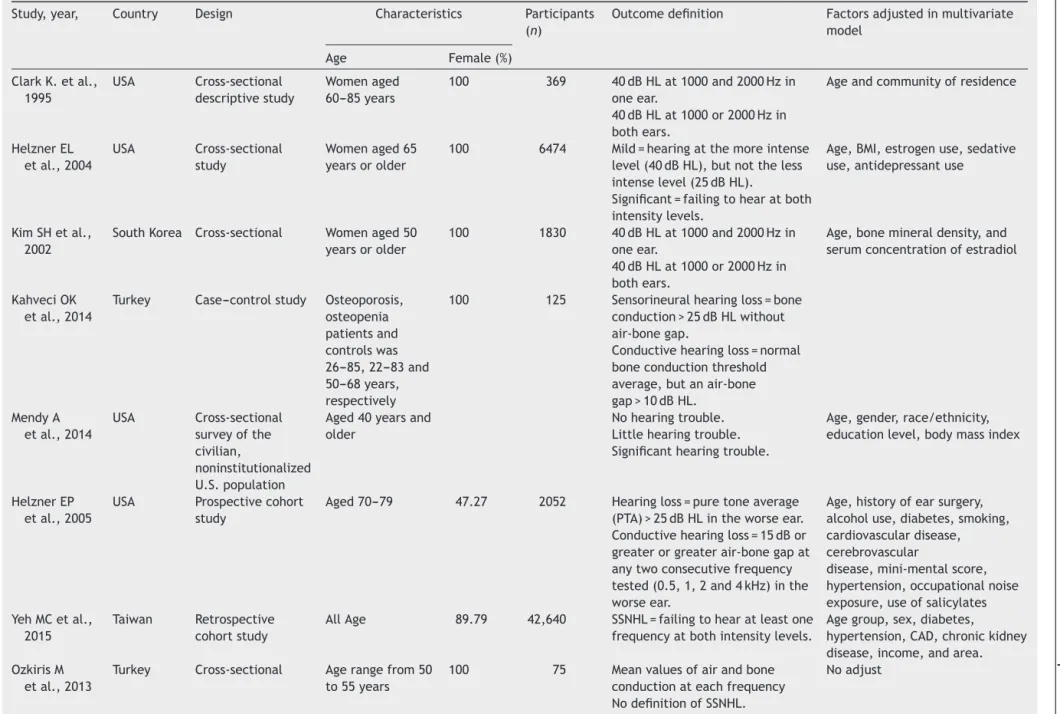
Most of them had cross-sectional design; others were prospectivecohort,retrospectivecohort,andcase---control studies.IncludedstudieswerefromTurkey,USA,andKorea. Theseincludednationalpopulation-basedstudiesfromtwo nations. All participants were assessed by bone mineral densitybystandardizedmethods(dualenergyX-ray absorp-tiometryor DXA).Sites of BMD measurementwere femur, lumbar spine, head, and methods of assessing hearing status included audiometry, otoscopic examination, and self-reported. The characteristics of the eight extracted studiesincludedinthisreviewareoutlinedinTable1.
Qualityassessmentofincludedstudies
The qualityof ninecross-sectional,threecohortand,two case---controlstudieswereevaluatedbyNOS(Table1).Total scorerangedfrom3to8.Twostudieshadlowquality(total score=3)andwereexcludefromthemeta-analysis.
Meta-analysisresults
Fivestudies(2,12,13,16,20)wereincludedinthe meta-analysisofhearingloss.Therewasastatisticallysignificant increased odds of hearing loss in the low BMD or osteo-porosisgroupwithORof 1.20(95%CI1.01---1.42, p=0.04, I2=82%, P
heterogeneity=0.01) (Fig. 2). The study from Clark
etal.,Kahvecietal.,Mendyetal.,andYehetal.allreported significantlyincreasedoddsofhearinglossinthelowBMD groupwithORof1.90(95%CI1.37---2.63,p<0.01),4.50(95% CI1.82---11.13,p<0.01),2.08(95%CI1.33---3.24,p<0.01), and 1.76 (95% CI 1.33---2.33, p<0.01), respectively. How-ever, the study from Helzner et al. reported significantly increasedoddsofhearinglossinthelowBMDgroup,in par-ticulartheareaandpopulationincluded thefemoralneck of black men 1.37 (95% CI 1.07---1.76, p=0.01) and total hipofblackmen1.36(95%CI1.05---1.76,p=0.02).
0.0 0.1 0.2 0.3 0.4 0.5
–2.0 –1.5 –1.0 –0.5 0.0
Log odds ratio
Funnel plot of standard error by log odds ratio
Standard error
0.5 1.0 1.5 2.0
Figure3 Funnelplotassessingpublicationbias.
Sensitivityanalysis
Toassessthestabilityoftheresultsofthemeta-analysis,we conductedasensitivityanalysisbyexcludingonestudyata time.Noneoftheresultswassignificantlyaltered,indicating thatourresultswererobust.
Publicationbias
Toinvestigatepotentialpublicationbias,weexaminedthe contour-enhanced funnel plot of the included studies in assessingchangeinlogORofhearingloss(Fig.3).The ver-ticalaxis representsstudy size(standard error) while the horizontalaxisrepresentseffectsize(logoddsratio).From thisplot,biasisnotpresent becausethereissymmetrical distributionofstudiesonbothsidesofthemean.TheEgger’s test was non-significant (p=0.36). Using the trimand fill methodsintherandom-effectsmodel,therewasno differ-enceoftheimputedOR(1.38)andits95%CI(1.08---1.7).
Discussion
Upala
S
et
al.
Table1 Characteristicsofincludedstudies.
Study,year, Country Design Characteristics Participants
(n)
Outcomedefinition Factorsadjustedinmultivariate
model
Age Female(%)
ClarkK.etal., 1995
USA Cross-sectional
descriptivestudy
Womenaged
60---85years
100 369 40dBHLat1000and2000Hzin
oneear.
40dBHLat1000or2000Hzin bothears.
Ageandcommunityofresidence
HelznerEL etal.,2004
USA Cross-sectional
study
Womenaged65
yearsorolder
100 6474 Mild=hearingatthemoreintense
level(40dBHL),butnottheless intenselevel(25dBHL).
Significant=failingtohearatboth intensitylevels.
Age,BMI,estrogenuse,sedative use,antidepressantuse
KimSHetal., 2002
SouthKorea Cross-sectional Womenaged50
yearsorolder
100 1830 40dBHLat1000and2000Hzin
oneear.
40dBHLat1000or2000Hzin bothears.
Age,bonemineraldensity,and serumconcentrationofestradiol
KahveciOK
etal.,2014
Turkey Case---controlstudy Osteoporosis,
osteopenia patientsand controlswas 26---85,22---83and 50---68years, respectively
100 125 Sensorineuralhearingloss=bone
conduction>25dBHLwithout air-bonegap.
Conductivehearingloss=normal
boneconductionthreshold
average,butanair-bone gap>10dBHL.
MendyA
etal.,2014
USA Cross-sectional
surveyofthe civilian,
noninstitutionalized U.S.population
Aged40yearsand older
Nohearingtrouble. Littlehearingtrouble. Significanthearingtrouble.
Age,gender,race/ethnicity, educationlevel,bodymassindex
HelznerEP etal.,2005
USA Prospectivecohort
study
Aged70---79 47.27 2052 Hearingloss=puretoneaverage
(PTA)>25dBHLintheworseear. Conductivehearingloss=15dBor greaterorgreaterair-bonegapat
anytwoconsecutivefrequency
tested(0.5,1,2and4kHz)inthe worseear.
Age,historyofearsurgery, alcoholuse,diabetes,smoking, cardiovasculardisease, cerebrovascular
disease,mini-mentalscore, hypertension,occupationalnoise exposure,useofsalicylates YehMCetal.,
2015
Taiwan Retrospective
cohortstudy
AllAge 89.79 42,640 SSNHL=failingtohearatleastone
frequencyatbothintensitylevels.
Agegroup,sex,diabetes,
hypertension,CAD,chronickidney disease,income,andarea. OzkirisM
etal.,2013
Turkey Cross-sectional Agerangefrom50
to55years
100 75 Meanvaluesofairandbone
conductionateachfrequency NodefinitionofSSNHL.
Noadjust
Osteoporosisandhearingloss 651
densityandhearingloss.Accordingtoourmeta-analysisof 5studiesfromdifferentcountries,agegroups,gendersand races,wefoundthatadecreaseinBMDorosteoporosiswas significantlyassociatedwithhearingloss.
Age related hearing loss or ‘‘presbycusis’’ is caused by multifactorialetiologies. Arecent study purposed that demineralized petrous temporal bone in addition to age-related bone mass loss could be the cause of developing presbycusis.11,21Interestingly,inPagetdiseaseofthebone, demineralization of the cochlear bone is associated with hearing loss. However, the etiology of the association is unclear.22InconcordancewithdemineralizationinPaget dis-easeofthebone,astudyconductedinotoslcerosispatients byhigh-resolutioncomputedtomographicevaluationofthe cochlear capsule showed decreased BMD at specific loca-tions onthecochlear capsule. Therefore,decreasing BMD physiologicallyassociateswithhearingloss.
The etiology ofPaget diseaseof thebone and otoscle-rosis share similar pathogenesisin the lateral wall of the cochlea,wheretheabnormalboneremodelingmanipulates thechangeinionandfluidhemostasisinperilymphaticspace ofthecochlea.23However,thereareseveralunique charac-teristicsofthepathologicchangeinotosclerosis,including fibrousthickeningandlossofcochlearbloodvessels,spiral ligamenthyalinizationandstriavascularisatrophy.24
Therefore,imbalanceinboneformationandbone resorp-tion from osteoporosis may play an important role in dysfunctional ionic metabolism leading to sensory neural hearingloss.
Normally,BMDsatperipheralsiteshasastrong correla-tionwithmeasurementsathipand spine.The correlation coefficients between peripheral sites and central sites is between 0.6 and 0.70 (25). However, some populations whose peripheral measurements are normal could have osteoporotichiporspine;forexample,thepostmenopausal womanwith significant osteoporoticrisk factors.25 There-fore,differentsitesofBMD measurementfromeachstudy may not accurately reflect total body BMD. With limited resultsfromprevious studies,ourstudy demonstratedthe firstmeta-analysisofcorrelationbetweenhearinglossand BMD.Everystudythatwasincludedinourmeta-analysisdid notreporttotalbodyBMD.Nevertheless,ourmeta-analysis has raised the concern of hearing loss in osteoporosis, sinceourresultisthestrongestevidenceoftheassociation betweenhearinglossandosteoporosiseverreported. There-fore,toevaluatemoreevidenceoftheassociation,further cohortstudies of theassociation between totalbodyBMD andhearinglossshouldbeevaluated.
Thelimitationsofourstudyincludedifferenthearingloss outcomesanddifferentsitesofBMDmeasurementfrom dif-ferentstudies.Hearing lossoutcomesweredeterminedin differentaspectsofmeasurementincludingaudiometryand patientself-evaluation.Variationintheoutcomeofhearing losscouldpotentiallyaltertheresultsandconclusion.Since differentsitesofBMDmeasurementmaynotbeaccurateas totalBMD,theinterpretationofourstudymaybelimited.
Conclusion
Inconclusion,ourstudyproposedthefirstmeta-analysisthat demonstratedaprobable associationbetweenhearingloss
andBMD.Osteoporosiscouldbeariskfactorinhearingloss andmightplayanimportantroleinage-relatedhearingloss.
Ethical
approval
Thisarticledoesnotcontainanystudieswithhuman partic-ipantsoranimalsperformedbyanyoftheauthors.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgment
WethankMatthewRoslundforvalidationofthesearch.
Appendix
1.
Search
strategy
MEDLINE
1)Hearingloss.mp.orexpHearingLoss/ 2)Audiometry.mp.orexpAudiometry/
3)Otoacoustic.mp.[mp=title,abstract,originaltitle,nameof substanceword,subjectheadingword,keywordheading word,protocolsupplementaryconceptword,raredisease supplementaryconceptword,uniqueidentifier].
4)ExpOsteoporosis/orosteoporosis.mp. 5)Osteopenia.mp.
6)ExpBoneDensity/orbonedensity.mp. 7)Bonemass.mp.
8)Boneloss.mp. 9)BMD.mp.
10)Bonemineraldensity.mp. 11)1or2or3
12)4or5or6or7or8or9or10 13)11and12
14)limit13tohumans EMBASE
((’osteoporosis’/expor‘osteoporosis’and[embase]/lim)or (osteopeniaand[embase]/lim)or(’bonedensity’and [embase]/lim)or(’bonemass’and[embase]/lim)or(’bone loss’and[embase]/lim)or(bmdand[embase]/lim))and ((’hearingloss’/expor‘hearingloss’and[embase]/lim)or (’audiometry’/expor‘audiometry’and[embase]/lim))and [humans]/lim)and[embase]/limnot[medline]/lim.
References
1.FederK,MichaudD,Ramage-MorinP,McNameeJ,Beauregard Y.PrevalenceofhearinglossamongCanadiansaged20to79: audiometricresultsfromthe2012/2013CanadianHealth Meas-uresSurvey.HealthRep.2015;26:18---25.
2.Clark K, Sowers MR, Wallace RB, Jannausch ML, Lemke J, AndersonCV.Age-relatedhearinglossandbonemassina pop-ulation ofruralwomen aged60to 85years.Ann Epidemiol. 1995;5:8---14.
4.DaltonDS,CruickshanksKJ,KleinBE,KleinR,WileyTL,Nondahl DM.Theimpactofhearinglossonqualityoflifeinolderadults. Gerontologist.2003;43:661---8.
5.Kramer SE, Kapteyn TS, Kuik DJ, Deeg DJ. The association ofhearingimpairmentandchronicdiseaseswithpsychosocial healthstatusinolderage.JAgingHealth.2002;14:122---37.
6.WoodcockK,PoleJD.HealthprofileofdeafCanadians:analysis oftheCanadaCommunityHealth Survey.CanFamPhysician. 2007;53:2140---1.
7.WoodcockK,PoleJD.Educationalattainment,labourforce sta-tus and injury:a comparisonof Canadianswithand without deafnessandhearingloss.IntJRehabilRes.2008;31:297---304.
8.Hasson D, Theorell T, Westerlund H, Canlon B. Prevalence andcharacteristicsofhearingproblemsinaworkingand non-workingSwedishpopulation.JEpidemiol CommunityHealth. 2010;64:453---60.
9.FerriteS,SantanaV.Jointeffectsofsmoking,noiseexposure andageonhearingloss.OccupMed(Lond).2005;55:48---53.
10.HuangQ,TangJ.Age-relatedhearinglossorpresbycusis.Eur ArchOtorhinolaryngol.2010;267:1179---91.
11.KimJY,LeeSB,LeeCH,KimHM.Hearinglossinpostmenopausal women with low bone mineral density. Auris Nasus Larynx. 2016;43:155---60.
12.Yeh MC, Weng SF, Shen YC, Chou CW, Yang CY, Wang JJ, et al. Increased risk of sudden sensorineural hearing loss inpatientswithosteoporosis:apopulation-based,propensity score-matched,longitudinalfollow-upstudy.JClinEndocrinol Metab.2015;100:2413---9.
13.Kahveci OK, Demirdal US, YucedagF, CerciU. Patients with osteoporosis have higher incidence of sensorineural hearing loss.ClinOtolaryngol.2014;39:145---9.
14.StroupDF,BerlinJA,MortonSC,OlkinI,WilliamsonGD,Rennie D,etal.Meta-analysisofobservationalstudiesinepidemiology: aproposalforreporting.Meta-analysisOfObservationalStudies inEpidemiology(MOOSE)group.JAMA.2000;283:2008---12.
15.StangA.CriticalevaluationoftheNewcastle---Ottawascalefor theassessmentofthequalityofnonrandomizedstudiesin meta-analyses.EurJEpidemiol.2010;25:603---5.
16.Purchase-HelznerEL,CauleyJA,FaulknerKA,PrattS,Zmuda JM,TalbottEO,etal.Hearingsensitivityandtheriskofincident fallsand fractureinolderwomen:thestudyofosteoporotic fractures.AnnEpidemiol.2004;14:311---8.
17.KimSH,KangBM,ChaeHD,KimCH.Theassociationbetween serumestradiollevelandhearingsensitivityinpostmenopausal women.ObstetGynecol.2002;99:726---30.
18.Ozkiris M, Karacavus S, Kapusuz Z, Balbaloglu O, Saydam L. Does bone mineral density have an effect on hearing loss in postmenopausal patients. Ann Otol Rhinol Laryngol. 2013;122:648---52.
19.Helzner EP, CauleyJA, Pratt SR, WisniewskiSR, Talbott EO, ZmudaJM,etal.Hearingsensitivityandbonemineraldensity inolderadults:thehealth,agingandbodycompositionstudy. OsteoporosInt.2005;16:1675---82.
20.MendyA,VieiraER,AlbatinehAN,NnadiAK,LowryD,GasanaJ. Lowbonemineraldensityisassociatedwithbalanceandhearing impairments.AnnEpidemiol.2014;24:58---62.
21.ShinYJ,FraysseB,DeguineO,CognardC,CharletJP,SevelyA. Sensorineuralhearinglossandotosclerosis:aclinicaland radio-logicsurveyof437cases.ActaOtolaryngol.2001;121:200---4.
22.MonsellEM.ThemechanismofhearinglossinPaget’sdiseaseof bone.Laryngoscope.2004;114:598---606.
23.Wangemann P. Supporting sensory transduction: cochlear fluidhomeostasis and theendocochlear potential.J Physiol. 2006;576:11---21.
24.DohertyJK,LinthicumFHJr.Spiralligamentandstriavascularis changesincochlearotosclerosis:effectonhearinglevel.Otol Neurotol.2004;25:457---64.