Influence of the robotic exoskeleton Lokomat on the control of human gait: an electromyographic and kinematic analysis
153
0
0
Texto
Imagem
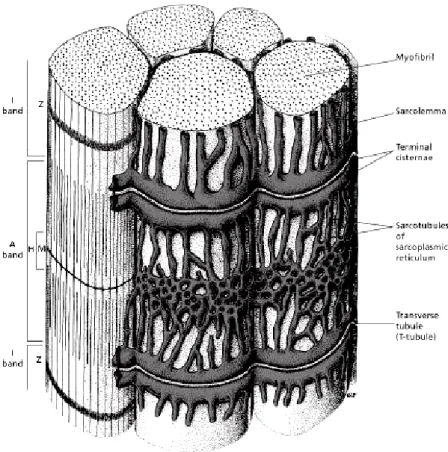
![Figure 3.10: Detailed representation of the organization of the skeletal muscle [84]. Reproduced by permis- permis-sion](https://thumb-eu.123doks.com/thumbv2/123dok_br/17934592.852194/46.892.176.720.133.755/figure-detailed-representation-organization-skeletal-muscle-reproduced-permis.webp)
+7
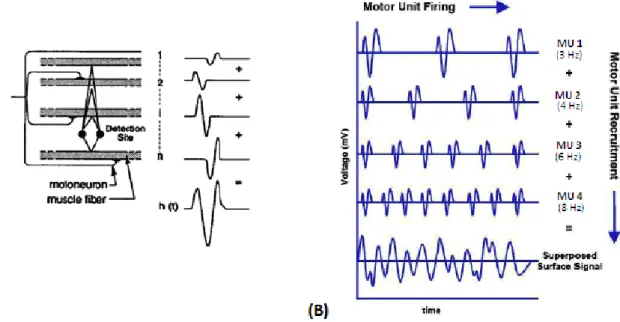
![Figure 4.7: Block diagram of typical sEMG instrumentation. Used with permission from [17]](https://thumb-eu.123doks.com/thumbv2/123dok_br/17934592.852194/56.892.118.763.129.362/figure-block-diagram-typical-semg-instrumentation-used-permission.webp)
Documentos relacionados