REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
Factors
associated
with
low
levels
of
aerobic
fitness
among
adolescents
Eliane
Cristina
de
Andrade
Gonc
¸alves,
Diego
Augusto
Santos
Silva
∗ProgramadePós-Graduac¸ãoemEducac¸ãoFísica,UniversidadeFederaldeSantaCatarina(UFSC),Florianópolis,SC,Brazil
Received24March2015;accepted22June2015 Availableonline5March2016
KEYWORDS
Association;
Oxygenconsumption; Lifestyle;
Exercise;
Adolescenthealth
Abstract
Objective: Toevaluatetheprevalenceoflowaerobicfitnesslevelsandtoanalyzethe associ-ationwithsociodemographicfactors,lifestyleandexcessbodyfatnessamongadolescentsof southernBrazil.
Methods: Thestudyincluded879adolescentsaged14---19yearsthecityofSãoJosé/SC,Brazil. TheaerobicfitnesswasassessedbyCanadianmodifiedtestofaerobicfitness.Sociodemographic variables(skincolor,age,sex,studyturn,economiclevel),sexualmaturationandlifestyle (eat-inghabits,screentime,physicalactivity,consumptionofalcoholandtobacco)wereassessed byaself-administeredquestionnaire.Excessbodyfatnesswasevaluatedbysumofskinfolds tricepsandsubscapular.Weusedlogisticregressiontoestimateoddsratiosand95%confidence intervals.
Results: Prevalenceoflowaerobicfitnesslevelwas87.5%.Thegirlswhospenttwohoursor moreinfrontscreen,consumedlessthanoneglassofmilkbyday,didnotsmokeandhadan excessofbodyfatnesshadahigherchanceofhavinglowerlevelsofaerobicfitness.Whiteboys withlowphysicalactivityhadhadahigherchanceofhavinglowerlevelsofaerobicfitness.
Conclusions: Eight out of ten adolescents were with low fitness levels aerobic. Modifiable lifestylefactorswereassociatedwithlowlevelsofaerobicfitness.Interventionsthatemphasize behaviorchangeareneeded.
©2015SociedadedePediatriadeSãoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(https://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Associac¸ão;
Consumodeoxigênio; Estilodevida; Exercício;
Saúdedoadolescente
Prevalênciaefatoresassociadosabaixosníveisdeaptidãoaeróbiaemadolescentes
Resumo
Objetivo: Avaliaraprevalênciadebaixosníveisdeaptidãoaeróbiaeanalisarsuaassociac¸ão comfatoressociodemográficos,estilodevidaeexcessodeadiposidadecorporalem adoles-centesdeumacidadedosuldoBrasil.
∗Correspondingauthor.
E-mail:[email protected](D.A.S.Silva).
http://dx.doi.org/10.1016/j.rppede.2015.06.025
Métodos: Estudo com879adolescentesde 14a19 anosde SãoJosé,SC, Brasil.A aptidão aeróbiafoiavaliadapelotestecanadensemodificadodeaptidãoaeróbia.Variáveis sociode-mográficas(cordapele,idade,sexo,turnodeestudo,níveleconômico),maturac¸ãosexuale estilodevida(hábitosalimentares,tempodetela,níveldeatividadefísica,consumodeálcool edetabaco)foramavaliadosporquestionárioautoadministrado.Oexcessodeadiposidade cor-poralfoiavaliadopelosomatóriodasdobrascutâneasdotrícepsesubescapular.Empregou-se aregressãologísticaparaaestimativadeoddsratioeintervalosdeconfianc¸ade95%.
Resultados: Aprevalênciadebaixoníveldeaptidãoaeróbiafoide87,5%.Asgarotasque gas-tavamduashorasoumaisemfrente àtela,queconsumiam menosdeum copodeleite ao dia,asnãofumantesecomexcessodeadiposidadecorporalapresentarammaischancesdeter baixosníveis deaptidãoaeróbia.Osgarotosdecordepelebrancaequeerampoucoativos fisicamenteapresentarammaischancesdeterbaixoníveldeaptidãoaeróbia.
Conclusões: Oitoem cadadez adolescentesestavam combaixosníveis deaptidão aeróbia. Fatoresmodificáveisdoestilodevidaforamassociadoscombaixosníveisdeaptidãoaeróbia. Intervenc¸õesqueenfatizemamudanc¸adecomportamentosãonecessárias.
©2015SociedadedePediatriadeSãoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Seculartrendstudieshave shownthat theaerobic perfor-mance of young individuals is decreasing.1 The decrease hasreached 0.36% a year,1 witha prevalence of low aer-obic performance in approximately 80% among Brazilian adolescents.2
Thehighprevalenceofinadequatelevelsofaerobic fit-ness in adolescents increases morbidity and mortality in adulthood,duetooverweight,3metabolicriskfactors3and cognitivediseases,4inadditiontocausingdifficultiesin per-formingeveryday activities.5 Conversely,themaintenance ofadequatecardiopulmonaryindexes, initself,iscapable ofreducinghealth hazardsandhelping therecoveryafter intensephysicalexertion.3
The decline in aerobic fitness is associated with some individualcharacteristics,suchassociodemographicandlife stylefactors.6Asystematicreviewidentifiedthefollowing factorsassociatedwithlowlevelsofaerobicfitness:female gender, low economic level, lower consumption of dairy products and cereals, higher consumption of sweetened beverages, insufficient physical activity, excessive screen timeandexcessof bodyfat.6 However,it is controversial theassociation between low levelsof aerobic fitnessand othersociodemographicfactors,suchasskincolorandage. Moreover, the association between aerobic fitness levels andexcessivealcohol andtobaccoconsumptionisscarcely studied.6
Toassesstheprevalenceoflowlevelsofaerobicfitness andpossiblerelatedfactors,suchassociodemographicand lifestyle indicators is justifiedbecause: (a) it contributes to the epidemiological knowledge of the subject; (b) it allows identifying whether the proportion of adolescents withinsufficientlevelsofaerobicfitnessisthesamein dif-ferent places; (c) it will allow effective interventions to becarriedoutat communityandschool levelonthe out-come.Therefore,theaimofthisstudywastoevaluatethe prevalenceof lowlevelsof aerobicfitnessand toanalyze
theassociationwithsociodemographicfactors,lifestyleand excessbodyfatinhighschooladolescentslivinginacityin southernBrazil.
Method
Thiscross-sectionalanalyticalschool-basedstudyispartof the‘‘BrazilianGuideofPhysicalFitnessEvaluationRelated to Health and Life Habits --- Stage I’’macroproject (Guia Brasileiro de Avaliac¸ão da Aptidão Física Relacionada à SaúdeeHábitosdeVida---EtapaI).Itwasapprovedbythe InstitutionalReviewBoardofUniversidadeFederaldeSanta CatarinaunderprotocolCAAE:33210414.3.0000.0121,and wascarriedoutbetweenAugustandNovember2014.
Thepopulation(n=5182)consistedofschoolchildrenaged 14---19 years enrolledin public schools of SãoJosé, Santa Catarina(SC), Brazil,whichhas209,804inhabitants anda municipal Human Development Index of 0.809.7 São José shares borders with the state capital city of Florianópo-lis, and together they form the most densely populated metropolitanareaofthestateofSC.Inadditiontothefact thattheschoolenvironmentisafavorableplaceto encour-agetheimplementationofahealthyandactivelifestyle,as itistheplacewhereyoungindividualsspendmuchoftheir time,thechoiceofstudentsfrompublicinstitutionsis justi-fiedbecausetheschoolsandneighborhoodswheretheyare located showsocial,cultural andeconomic discrepancies, whichallowsidentifyingadolescentswithdifferentcultures, ethnicitiesandlifestyles.
The samplingprocess wasdeterminedin twostages: 1 --- stratified by state public high schools (n=11); 2 --- class clustersconsideringtheschoolshiftandschoolyear(n=170 classes). In Stage 2, all high school students who were present in classroom onthe days of data collectionwere invitedtoparticipateinthestudy.
of fivepercentagepoints,95% confidenceinterval,design effectof 1.5;20% wereaddedfor lossesand refusalsand an extra20% for the association study.Thus, asample of 751adolescentswasestimated.However,duetothecluster sampling,allstudentsfromallclasseswereinvitedto par-ticipateinthestudy,whichresultedin1148studentswhose data were collected;16 were excluded from the analysis becausetheywereolder than19yearsandthus,thefinal sampleconsistedof1132individuals.
The student eligible for the study was defined as: studentsenrolledinstateschools,beingpresentinthe class-roomonthedatacollectiondayandbeing14---19years.We consideredarefusalwhentheadolescentdeclinedto par-ticipateand,assampleloss,thestudentswhoreturnedan incompletequestionnaire or didnotundergoone or more physicaltests.
Aerobicfitnesswasmeasured usingthemodified Cana-dianAerobicFitnessTest(mCAFT),8validatedincomparison withindirectcalorimetryinCanadianmenandwomenaged 15---69years.9Theadolescentshadtocompleteoneormore stages lasting three minutes each (go up and down two steps measuring20.3cmeach) at pre-determinedrhythms accordingtothegenderandage.Thetestwasterminated onlywhenthe participantreached 85%of maximumheart rate (recommended by the formula220-age),8 which was measuredusingaPolar®H7Bluetoothfrequencymeter.For adolescentswhocompletedatleastonestage,butstopped inthemiddleoftheother,thepreviousstagewasrecorded asthefinalstage.
Oxygen consumptionand thereferencevaluesof aero-bicfitnessweredeterminedusingtheCanadiantests.8The aerobicfitnessscoreequationis:
Scores=10[17.2+(1.29×oxygenconsumption)
−(0.09×weightinkg)−(0.18×ageinyears)]
Basedonthisscore,eachparticipantwasclassifiedinto oneof thefollowing fivecategories: (a)‘‘Needs Improve-ment’’; (b) ‘‘Fair’’; (c) ‘‘Good’’; (d) ‘‘Very good’’; (e) ‘‘Excellent’’.Inthis study,aerobicfitnesswasconsidered ‘‘normal/high’’ for adolescents in categories (c), (d), (e) and‘‘low’’incategories(a)and(b),astheaimofthisstudy wastoidentifythesubgroupsthatweremorelikelytoshow lowlevelsofaerobicfitness,whichresultinseveral prob-lemsfortheadolescents’healthandallowthedevelopment ofdifferentdiseasesinadulthood.1,3,4
The sociodemographic andlifestylevariables were col-lected through a self-administered questionnaire. The questions about eatinghabits, physical activity,excessive consumption of alcohol andtobaccowere takenfrom the Youth Risk Behavior Survey questionnaire, translated and validatedforBrazil.10
Skin color wasself-reported according tothe Brazilian Institute of Geography and Statistics11 and dichotomized into‘‘White’’and‘‘Mixed-race/Black/Yellow/Native Brazil-ian’’.Age wascategorizedas‘‘14---16years’’and‘‘17---19 years’’.The economic level wasidentified by Abep12 and dichotomizedinto‘‘high’’(‘‘A1’’;‘‘A2’’;‘‘B1’’;‘‘B2’’)and ‘‘Low’’(‘‘C1’’;‘‘C2’’;‘‘D’’;‘‘E’’).Theschoolshiftwas cat-egorizedas‘‘day shift’’(morning,afternoon or full-time) and‘‘nightshift’’(nighttime).
Analysisofthescreentimewascarriedoutbyapplying sixdifferentquestions,whichcheckedtheamountofhours spent watching television, using the computer and video game,weeklyandonweekends.Thescreen timewas cal-culated by thesum of hours of screen time onweekdays (calculatedby multiplyingthe hoursand minutes by five) andweekend(calculatedbymultiplyingthehoursand min-utesbytwo),whichresultedinthetotalscreentime.The dailymeanhourswasverifiedbythe sumofhoursonthe sevendaysof the week,divided by thedaysof the week (sevendays)forthethreetypesofelectronicdevices (tele-vision, computer and video games). The categories were ‘‘appropriate’’ (<2h per day) and ‘‘inappropriate’’ (≥2h daily).13
Eatinghabitswereanalyzed bytwodifferentquestions abouthowmanytimestheadolescentconsumedsoftdrinks and milk during the last seven days prior to the survey. Thecategorieswere:‘‘Adequate’’(adolescentwhodidnot consumesoftdrinks);‘‘Inadequate’’(adolescentthat con-sumedsoft drinks)14 and‘‘Adequate’’(consumed≥1glass ofmilk/day);‘‘Inadequate’’(Consumed<1glass/day).15We decidedto analyze these two indicators because a study identifiedareductioninmilkconsumptionandanincrease in softdrink consumption in Brazil.15 This situationhas a negative impact on the health of young individuals, and causes,for instance, bone density impairmentdue tothe lowconsumptionofmilk,whichcandecreaseperformance inphysical activityandtheincreaseinoverweight/obesity duetoconsumptionofsoftdrinks.15
Thequestionregardingphysicalactivitywas:‘‘Duringthe pastsevendays,howmanydayswereyouphysicallyactive foratleast 60minaday?’’The adolescentswhopracticed physicalactivityfiveormoredays/weekwereclassifiedas ‘‘physicallyactive (≥300min a week)’’ and less than five days/weekas‘‘insufficientlyphysicallyactive(<300minper week)’’.16,17
Thequestionsaboutsmokingandexcessivealcohol con-sumptionwerebasedonthenumberofdays(30daysprior tothestudy)inwhichtheadolescentsmokedandconsumed fiveormorealcoholicdrinksonasingleoccasion.The cat-egorieswere:‘‘No’’(didnotsmoke);‘‘Yes’’(smokedaday ormore),18 ‘‘No’’(didnotconsumefiveormorealcoholic drinksonasingleoccasion);‘‘Yes’’(consumedfiveormore alcoholicdrinksonasingleoccasion).19
Excessbodyfatwasmeasuredthroughtwoskinfolds (tri-cepsand subscapular) usinga Cescorf® caliper, according tothestandardization ofthe InternationalSociety forthe Advancementof Kinanthropometry (ISAK).Anthropometric measurementswereobtained byasingleevaluatorwitha level1ISAKcertification.Theresultsoftheskinfoldswere addedandanalyzed accordingtoLohman,20 takinggender intoaccount.Adolescentswithasum≥30mmand≥35mm, for boys and girls respectively, were classified as having excessbodyfat.
The descriptive analysis of the variables used means, standard deviations and frequency distribution. Data normality was verified through sampling distribution histograms;however, novariableshowed normal distribu-tion. The Chi-square test of heterogeneity was applied to identify differences in the prevalence of low lev-els of aerobic fitness according to the independent variables.
Binary logistic regression was employed and the odds ratio (OR) and 95% confidence interval were estimated. All variables were controlled for sexual maturation and introduced in the adjusted model irrespective of the p-value in the crude analysis. The analysis was performed hierarchically,23 divided into three blocks: 1 --- demo-graphic factors (Distal); 2 --- economic level and school shift (Intermediate 1); 3 --- lifestyle (Intermediate 2) and 4--- excessbodyfat(Proximal).Thevariableswithp-value <0.2024 remained in the adjusted model when the back-ward adjusted analysis was performed. The significance level was set at 5%. The analysis were performed using the Statistical Package for Social Sciences (SPSS) version 22.0, considering the effectof design andsample weight and are shown for the entire sample and stratified by gender.
Results
Ofthe1132analyzedstudents,253wereexcludedfromthe analysisfor notundergoingtheaerobicfitnesstest, which resultedin879students.Tables1and2showthe character-isticsofthesample.
Theprevalenceoflowaerobicfitnesswas87.5%(85.3% ofboysand89.4%girls).Adolescentswhowereinsufficiently active hadtwoor more hoursof screen time,had excess bodyfatandhigherprevalenceoflowlevelsofaerobic fit-ness(p<0.05)(Table3).Boysofwhiteethnicity,insufficiently activeandwithexcessbodyfathadahigherprevalenceof lowlevelsofaerobicfitness.Girlsthathadtwoormorehours ofscreentime,didnotsmokeandhadexcessbodyfathad ahigherprevalenceoflowlevelsofaerobicfitness(p<0.05) (Table3).
Thecrudeanalysisshowedthatadolescentsofwhite eth-nicitythattwoormorehoursofscreentime,whoconsumed alcoholinexcessandhadexcessbodyfatweremorelikelyto havelowlevelsofaerobicfitness(Table4).Intheadjusted analysis,the adolescentswhospenttwohoursor more in front ofthe screen,had inadequateconsumption ofmilk, wereinsufficientlyactiveandhadexcessbodyfatweremore likelytohavelowlevelsofaerobicfitness(Table4).
Table1 Totalandstratifiedvaluesbygenderofthemeanandstandarddeviationofage,anthropometricvariables,screen timeandaerobicscore.
Totalsample Male Female p-value
Age 16.2±1.1 16.2±1.1 16.1±1.1 0.15
Bodymass(kg) 61.7±12.2 65.4±12.0 58.3±11.3 0.25
Height(cm) 166.6±8.8 172.5±7.3 161.1±6.0 <0.01a
Screentime(h) 6.5±4.9 7.0±4.9 5.9±4.8 <0.01a
Triceps 14.9±7.3 10.7±5.1 18.7±6.9 <0.01a
Subscapular 13.3±6.7 10.7±4.8 15.6±7.3 <0.01a
Sumoffolds(mm) 28.2±13.4 21.5±9.5 34.3±13.6 <0.01a
Aerobicscore 388.1±58.3 426.8±53.4 353.3±36.6 <0.01a
M,mean;SD,standarddeviation.Sumoftricepsandsubscapularskinfolds.
ap≤0.05(Mann---Whitneytest).
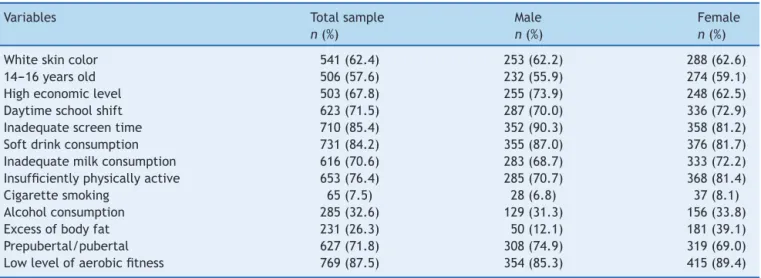
Table2 Distributionofthetotalandstratifiedsamplebygenderinrelationtosociodemographicfactors,lifestyle,excessof bodyfat,sexualmaturationandlevelofaerobicfitness.
Variables Totalsample Male Female
n(%) n(%) n(%)
Whiteskincolor 541(62.4) 253(62.2) 288(62.6)
14---16yearsold 506(57.6) 232(55.9) 274(59.1)
Higheconomiclevel 503(67.8) 255(73.9) 248(62.5)
Daytimeschoolshift 623(71.5) 287(70.0) 336(72.9)
Inadequatescreentime 710(85.4) 352(90.3) 358(81.2)
Softdrinkconsumption 731(84.2) 355(87.0) 376(81.7)
Inadequatemilkconsumption 616(70.6) 283(68.7) 333(72.2)
Insufficientlyphysicallyactive 653(76.4) 285(70.7) 368(81.4)
Cigarettesmoking 65(7.5) 28(6.8) 37(8.1)
Alcoholconsumption 285(32.6) 129(31.3) 156(33.8)
Excessofbodyfat 231(26.3) 50(12.1) 181(39.1)
Prepubertal/pubertal 627(71.8) 308(74.9) 319(69.0)
Table3 Sampledistributioninrelationtosociodemographicsignificantfactors,lifestyle,sexualmaturationandexcessofbody fatassociatedwiththelevelofaerobicfitness.
Aerobicfitness---total Aerobicfitness---malegender Aerobicfitness---femalegender
Normal/high Low Normal/high Low Normal/high Low
n(%) n(%) p-value n(%) n(%) p-value n(%) n(%) p-value
Skincolor 0.58 0.04a 0.64
White 59(10.9) 482(89.1) 30(11.9) 223(88.1) 29(10.1) 259(89.9) Mixed
race/Black/Yellow/Native Brazilian
50(15.3) 276(84.7) 30(19.5) 124(80.5) 20(11.6) 152(88.4)
Levelofphysical activity
0.01a 0.04a 0.32
Physicallyactive 36(17.8) 166(82.2) 24(20.3) 94(79.7) 12(14.3) 37(10.1) Insufficiently
physicallyactive
72(11.0) 581(89.0) 35(12.3) 250(87.7) 37(10.1) 331(89.9)
Screentime 0.02a 0.34 0.01a
Adequate 23(19.0) 98(81.0) 08(21.1) 30(78.9) 15(18.1) 68(81.9) Inadequate 82(11.5) 628(88.5) 52(14.8) 300(85.2) 30(8.4) 328(91.6)
Excessofadiposity <0.01a <0.01a <0.01a
No 104(16.1) 542(83.9) 61(16.8) 303(83.2) 43(15.2) 239(84.8)
Yes 06(2.6) 225(97.4) 00(0.0) 50(100.0) 06(3.3) 175(96.7)
Excessofadiposity=excessofbodyfat.Physicallyactive≥300min/week.
a p<0.05(Chi-squaretest).
Table4 Crudeandadjustedlogisticregressionanalysisbetweenlowaerobicfitnessandsociodemographicfactors,lifestyle andexcessofbodyfatinadolescents.
Variables Totalsample Male Female
Crude analysis
Adjusted analysis
Crude analysis
Adjusted analysisa
Crude analysis
Adjusted analysisa
OR(95%CI) OR(95%CI) OR(95%CI)
Non-whiteskin color
0.7(0.5---0.9)a 0.7(0.5---1.0) 0.6(0.3---0.9)a 0.6(0.3---0.9)a 0.9(0.5---1.6) 0.8(0.5---1.5)
Inadequatescreen time
1.8(1.1---3.0)a 1.7(1.1---3.0)a 1.5(0.7---2.0) 1.3(0.5---3.3) 2.2(1.1---4.3)a 2.3(1.1---4.5)a
Inadequatemilk consumption
1.7(1.1---2.6)a 1.7(1.1---2.6)a 1.2(0.7---2.1) 1.1(0.6---2.1) 1.6(0.8---2.9) 2.0(1.1---3.9)a
Insufficiently physicallyactive
1.6(1.1---2.5)a 1.6(1.1---2.4)a 1.8(1.1---3.2)a 2.0(1.1---3.7)a 1.5(0.7---3.0) 1.5(0.7---3.2)
Alcohol consumption
0.8(0.5---1.2) 0.8(0.5---1.3) 0.6(0.3---1.1) 0.7(0.4---1.2) 0.7(0.4---1.3) 1.1(0.5---2.1)
Cigarettesmoking 0.6(0.3---1.1) 0.5(0.2---1.1) 1.1(0.3---3.1) 1.2(0.4---4.0) 0.4(0.2---0.9)a 0.4(0.1---0.8)a Excessofbodyfat 7.9(3.1---20.2)a 7.9(3.19---20.1)a 32.5(27.6---40.0)a 35.5(26.0---45.0)a 5.2(2.1---12.6)a 6.1(2.3---16.2)a Post-pubertal 1.1(0.6---1.7) 1.1(0.6---1.8) 1.4(0.7---2.8) 1.6(0.8---3.2) 1.1(0.5---2.1) 0.9(0.4---1.9)
OR,oddsratio;CI,confidenceinterval.
Analysisadjustedforallthevariables,withcontrolbythesexualmaturation,regardlessofp-valueinthecrudeanalysis.
a p<0.05.
Inbothcrudeandadjustedanalyses,boysofwhite eth-nicity that were insufficiently active were more likely to have low levels of aerobic fitness. In the crude analysis, thegirlswhodidnotsmokeandhadexcessbodyfatwere morelikelytohavelowlevelsof aerobicfitness(Table4). Inthe adjustedanalysis,girls thathadtwoor morehours ofscreentimeandhadaninadequateconsumptionofmilk
were more likely to have low levels of aerobic fitness (Table4).
Discussion
Brazilianregionswith7057childrenandadolescents.2 The girlsinthisstudyhadahigherprevalenceoflowlevelsof aerobicfitnessthanboys.Thisfactisjustifiedbecausegirls practicelessphysicalactivityduringadolescenceandhave lowerleftventricularmasswhencomparedwithboys,which determineslowersystolicvolumeatrestandresultsinlower aerobicperformance.25
Forthetotalsampleandforthefemalegender,the ado-lescentsthathadtwoormorehoursofscreentimeshowed lowlevelsofaerobicfitness.Similarresultswerefoundina studycarriedoutintheUnitedStates.3Thatoccursbecause duringthetimespentwithelectronicdevices,adolescents failtoperformmoreintenseactivities,whichresultsinlow levelsofphysicalactivityandphysicalfitnessingeneral.5
Lowlevelsofaerobicfitnesswereassociatedwith inad-equateconsumptionofmilkinthetotalsampleandforthe female gender, which is similar to the study carried out inseven European countrieswithadolescents aged12---17 years.26 This finding is of concern, as milkis a source of protein,aminoacids,vitaminsandcarbohydrates(lactose), beingusedasenergybymuscles.15,26Additionally,milk nutri-entsareresponsibleforthereestablishmentoffluidbalance afterexercise-induceddehydration,andaidinmusclemass gain.15,26 Thus, theinadequateconsumption of milk influ-encesphysicalperformanceinchildhoodandadolescence.26 Inthetotalsampleandforthefemalegender,the ado-lescentswithexcessbodyfatwerenearlyeighttimesmore likelytohave low levels of aerobicfitness. Other studies havealsofoundanassociationbetweenthesevariables.3,25 Apossible justification is that individualswith high levels ofbodyfat aremorelikelytohavedifficultiesin locomo-tion,whichinfluencesintheeconomyofmovement,greater energyconsumptionandearlyfatigueinaerobicactivities, whichdecreasesperformanceinphysicaltests.6
The girls whodid notsmoke hadlow levels ofaerobic fitness.Thisfindingmaybeanassociationknownasafalse one,duetosystematicor randomerrors,inherentto epi-demiologicalstudiesbasedonempiricalobservationsfrom samples.27 Systematicerrorscanmakean associationthat actually does not exist look real.27 Additionally, the sys-tematicreview identifiedthat thereareno investigations onlow aerobic fitnessand smoking in adolescents,which emphasizes the need for studies to investigate the asso-ciationbetweenthesetwovariables.6 Whattheliterature affirmsisthat, althoughthe individualmight havea good levelofphysical activityor physicalfitness,smokingalone impairstheperformanceandgeneralhealth.28
Forthetotalsample andfor themalegender, the ado-lescents who were insufficiently active had low aerobic fitnesslevels, similartothe results found in a study car-ried out in Spain with adolescents aged 12---18 years.25 The association between these variables occurs because the insufficient physical activity practice or low-intensity activities are insufficient to meet the required threshold forcardiovascularadaptationsthatincreaseaerobicfitness levels.3,25
The white ethnicityin boysshowed low levelsof aer-obic fitness.This fact is justified becausewhite ethnicity adolescentsusuallyconstitutethe mostfavored economic classes.29Thus,theyhavegreateraccesstoconvenienceand fastfoodstores,TV,computersandvideogames,whichcan increasethetimespentinsedentaryactivities.29
The studylimitations were: 1--- thefact that the ado-lescentsknowtheyareparticipatinginastudyonlifestyle can,in itself,haveinfluencedthe lowprevalence results, especiallyregardingtheexcessiveconsumptionofalcoholic beveragesandcigarettes;2---asitwasnotpossibleto con-troltheadolescents’movementsbeforetheaerobicfitness test, some individuals mayhave initiated the test with a heartrateabovetherestingheartrate.
Thisinvestigationcontributestotheareaofstudy,asit shows different sociodemographic and lifestyle variables, chosen inordertodisclose agreater overviewof possible factorscorrelatedtothelowaerobicfitnesslevelsin ado-lescents andcontributes tothe analysisand discussion of modifiable socioculturaland behavioralaspectsthat influ-encethelowaerobicperformance.Additionally,itdiscloses dataontheaerobicfitnesslevelamongadolescentsfroma cityinsouthernBrazil,servingasacomparativeparameter forstudieswithyoungindividuals.Moreover,theassociation betweenlowlevelsofaerobicfitnessandsociodemographic factors,lifestyleandexcessofbodyfathighlightstheneed forplanningprogramstoimprovetheaerobicperformance ofstudents,aimingtoreducethehealthrisksgeneratedby thiscondition.
Theconclusionisthateightoftenadolescentshad inad-equatelevelsofaerobicfitnessforgoodhealth.Thewhite ethnicityandinsufficientlyactiveboysandnonsmokergirls thathadexcessofbodyfat,hadtwoormorehoursofscreen timeandhadinadequatemilkconsumptionweremorelikely tohavelowlevelsofaerobicfitness.
Funding
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Universal Public Notice 2013 (n◦ 472763/2013-0).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TomkinsonGR,LégerLA,OldsTS,CazorlaG.Seculartrendsin theperformanceofchildrenandadolescents(1980---2000):an analysisof55studiesofthe20mshuttleruntestin11countries. SportsMed.2003;33:285---300.
2.PelegriniA, Silva DA,Petroski EL, GlanerMF. Aptidão física relacionadaàsaúdedeescolaresbrasileiros:dadosdoprojeto esporteBrasil.RevBrasMedEsporte.2011;17:92---6.
3.Pate RR, Wang CY, Dowda M, Farrell SW, O’Neill JR. Car-diorespiratory fitness levels among US youth 12to 19 years of age: findings from the 1999---2002 National Health and Nutrition Examination Survey. Arch Pediatr Adolesc Med. 2006;160:1005---12.
4.CastelliDM,Hillman CH,Buck SM,ErwinHE.Physicalfitness andacademicachievementinthird-andfifth-gradestudents.J SportExercPsychol.2007;29:239---52.
6.Gonc¸alvesEC,SilvaDA,NunesHE.Prevalenceandfactors asso-ciatedwithlowaerobicperformancelevelsinadolescents:a systematicreview.CurrPediatrRev.2015;11:56---70.
7.Atlas Brasil [page on the Internet]. Atlas de
Desen-volvimento Humano do Brasil; 2013. Available from:
http://www.atlasbrasil.org.br/2013/[accessed20.11.14]. 8.CanadianSocietyforExercisePhysiology.TheCanadianphysical
activity,fitness &lifestyle appraisal:CSEP’s planfor healthy living.2aed.Ottawa:CSEP;1998.
9.WellerIM, ThomasSG, GledhillN,Paterson D,Quinney A. A studytovalidatethemodifiedCanadianAerobicFitnessTest. CanJApplPhysiol.1995;20:211---21.
10.GuedesDP,LopesCC.Validac¸ãodaversãobrasileiradoyouth riskbehaviorsurvey2007.RevSaudePublica.2010;44:840---50.
11.Brasil---InstitutoBrasileirodeGeografiaeEstatística.Pesquisa NacionaldeSaneamentoBásico---2008.RiodeJaneiro:IBGE; 2010.
12.Brasil---Associac¸ãoBrasileiradeEmpresasdePesquisa.Critério declassificac¸ãoeconômicaBrasil.SãoPaulo:ABEP;2010.
13.American Academy of Pediatrics; Committee on Public Edu-cation.Children, adolescents, and television.Committee on PublicEducation.Pediatrics.2001;107:423---6.
14.RanjitN,EvansMH,Byrd-WilliamsC,EvansAE,HoelscherDM. Dietaryand activity correlates ofsugar-sweetened beverage consumptionamongadolescents.Pediatrics.2011;126:754---61.
15.Brasil ---Ministério da Saúde.Secretariade Atenc¸ãoà Saúde --- coordenac¸ão-geral da política de alimentac¸ão e nutric¸ão. Guia alimentar para a populac¸ão brasileira: promovendo a alimentac¸ãosaudável.Brasília:MinistériodaSaúde;2005.
16.WorldHealthOrganization.Globalrecommendationson physi-calactivityforhealth.Geneve:WHO;2010.
17.StrongWB, Malina RM,Blimkie CJ, Daniels SR, DishmanRK, GutinB,etal.Evidencebasedphysicalactivityforschool-age youth.JPediatr.2005;146:732---7.
18.Organizac¸ãoMundialdaSaúde.Organizac¸ãoPan-Americanade Saúde.Whoreportontheglobaltobaccoepidemic,2008:the MPOWERpackage.Geneva:OMS;2008.
19.MidanikLT.Drunkenness,feelingtheeffectsand5meassures. Addiction.1999;94:887---97.
20.LohmanTG.Theuseofskinfoldtoestimatebodyfatnesson childrenandyouth.JOPERD.1987;58:98---102.
21.TannerJM.Growth atadolescence; withageneral consider-ation oftheeffects ofhereditaryand environmental factors upon growthand maturation frombirth tomaturity. Oxford: BlackwellScientific;1962.
22.Matsudo SM, Matsudo KR. Self-assessment and physician assessment ofsexual maturation in Brazilianboys and girls: concordance and reproducibility. Am J Hum Biol. 1994;6: 451---5.
23.VictoraCG,HuttlySR, FuchsSC,OlintoMT.Theroleof con-ceptualframeworksinepidemiologicalanalisys:ahierarchical approach.IntJEpidemiol.1997;26:224---7.
24.Maldonado G, Greenland S. Simulationstudyof confounder-selectionstrategies.AmJEpidemiol.1993;138:923---36.
25.Morales-Suárez-VarelaMM,Clemente-BoschE,Llopis-González A.Relationshipbetweenthelevelofphysicalactivityand mark-ersofcardiovascularhealthinValencianadolescents(Spain). ArchArgentPediatr.2013;111:398---404.
26.Cuenca-GarcíaM,OrtegaFB,HuybrechtsI,RuizJR, González-Gross M, Ottevaere C, et al. Cardiorespiratory fitness and dietaryintakeinEuropeanadolescents:theHealthyLifestyle in Europe by Nutrition in Adolescence study. Br J Nutr. 2012;107:1850---9.
27.MedronhoRA,BlochKV,LuizRR,WerneckGL.Epidemiologia. 2aed.SãoPaulo:Atheneu;2009.
28.CostaAA,ElabrasFilhoJ,AraújoML,FerreiraJE,MeirellesLR, MagalhãesCK.Programamultiprofissionaldecontroledo tabag-ismo:aspectosrelacionadosàabstinênciadelongoprazo.Rev SOCERJ.2006;19:397---403.