REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
REVIEW
ARTICLE
Identification
of
cutoff
points
for
Homeostatic
Model
Assessment
for
Insulin
Resistance
index
in
adolescents:
systematic
review
Maria
Izabel
Siqueira
de
Andrade
∗,
Juliana
Souza
Oliveira,
Vanessa
Sá
Leal,
Niedja
Maria
da
Silva
Lima,
Emília
Chagas
Costa,
Nathalia
Barbosa
de
Aquino,
Pedro
Israel
Cabral
de
Lira
UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
Received1July2015;accepted13August2015 Availableonline28January2016
KEYWORDS Insulinresistance; Adolescent; ROCcurve; Review
Abstract
Objective: ToidentifycutoffpointsoftheHomeostaticModelAssessmentforInsulinResistance (HOMA-IR)indexestablishedforadolescentsanddiscusstheirapplicabilityforthediagnosisof insulinresistanceinBrazilianadolescents.
Datasource: AsystematicreviewwasperformedinthePubMed,LilacsandSciELOdatabases, usingthefollowingdescriptors:‘‘adolescents’’,‘‘insulinresistance’’and‘‘ReceiverOperating CharacteristicsCurve’’.Originalarticlescarriedoutwithadolescentspublishedbetween2005 and2015inPortuguese,EnglishorSpanish languages,whichincludedthestatisticalanalysis usingReceiverOperatingCharacteristicsCurvetodeterminetheindexcutoff(HOMA-IR)were included.
Datasynthesis: Atotalof184articleswereidentifiedandafterthestudyphaseswereapplied, sevenarticleswereselectedforthereview.Allselectedstudiesestablishedtheircutoffsusing aReceiverOperatingCharacteristicsCurve,withthelowestobservedcutoffof1.65forgirlsand 1.95forboysandthehighestof3.82forgirlsand5.22forboys.Ofthestudiesanalyzed,one proposedexternalvalidity,recommendingtheuseoftheHOMA-IRcutoff>2.5forbothgenders.
Conclusions: TheHOMA-IRindexconstitutesareliablemethodforthedetectionofinsulin resis-tanceinadolescents,aslongasitusescutoffsthataremoreadequatefortherealityofthe studypopulation,allowingearlydiagnosisofinsulinresistanceandenablingmultidisciplinary interventionsaimingathealthpromotionofthispopulation.
©2015SociedadedePediatriadeSãoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(https://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](M.I.S.Andrade).
http://dx.doi.org/10.1016/j.rppede.2016.01.004
PALAVRAS-CHAVE Resistênciaàinsulina; Adolescente;
CurvaROC; Revisão
Identificac¸ãodospontosdecortedoíndiceHomeostaticModelAssessmentforInsulin Resistanceemadolescentes:revisãosistemática
Resumo
Objetivo: Identificar ospontosdecortedoíndice HomeostaticModelAssessmentfor Insulin Resistance(HOMA-IR) estabelecidospara adolescentesediscutirasuaaplicabilidadepara o diagnósticodaresistênciaàinsulinaemadolescentesbrasileiros.
Fontesdedados: RevisãosistemáticafeitanasbasesdedadosPubMed,LilacseSciELOcomos descritores‘‘Adolescentes’’,‘‘Resistênciaàinsulina’’e‘‘CurvaROC’’.Foramincluídosartigos originais,publicados entre2005e2015,conduzidoscomadolescentes,noidioma português, inglêsouespanholeincluindoanáliseestatísticacomusodacurvaROCparadeterminac¸ãodos pontosdecortedoíndice(HOMA-IR).
Síntesedosdados: Foramidentificados 184 artigos e, após a aplicac¸ão das etapas do pro-cedimento, foram selecionados sete para compor a revisão. Todosos estudos selecionados estabeleceram seus pontosde corte comacurva ROC. Omenor pontode corte observado foi de1,65parameninase 1,95para meninoseomaiorde 3,82para meninase5,22para meninos.Dosestudosanalisados,umpropôsvalidadeexterna,recomendandoousodoponto decortedoHOMA-IR>2,5paraambosossexos.
Conclusões: OíndiceHOMA-IRconstitui-seemmétodoconfiávelparadetecc¸ãodaresistência insulínicaemadolescentes,desdequeusadosospontosdecortequemaisseadequemà reali-dadedapopulac¸ãoemestudo,oquepermiteumdiagnósticoprecocedaresistênciaàinsulina epossibilitaintervenc¸õesmultiprofissionaisparaapromoc¸ãodasaúdedessapopulac¸ão. ©2015SociedadedePediatriadeSãoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Adolescenceisacriticalperiodfortheonsetofobesityand othermetabolicdisordersassociatedwithbodyfat accumu-lation.Adolescents withexcess weighthave ahigh riskof becomingobeseadultsandarepronetodeveloping cardio-vasculardiseases.1,2
Excessive accumulation of body fat, particularly fat locatedinthecentralorvisceralregion,favorstheincrease in free fatty acids in the bloodstream, which may impair insulinsignaling,decreasingthesensitivityofreceptorson cellmembranesandresultingininsulinresistance(IR).3
Brazilian studieshave detectedthe prevalenceof IRin theagerangeofadolescenceandhavereportedprevalence rates ranging from6.5% to90.8% in adolescents withand withoutexcessweight.3---5Themostcommonlyusedmethods
fordeterminingIRinepidemiological studiesareobtained frompracticalformulasthatusefastingglucoseandinsulin levels, as the Fasting Glucose/Insulin Ratio (FGIR), the Quantitative insulin sensitivity check index (QUICKI) and the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR),whichhasbeenfrequentlyvalidatedinchildren and adolescents and is recommended as the most sensi-tiveandspecificmethodforassessinginsulin sensitivityin thispopulation.6---8 Itisnoteworthythatoneof the
impor-tantaspectstobeobservedinthesuccessfulapplicationof HOMA-IRindexin agivenpopulation istheuse ofspecific cutoffsforgender,ethnicity,ageand/orsexualmaturation level(ifusedinadolescents).Forthisreason,severalcutoff pointshavebeenrecommendedforthediagnosisofIRbased ontheindex.9---12 The objectiveof thisstudy wasto
iden-tifyHOMA-IRindexcutoffsestablishedforadolescentsand
discusstheirapplicabilityforthediagnosisofIRinBrazilian adolescents.
Method
Literaturesearchstrategy
Asystematicliterature reviewof scientificarticlesonthe topic‘‘Insulinresistance inadolescents’’ wascarriedout, takingintoaccountthefollowing guidingquestion: ‘‘what arethecutoffsforHOMA-IRindexestablishedforIR determi-nationinadolescentswithandwithoutmetabolicsyndrome inobservationalstudies?’’.
The definitionof the researchquestion wasstructured according to the acronym PECO, recommended by the Methodological Guidelines for the preparation of system-aticreviewandmeta-analysisofcomparativeobservational studiesonriskfactorsandprognosis,in whicheach letter correspondsto a component of theguiding question: P ---population,E---exposure,C---Control,O---Outcome.13After
determiningthequestion,a searchwascarriedoutinthe PubMed,LilacsandSciELOdatabases.
Tosearchusedthefollowingdescriptors:‘‘adolescent’’, ‘‘Insulinresistance’’and‘‘ROC(ReceiverOperating Charac-teristic)curve’’.Thetermspresentinthemodelwerefound inthelistofMedicalSubjectHeadings(Mesh),availablefrom theUSNationalLibraryofMedicine, andthelistofHealth SciencesDescriptors,availableontheBVSportal.
[MeshTerms] OR(‘‘insulin’’[AllFields]AND ‘‘resistance’’ [AllFields])OR‘‘insulinresistance’’[AllFields])AND(‘‘roc curve’’[MeSHTerms] OR(‘‘roc’’[AllFields]AND‘‘curve’’ [All Fields]) OR ‘‘roc curve’’ [All Fields]). In the Lilacs and SciELO databases, the search was carried out using theexpression:(tw:[adolescentes])AND(tw:[resistênciaà insulina])AND(tw:[curvaroc])AND(instance:regional).
The methodological procedure used to carry out this researchwascompleteandfinalizedonMarch1st,2015.
Studyselection
The articles identified during the database search were selected after the reading of the titles, followed by the abstracts and full texts, when indicated. The procedure wasindependentlycarried outby tworesearchers,taking intoaccountthepredefinedinclusioncriteria:original arti-cle,publishedinthelast10 years(between 2005andthe searchenddate),carriedoutwithAdolescents, writtenin Portuguese,EnglishorSpanish,includingstatisticalanalysis usingReceiverOperatingCharacteristicsCurvetodetermine thecutoffpointsforHOMA-IRindex.
Afterarticleselection,theKappaindexwasapplied14to
analyzethe agreement between the two researchersand anexcellent/almostperfectagreementwasfound(=0.90). In case of disagreement, the studies were discussed in a meetingwiththeauthorsfor evaluationandconsensuson theirinclusioninthisreview.
The entire description procedurefor identification and selection of studies wasbasedon theguideline Preferred ReportingItemsforSystematicReviews(Prisma).15
Analysisofarticlequality
Article qualitywasassessed according tothe initiative of Strengthening the Reporting of Observational Studies in Epidemiology (Strobe), translated into Portuguese.16 The
checklist comprising Strobe includes 22 questions divided intosix groups:TitleandAbstract,Introduction, Methods, Results,DiscussionandOtherInformation.Thus,thearticles includedinthisreviewwerescoredfrom0to22,whichwere later transformed into percentages for better qualitative analysis.
Considering the nature of the initial search for obser-vational studies, of the eligibility criteriato conduct the findingstodirectedarticlesandthesmallnumberof stud-iesinBrazil,itwasdecidedtoincludealleligiblearticles, regardlessoftheachievedscore.
Dataextraction
Dataextraction wasperformed using Microsoft Excel pro-gram, version 2007 using a protocol created by the researchers,inwhichthefollowingdatawereincluded: arti-cletitle,author,placeandyearofpublication,samplesize, characteristics of thestudy population, age range, cutoff basedontheHOMA-IRindex,sensitivityandspecificityofthe cutoffdetermined throughthe HOMA-IRindex,limitations andexternalvalidationoftheselectedstudies.
Results
Initially,atotalof184articleswereidentified.After analyz-ingthetitlesandabstracts,weselected16thatapparently met the inclusioncriteria. Afterreading the full articles, nine were excluded, as they did not meet the eligibility criteria,totalingsevenfullarticlesincludedinthereview. Theflowchartofarticleidentificationandselectionprocess isshowninFig.1.
The data concerning the main characteristics of the studies included in the systematic review are shown in Table 1. The studies were arranged in descen-ding order of the obtained score, according to Strobe criteria. The median score of article quality was 14.3 (interquartile range: 12.7---17.5) points, and among the studiesincluded,six17---22obtainedqualityscorepercentage
>50%.
Sixstudies,18,20---23 werecarriedoutinforeigncountries
between 2005 and 2015 and one19 was performed with
Brazilianadolescentsin2011.Thesmallestsampleconsisted of 57 participants23 and the largest had 3203.22 All
ana-lyzedstudieshadcross-sectionaldesign,three17,20,22ofthem
nestedinacohort.
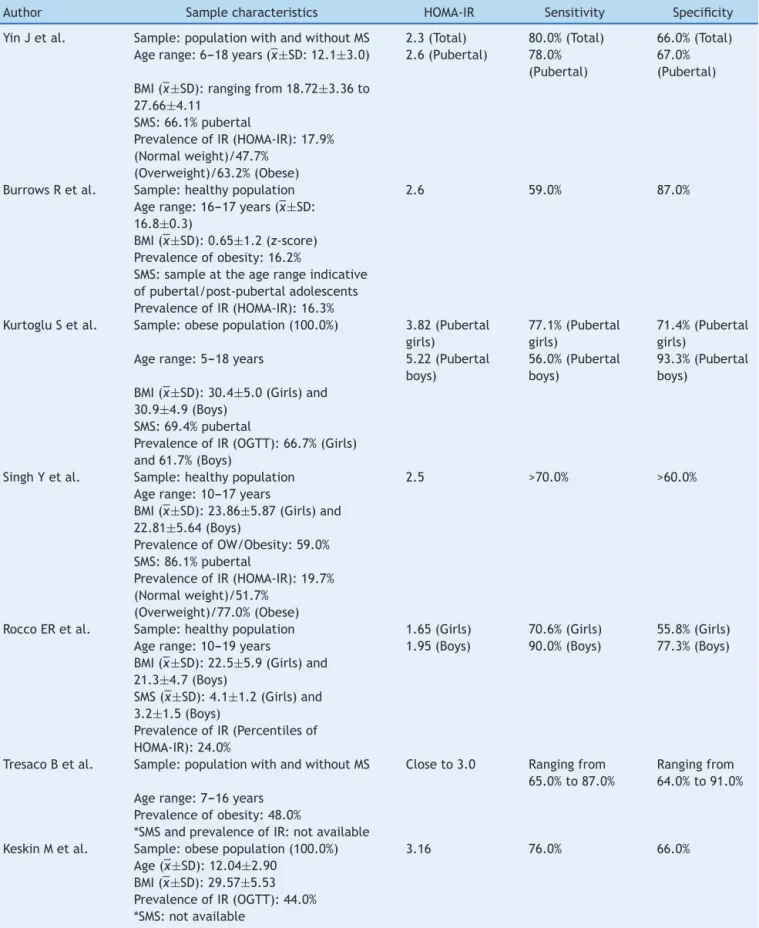
The characteristics of thesamples included in the dif-ferentstudiesandthecutoffsdeterminedfortheHOMA-IR index, withtheirrespective sensitivitiesand specificities, areshowninTable2.
The adolescents included in the selected studies were individualswithmetabolicsyndromeorwithnormalglucose tolerance,withagerangingfrom5to19years.
TheprevalenceofIRvariedfrom16.3%to77%andwas mainlydeterminedbytheoralglucosetolerancetest(OGTT) or thecutoffpointsestablishedfor theHOMA-IRindex.In onestudy,19 IRfrequencywasevaluatedbythepercentile
distribution of the HOMA-IR and was considered IR when greaterthanthe85thpercentile.
Regarding thenutritional status of the studied adoles-cents, most studies18,20,23 consisted of a higherfrequency
of adolescents with overweight/obesity. Two studies18,23
wereexclusivelycarriedoutinsubjectsclassifiedwiththe diagnosisofobesity,accordingtotheusedanthropometric parameters.
Ofthesevenincludedstudies,four18---20,22included
sam-ples withthe highest percentage of pubertal individuals. Two studies21,23 didnotprovide informationregarding the
assessed adolescents’ sexual maturation stage and one study17 used a sample of adolescents representative of
pubertal/post-pubertalindividuals.
Regarding the cutoff points for HOMA-IR index, all selectedstudiesestablishedcutoffsusingtheReceiver Oper-ating Characteristics Curve as a tool. Six studies17,18,20,23
preferredthe useof thecutoffpointwithhigh sensitivity andspecificity andone study19 prioritized thecutoffwith
greatersensitivity.Thelowercutoffpointsfoundwere1.65 for girlsand1.95forboys19 andthehighestwere3.82for
girlsand5.22forboys.18
To determine the cutoff, two studies18,22 took into
accounttheadjustmentaccordingtothesexualmaturation stageandtwo18,19 establishedcutoffsaccordingtogender.
Onestudy18proposedacutoffadjustedforgenderand
184 articles identified in the initial database search
Exclusion of duplicates (n=5)
163 articles excluded
16 full articles for eligibility
assessment 9 articles excluded:
Review article: 1 Another language: 1 Determination of HOMA-IR
cutoff without using the ROC curve: 4
Studies carried out in children or adults and the elderly: 3
7 articles included in the qualitative synthesis
179 articles selected
Identification
Screening
Eligibility
Included
Figure1 FlowchartoftheprocessofidentificationandselectionofarticlesincludedinthesystematicreviewofHOMA-IRindex cutoffpointsinadolescents.
werelowercomparedtothosefoundfor males.Regarding thestudies18,22thatassessedprepubertalandpubertal
indi-viduals separately, data related to the prepubertal ones werenotexposedinthissystematicreview.
Themainlimitationshighlightedintheincludedstudies were:smallsamplesize,studieswithcross-sectionaldesign, nosample sizecalculationandsamplerepresentativeness, inability to extrapolate the results (external validation), nonspecificcutoffpointsforgender andsexualmaturation stageandlackofstandardizationoflaboratorymethodsfor insulinemiadetection(Table3).
Oftheassessedstudies,one20 showedthepossibilityof
resultextrapolation (externalvalidation)toother popula-tions(Table3).
Discussion
Earlyidentificationofcardiovascularriskfactorsin adoles-cents is of great value in preventing chronic diseases in adulthoodandthediagnosisofIR,becauseithasacentral rolein the genesis of metabolic disorders,constitutes an initialtypeofintervention.24,25
The gold standard for the detection of IR is the eug-lycemic clamp, recommended by the guidelines of the AmericanDiabetes Association26; however, this method is
not routinely used, as it is expensive and constitutes an invasiveandcomplexprocedure. The HOMA-IRindex,first describedbyMatthewsetal.27 in 1985,hastheadvantage
ofbeingapractical,fast,inexpensivemethodandonethat
Table1 Characteristics,scoreandqualitypercentageofarticlesselectedforinclusioninthesystematicreview.
Studyauthor,yearandlocation Samplesize Studytype Scorea Percentage(%)
YinJetal.,2013,Beijing/China 3203 Cross-sectional,cohortnested 18.5 84.0 BurrowsRetal.,2015,Santiago/Chile 667 Cross-sectional,cohortnested 17.5 79.5 KurtogluSetal.,2010,Kayseri/Turkey 268 Cross-sectionalinPediatricsarea 16.1 73.2 SinghYetal.,2013,Delhi/India 691 Cross-sectional,cohortnested 14.3 65.0 RoccoERetal.,2011,SãoPaulo/Brazil 319 School-basedcross-sectional 14.0 63.6 TresacoBetal.,2005,Zaragoza/Spain 140 School-basedcross-sectional 12.7 57.7 KeskinMetal.,2005,Kayseri/Turkey 57 Cross-sectionalinPediatricsarea 10.0 45.4
Table2 SamplecharacteristicsandHomeostasisModelAssessment-InsulinResistanceindexcutoffpointsestablishedfor ado-lescentsinstudiesselectedforinclusioninthesystematicreview.
Author Samplecharacteristics HOMA-IR Sensitivity Specificity
YinJetal. Sample:populationwithandwithoutMS 2.3(Total) 80.0%(Total) 66.0%(Total) Agerange:6---18years(¯x±SD:12.1±3.0) 2.6(Pubertal) 78.0%
(Pubertal)
67.0% (Pubertal) BMI(¯x±SD):rangingfrom18.72±3.36to
27.66±4.11 SMS:66.1%pubertal
PrevalenceofIR(HOMA-IR):17.9% (Normalweight)/47.7%
(Overweight)/63.2%(Obese)
BurrowsRetal. Sample:healthypopulation 2.6 59.0% 87.0%
Agerange:16---17years(¯x±SD: 16.8±0.3)
BMI(¯x±SD):0.65±1.2(z-score) Prevalenceofobesity:16.2%
SMS:sampleattheagerangeindicative ofpubertal/post-pubertaladolescents PrevalenceofIR(HOMA-IR):16.3%
KurtogluSetal. Sample:obesepopulation(100.0%) 3.82(Pubertal girls)
77.1%(Pubertal girls)
71.4%(Pubertal girls)
Agerange:5---18years 5.22(Pubertal boys)
56.0%(Pubertal boys)
93.3%(Pubertal boys)
BMI(¯x±SD):30.4±5.0(Girls)and 30.9±4.9(Boys)
SMS:69.4%pubertal
PrevalenceofIR(OGTT):66.7%(Girls) and61.7%(Boys)
SinghYetal. Sample:healthypopulation 2.5 >70.0% >60.0%
Agerange:10---17years
BMI(¯x±SD):23.86±5.87(Girls)and 22.81±5.64(Boys)
PrevalenceofOW/Obesity:59.0% SMS:86.1%pubertal
PrevalenceofIR(HOMA-IR):19.7% (Normalweight)/51.7%
(Overweight)/77.0%(Obese)
RoccoERetal. Sample:healthypopulation 1.65(Girls) 70.6%(Girls) 55.8%(Girls) Agerange:10---19years 1.95(Boys) 90.0%(Boys) 77.3%(Boys) BMI(¯x±SD):22.5±5.9(Girls)and
21.3±4.7(Boys)
SMS(¯x±SD):4.1±1.2(Girls)and 3.2±1.5(Boys)
PrevalenceofIR(Percentilesof HOMA-IR):24.0%
TresacoBetal. Sample:populationwithandwithoutMS Closeto3.0 Rangingfrom 65.0%to87.0%
Rangingfrom 64.0%to91.0% Agerange:7---16years
Prevalenceofobesity:48.0%
*SMSandprevalenceofIR:notavailable
KeskinMetal. Sample:obesepopulation(100.0%) 3.16 76.0% 66.0%
Age(¯x±SD):12.04±2.90 BMI(¯x±SD):29.57±5.53 PrevalenceofIR(OGTT):44.0% *SMS:notavailable
SMS,sexualmaturationstage;OW,overweight;HOMA-IR,HomeostasisModelAssessment-InsulinResistance;IR,insulinresistance;MS,
Table3 Mainmethodologicallimitationsandexternalvalidationofthestudiesselectedforinclusioninthesystematicreview.
Author Mainmethodologicallimitations Externalvalidation
YinJetal. Lackofstandardizationofinsulin detectionmethods,lackofcomparison byeuglycemicclampandcross-sectional study.
StudycarriedoutwithChinese adolescents,itisnotpossibleto extrapolatetheresultstoother ethnicities.
BurrowsRetal. Sampleisnotrepresentative, cross-sectionalstudy.
Thecutoffisapplicableinclinical practice.
KurtogluSetal. Smallsamplesizeinterferedin determiningprecisecutoffpoints,lack ofcomparisonbyeuglycemicclamp, cross-sectionalstudy.
Smallsamplesize,itisnotpossibleto extrapolatetheresults.
SinghYetal. Absenceoflongitudinalmonitoringand comparisonbytheeuglycemicclamp.
Thecutoffpointisapplicablebecauseit wasobtainedfromalargecohortwitha homogeneoussampleofnormaland obeseindividuals.
RoccoERetal. Lackofstandardizationofinsulin detectionmethods,absenceof comparisonbyeuglycemicclampand cross-sectionalstudy.
Theobtaineddatacanbeappliedto detectasetofcardiometabolicchanges.
TresacoBetal. Determinationofasetofapproximated cutoffpointswithoutestablishinga singlecutoff,nocomparisonby euglycemicclamp,cross-sectionalstudy withoutconsideringSMSandgenderto determinethecutoffs.
RestrictedtothePediatricsarea.They shouldnotbeusedwiththegeneral populationinepidemiologicalstudies
KeskinMetal. Cross-sectionalstudy,smallsamplesize, absenceofcomparisonbyeuglycemic clamp,withoutconsideringSMSand gendertodeterminethecutoffs.
Noinformation
SMS,sexualmaturationstage.
hasahighcorrelation withtheeuglycemicclamp(r=0.88; p<0.0001).
InastudycarriedoutbySouzaetal.5withchildrenand
adolescentstreatedonanoutpatientbasis,theuseof HOMA-IR(cutoff>2)wasproposed12fortheearlyidentificationof
thepresenceofIR,asthiscriterionhasbeenabletodetect ahigherpercentageofindividualswithIRwhencompared totheOGTT(90.8%vs.64.1%,respectively).
SomelimitationsregardingtheuseoftheHOMA-IRindex areworthmentioning,amongthemtheuseofparameters obtainedinthefastingstate;theuseofcutoffs,which,even thoughareofhighsensitivityandspecificity,arenotalways devoidoferrorsandcanincludemisdiagnosis;andthe esti-mateofanoverallinsulinsensitivity,whichcanbedifferent intheliverandperipheraltissues.28,29
Nonetheless, the HOMA-IR is well accepted by researchersand used in epidemiological studies to deter-mineinsulinresistancein adults,childrenandadolescents asasimplifiedoption tothemoreexpensive and sophisti-catedIRassessmentmethodologies.6,12,30---34Severalauthors
have proposed cutoffpoints to identify IR in adolescents basedontheHOMA-IRindex9---12andtheReceiverOperating
Characteristics Curve is one of the statistical methods most commonly used for this purpose. This tool is often used in clinical and epidemiological studies that aim to determine cutoffs for diagnosticmethods. This procedure takesintoaccountthesensitivityandspecificityofthetest
beingassessed, which are related tothe probabilitythat the test will correctly distribute the studied population in not healthy/ill patients (positive) and healthy/not ill (negative) respectively.29,35 In the present review, it was
observedthatsix17,18,20---23oftheincluded studiespreferto
usethecutoffpointswithhighersensitivityandspecificity. OnlytheBrazilianstudy19 assumed thecutoffwithgreater
sensitivity.
AccordingtoCarrazzoneetal.,36screeningtestsrequire
highsensitivityandmoderatespecificity.Ontheotherhand, diagnostictestsrequirehigherspecificities.Thisallowsonly the actually ill individuals to be classified as having that condition. Basedon thisfact, it can be inferredthat the cutoff with higher sensitivity, proposed in the study by Rocco et al.,19 can be indicated for early IR assessment
asascreening methodfor adolescents withhigherrisk of developingcardiometaboliccomplications.
In studies in which the cutoffs were adjusted for gender,18,19 female adolescents had lower values for the
HOMA-IRindexcutoff, anevent probablyobserveddue to highermeansofHOMA-IRindexandhigherfrequenciesofIR infemales.
Infact,studies4,37 show thatduringadolescence,there
withsignificantlyhigherHOMA-IRindexmeans. Therefore, thepopulationofadolescentsshouldbestudiedasa func-tionofgenderandsexualmaturationstage.Intheassessed studies, the analysisof sexualmaturation was performed usingtheclassificationcriteriaproposedbyTanner,38which
considerindividualsat ≥stageIIfor thesexualmaturation stageaspubertal.
Ofthe included investigations,only thestudy by Singh etal.20 with Indian adolescentsshowed the possibility to
extrapolatetheresultstoother populations.However,the authorsdidnottake intoaccountthegenderandstageof sexualmaturationin theiranalyses.Additionally,itshould benotedthatinordertousethecutoffestablishedinthis studyinBrazilianadolescents,oneshouldtakeintoaccount thedifferencesintheprevalenceofexcessweightand obe-sityamongBrazilianandIndianadolescents.Thepercentage ofthisnutritionaldiagnosisisloweramongBrazilians(25.4% amongBrazilian39vs.59.0%inIndianadolescents).However,
thecutoffdeterminedbythestudyhasgoodsensitivityand specificityandthevaluecanbeusefulintheearlydetection ofIR.
Inthe studycarriedout byBurrowsetal.17 withSouth
AmericanadolescentslivinginChile,thecutoffdetermined forHOMA-IRindexwasclosetothatrecommendedbythe previouslycited study20 andan important association was
foundbetweenHOMA-IR≥2.6andhighcardiometabolicrisk. It is suggested that the findings of Burrows et al.17
cor-roboratetheexternal validityofthe cutoffrecommended bySingh etal.,20 considering howclose thecutoff values
determinedinbothstudieswere.
TheIGuidelinesofPreventionofAtherosclerosisin Child-hood and Adolescence40 indicates the use of the cutoff
proposed by Keskin et al.23 to determine IR in Brazilian
adolescents.Astherearenostudiesonthesubjectwith rep-resentativesamplesofBrazilianadolescents,severalstudies carriedoutinthecountryusetherecommendationproposed bytheguideline40forIRdiagnosis.4,41---44However,itisworth
mentioning that after the publication of the guideline,40
otherinvestigationswerecarriedoutusingmorecontrolled methodologicalprocedureswithlargersamplesizes,which weremoresimilartothepopulationofBrazilianadolescents andofwhichproposedcutoffsweremoreconsistentwiththe physiologyoftheseindividuals.17,20
ThecutoffproposedbythestudyofRoccoetal.19 isan
optionforthedetectionofIRamongadolescents;however, asitwascreatedfortheanalysisofasetofcardiometabolic alterations,it is recommendedthatthe cutoffbeusedin clinicalpracticetoscreen at-riskadolescents.Thecutoffs proposedbythestudiesofYinetal.,22Kurtogluetal.18and
Tresacoetal.21aregearedtowardthepopulationsanalyzed
inthebaselinestudiesandmaynotbeconsistentwiththe presenceofIRinBrazilianadolescents.
Some limitations related to the design of the primary studieswererecorded,suchasthecross-sectionaldesign, whichpreventsinferringcauseandeffectassociations;the absence of the euglycemic clamp for comparison of this method with the HOMA-IR index; however, as mentioned before,theeuglycemicclampisnotfrequentlyperformedin clinicalandepidemiologicalstudiesconsideringitshighcost; andthe lack ofstandardization in laboratory methods for insulinemiadetection,whichmakesitdifficulttocompare theoriginalstudies.Additionally,anotherlimitingfactorwas
theinclusionofchildrenandadolescentsinthedesignofthe originalassessedstudies,withoutproperadjustmentforthe sexualmaturation stagewhendetermining thecutoffsfor theHOMA-IRindex.21,23
Regarding the interpretation of results in the present study,onemustconsidertheprobabilitythatsomearticles werenotfound duringthe literaturesearch,although the researchstrategy tookinto accountthe possibilityof this biasinallstages, andtheabsenceofquantitativeanalysis andthecalculation ofsummarymeasures(meta-analysis), due totheheterogeneity ofthe assessedstudies interms ofsampling,useofclassificationcriteriaanddifferentiated statisticalanalyses,aswellasbiologicalandsocialvariations betweenthepopulationsofthebaselinestudies.
Inbrief,theHOMA-IRindexconstitutesareliablemethod fordetectionofIRinadolescents,aslongasitusescutoff pointsthatarebestsuitedtotherealityofthepopulation beingassessed. Itcan beobserved thatthe literaturedid not show any representative studies carried out in Brazil thataimedtodeterminecutoffsfor IRdetectionusingthe HOMA-IRindexinadolescentsinthecountry.Therefore,it isnecessary tocarryoutnationalstudieswith representa-tivesamplesthatcanmorereliablyidentifyHOMA-IRindex cutoffpointsforBrazilianadolescents.
Itisexpectedthattheresultsofthissystematicreview contribute toencourage thestandardization of IR classifi-cation methodsthroughthe HOMA-IRindexinadolescents andassistintheearlydetectionofIRandcardiometabolic diseasepreventioninadulthood.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.CostaRF,SantosNS,GoldraichNP,BarskiTF,AndradeKS,Kruel LF.Síndromemetabólicaemadolescentesobesos:comparac¸ão entretrêsdiferentescritériosdiagnósticos.JPediatr(RioJ). 2012;88:303---9.
2.LavradorMS,AbbesPT,EscrivãoMA,TaddeiJA.Riscos cardio-vascularesemadolescentescomdiferentesgrausdeobesidade. ArqBrasCardiol.2011;96:205---11.
3.SigwaltFR,SilvaRC.Resistênciaàinsulinaemadolescentescom esemexcessodepesodemunicípiodaGrandeFlorianópolis ---SC.RevBrasEnferm.2014;67:43---7.
4.GobatoAO,VasquesAC,ZambonMP,BarrosFilhoAA,HesselG. Síndromemetabólicaeresistênciaàinsulinaemadolescentes obesos.RevPaulPediatr.2014;32:55---9.
5.SouzaMR,BezerraCS,MazzarioRA,LeiteBP,LiberatoreJunior RD.Análisedaprevalênciaderesistênciainsulínicaediabetes mellitustipo2em crianc¸aseadolescentesobesos.ArqCienc Saude.2004;11:215---8.
7.MieldazisSF,AzzalisLA,JunqueiraVB,SouzaFI,SarniRO, Fon-secaFL.Avaliac¸ãodohiperinsulinismoemamostradecrianc¸as pré-puberes.JPediatr(RioJ).2010;86:245---9.
8.UwaifoGI,FallonEM,ChinJ, ElbergJ,ParikhSJ,FallonEM. Indicesofinsulinaction,disposal,andsecretionderivedfrom fastingsamplesandclampsinnormalglucose-tolerantblackand whitechildren.DiabetesCare.2002;25:2081---7.
9.CuarteroBG, Lacalle CG,Lobo CJ, Vergaz AG, Rey CC, Vil-larMJ,et al.Índice HOMAyQUICKI, insulinaypéptidoC in ni˜nossanos:puntodecortederiesgocardiovascular.AnPediatr (Barc).2007;66:481---90.
10.Invitti C, Guzzaloni G, Gilardini L, Morabito F, Viberti G. Prevalence and concomitants of glucose intolerance in European obese children and adolescents. Diabetes Care. 2003;26:118---24.
11.Lee JM, Okumura MJ, Davis MM, Herman WH, Gurney JG. Prevalence and determinants of insulin resistance among U.S. adolescents. A population-based study. Diabetes Care. 2006;29:2427---31.
12.SchwimmerJB,Deutsch R, RauchJB,BehlingC,NewburyR, LavineJE.Obesity,insulinresistance,andother clinicopatho-logicalcorrelatesofpediatricnonalcoholicfattyliverdisease. JPediatr.2003;143:500---5.
13.Brasil---MinistériodaSaúde.SecretariadeCiência,Tecnologia eInsumosEstratégicos---Departamentodeciênciaetecnologia. DepartamentodeCiênciaeTecnologia.Diretrizes metodológi-cas:elaborac¸ãoderevisãosistemáticaemetanálisedeestudos observacionaiscomparativossobrefatoresderiscoe prognós-tico.Brasília:MinistériodeSaúde;2014.
14.LandisJR,KochGG.Themeasurementofobserveragreement forcategoricaldata.Biometrics.1997;33:159---74.
15.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statementfor reporting sys-tematicreviews and meta-analyses of studiesthat evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
16.Malta M, Cardoso LO, Bastos FI, Magnanini MM, Silva CM. Iniciativa STROBE: subsídiospara a comunicac¸ão de estudos observacionais.RevSaudePublica.2010;44:559---65.
17.Burrows R, Correa-Burrows P, Reyes M, Blanco E, Albala C, Gahagan S. Healthy Chilean adolescents with HOMA-IR ≥2.6 have increased cardiometabolic risk: association with genetic,biological,andenvironmentalfactors.JDiabetesRes. 2015:783296.
18.Kurto˘gluS,Hatipo˘gluN,Mazco˘gluM,KendiriciM,KeskinM, Kon-dolotM.Insulinresistanceinobesechildrenandadolescents: HOMA-IRcut-offlevelsintheprepubertalandpubertalperiods. JClinResPediatrEndocrinol.2010;2:100---6.
19.Rocco ER, Mory DB, Bergamin CS, Valente F, Miranda VL, Calegare BF. Optimal cutoff points for body mass index, waist circumference and HOMA-IR to identify a cluster of cardiometabolic abnormalities in normal glucose-tolerant Brazilianchildrenandadolescents.ArqBrasEndocrinolMetab. 2011;55:638---45.
20.SinghY,GargMK,TandonN,MarwahaRK.Astudyofinsulin resis-tancebyHOMA-IRanditscut-offvaluetoidentifymetabolic syndrome in urban Indian adolescentes. J Clin Res Pediatr Endocrinol.2013;5:245---51.
21.TresacoB,BuenoG,PinedaI,MorenoLA,GaragorriJM,BuenoM. Homeostaticmodelassessment(HOMA)indexcut-offvaluesto identifythemetabolicsyndromeinchildren.JPhysiolBiochem. 2005;61:381---8.
22.YinJ,LiM,XuL,WangY,ChengH,ZhaoX,etal.Insulin resis-tancedetermined byhomeostasis model assessment(HOMA) andassociationswithmetabolicsyndromeamongChinese chil-drenandteenagers.DiabetolMetabSyndr.2013;5:71---9.
23.Keskin M, Kurtoglu S, Kendirci M, Atabek ME, Yazici C. Homeostasismodel assessment is more reliablethan fasting
glucose/insulinratioandquantitativeinsulinsensitivitycheck indexforassessinginsulinresistanceamongobesechildrenand adolescents.Pediatrics.2005;115:e500---3.
24.CruzML, GoranMI. Themetabolic syndromein childrenand adolescents.CurrDiabRep.2004;4:53---62.
25.MoraesAC,FulazCS,Netto-OliveiraER,ReichertFF.Prevalência de síndrome metabólica em adolescentes: uma revisão sis-temática.CadSaudePublica.2009;25:1195---202.
26.American Diabetes Association. Conference development on insulinresistance.DiabetesCare.1998;21:310---4.
27.Matthews D,Hosker JP, Rudenski AS,Naylor BA, Trecher DF, Turner RC. Homeostasismodelassessment: insulinresistance andbeta-cellfunctionfromfastingplasmaglucoseandinsulin concentrationinman.Diabetologia.1985;28:412---9.
28.GelonezeB, TambasciaMA.Avaliac¸ão laboratoriale diagnós-tico da resistência à insulina. Arq Bras Endocrinol Metab. 2006;50:208---15.
29.Martinez EZ, Louzada-Neto F,Pereira BB. A curva ROC para testesdiagnósticos.CadSaudeColetiva.2003;1:7---31.
30.Geloneze B, Vasques AC, Stabe CF, Pareja JC, Rosado LE, Queiroz EC,et al. HOMA1-IR and HOMA2-IR indexes in iden-tifying insulin resistance and metabolic syndrome: Brazilian Metabolic Syndrome Study (BRAMS). Arq Bras Endocrinol Metabol.2009;53:281---7.
31.Madeira IR, Carvalho CN, Gazolla FM, Matos HJ, Borges MA, Bordallo MA. Ponto de corte do índice homeostatic model assessment for insulin resistance (HOMA-IR) avali-ado pela curva receiver operating characteristic (ROC) na detecc¸ão de síndrome metabólica em crianc¸as pré-púberes com excesso de peso. Arq Bras Endocrinol Metab. 2008;52: 1466---73.
32.MuniyappaR,LeeS,ChenH,QuonMJ.Currentapproachesfor assessinginsulinsensitivityandresistanceinvivo:advantages, limitations, and appropriate usage. Am J Physiol Endocrinol Metabol.2008;294:E15---26.
33.ReinehrT, AndlerW. Changesin the atherogenic risk factor profile according to degree of weight loss. Arch Dis Child. 2004;89:419---22.
34.SouzaMS,LemeRB,FrancoRR,RomaldiniCC,TumasR,Cardoso AL,etal.Síndromemetabólicaemadolescentescomsobrepeso eobesidade.RevPaulPediatr.2007;25:214---20.
35.CastanhoMJ,BarrosLC,VenditeLL,YamakamiA.Avaliac¸ãode umtesteemmedicinausandoumacurvaROCfuzzy. Biomatem-atica.2004;14:19---28.
36.CarrazzoneCF,BritoAM,GomesYM.Importânciadaavaliac¸ão sorológicapré-transfusionalemreceptoresdesangue.RevBras HematolHemoter.2004;26:93---8.
37.Faria ER, Faria FR, Franceschini SC, Peluzio MC, Sant’Ana LF, Novaes JF, et al. Resistência à insulina e compo-nentes da síndrome metabólica, análise por sexo e por fase da adolescência. Arq Bras Endocrinol Metab. 2014;58: 610---8.
38.TannerJM.Growthatadolescence.In:MalinaRM,BouchardC, editors.Growth,maturation,andphysicalactivity.Champaign: HumanKineticsBooks;1991.
39.Brasil---InstitutoBrasileirodeGeografiaeEstatística.Pesquisa de orc¸amentos familiares 2008---2009. Rio de Janeiro: IBGE; 2011.
40.Sociedade Brasileira de Cardiologia; departamento de aterosclerose. I Diretriz de Prevenc¸ão da Aterosclerose na Infância ena Adolescência.Arq BrasCardiol. 2005;85 Suppl 6:3---36.
41.Faria ER, Franceschini SC, Peluzio MC, Sant’Ana LF, Pri-oreSE.Correlac¸ãoentrevariáveis decomposic¸ão corporale metabólicaemadolescentesdosexofeminino.ArqBrasCardiol. 2009;93:119---27.
sexofemininodeescolaspúblicasdoDistritoFederal(Brasil). ALAN.2011;61:5---64.
43.SantosLC,CintraIP,FisbergM,MartiniLA.Bodytrunkfatand insulinresistanceinpost-pubertalobeseadolescents.SaoPaulo MedJ.2008;126:82---6.