REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
Care
needs
of
children
with
disabilities
---
Use
of
the
Pediatric
Evaluation
of
Disability
Inventory
Fernanda
Moreira
Teles,
Rosa
Resegue,
Rosana
Fiorini
Puccini
∗UniversidadeFederaldeSãoPaulo(Unifesp),SãoPaulo,SP,Brazil
Received10September2015;accepted14February2016 Availableonline6September2016
KEYWORDS
Healthofindividuals withdisabilities; Childrenwith disabilities; Rehabilitation; Dailyactivities
Abstract
Objective: Todescribethecareneedsreportedbycaregiversofchildrenwithdisabilitiesgoing throughtheschoolinclusionprocessusingthePediatricEvaluationofDisabilityInventory.
Methods: Cross-sectionalstudywith181childrenaged7---10yearswithphysicalormental dis-abilities,undergoingtheinclusionprocessinelementaryschoolin2007.Location:31schoolsof theRegionalEducationBoard---DistrictofPenha,EastSidethecityofSãoPaulo.Thechildren’s careneedsaccordingtothecaregiverswereassessedinthreeareas---self-care,mobilityand socialfunction,usingthePediatricEvaluationofDisabilityInventory,accordingtothe follow-ingscore:5,Independent;4,Supervision;3,MinimumAssistance;2,ModerateAssistance;1, MaximumAssistanceand0,TotalAssistance.Forstatisticalanalysis,weusedStudent’st-test andanalysisofvariance(ANOVA),withp<0.05beingstatisticallysignificant.
Results: Thelowermeans,withstatisticallysignificantdifferences,wereobservedfortheitems relatedtosocialfunction(55.8---72.0),followedbyself-carefunctions(56.0---96.5);foralltypes ofdisabilities,exceptforchildrenwithphysicaldisabilities,whohadlowermeansforself-care (56.0)andmobility(63.8).
Conclusions: Socialfunctionwastheareareferredtoastheonethatneededahigherdegree ofassistancefromthecaregiverandthePediatricEvaluationofDisabilityInventoryisatool thatcanhelpidentifytheseneedsanddevelopamoretargetedintervention.
©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](R.F.Puccini).
http://dx.doi.org/10.1016/j.rppede.2016.02.015
PALAVRAS-CHAVE
Saúdedapessoa comdeficiência; Crianc¸ascom deficiência; Reabilitac¸ão; Atividadescotidianas
Necessidadesdeassistênciaàcrianc¸acomdeficiência---UsodoInventáriode Avaliac¸ãoPediátricadeIncapacidade
Resumo
Objetivo: Descreverasnecessidadesdeassistênciareferidasporcuidadoresdecrianc¸ascom deficiênciaemprocessodeinclusãoescolar,pormeiodoInventáriodeAvaliac¸ãoPediátricade Incapacidade.
Métodos: Estudotransversalcom181crianc¸asde7-10anoscomdeficiênciasfísicasou men-tais,queseencontravamemprocessodeinclusãoescolarnocicloFundamentalI,em 2007. Local:31escolasdaDiretoriaRegionaldeEnsino---DistritoPenha,ZonaLestedoMunicípiode SãoPaulo. Foramavaliadas as necessidades de assistência do cuidador dacrianc¸a em três áreas---autocuidado,mobilidadeefunc¸ãosocial,pormeiodoInventáriodeAvaliac¸ãoPediátrica de Incapacidade, segundo aseguintepontuac¸ão:5Independente, 4Supervisão, 3 Assistên-ciamínima,2Assistênciamoderada,1Assistênciamáximae0Assistênciatotal.Paraanálise estatística,usou-seotestetdeStudenteanálisedevariância(Anova)efoisignificativop<0,05.
Resultados: As menores médias,comdiferenc¸a estatística, foramobservadas para ositens relacionadosàfunc¸ãosocial (55,8-72),seguidas dasfunc¸ões de autocuidado(56-96,5) para todosostiposdedeficiência,comexcec¸ãodascrianc¸ascomdeficiênciafísicaqueapresentaram menoresmédiasparaautocuidado(56)emobilidade(63,8).
Conclusões: Afunc¸ãosocialfoiaáreareferidacomoaquenecessitademaiorassistênciado cuidadoreoInventáriodeAvaliac¸ãoPediátricadeIncapacidadeéuminstrumentoquepode contribuirparaidentificar essasnecessidadeseparaodesenvolvimentodeumaintervenc¸ão maisdirigida.
©2016SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpenAccesssobumalicenc¸aCCBY(http://creativecommons.org/licenses/by/4.0/).
Introduction
Theinclusionof thedisabledchild isaprocessthatstarts within the family environment. This environment can be definedasasignificantsocialunitwithinsociety,influences the determination of human behavior and the person-ality formation of its members.1 The birth of a child withdisability brings significant changes to the organiza-tion and structure of families and the decisive role that these have in the child’s rehabilitation process is recog-nized, regarding the child’s development as well as her independence in functional abilities.2 In this process,the socialsupportreceivedbythecaregivers ofthechildwith disabilities is critical, as it lessens the parents’ stress and promotes a more adequate bonding with the child.3 The family’s response to this challenge depends on their previous experience, sociocultural aspects, family rela-tionships and the existence of social support network for this condition, especially in the areas of education and health.2
Theschool,inadditiontoitstraditionalaimofpromoting educationandsocialintegration,playsakeyrolein revers-ingexclusionsituationsbypromotingawarenessactionson therightsofindividualswithdisabilities.4,5Inclusive educa-tionisdefinedasthesetofeducationalprocessesbelonging toarticulatedpoliciesthat preclude anytype of segrega-tionand isolation. These policies seek toincrease access toregularschool,broadentheparticipationandensurethe permanenceofstudents,regardlessoftheircharacteristics. Froma practical point of view, inclusive education guar-anteesthatall childrenhave accesstoelementaryschool education.6
In 1990, in Brazil, this program was supported by the accomplishments established in the Federal Constitution (1988), which guarantees equal access to education and permanence at school. It emphasizes the Government’s responsibilityforeducation,representedbyobligatory ele-mentaryeducationthatisfreeforall,includingthosethat didnothave accesstoitatan appropriateage,aswellas specializededucationalservicesforindividualswith disabil-ities,preferablywithintheregularschoolsystem.7
Thus,thisstudywascarriedoutinordertodescribethe caregiver assistance provided tochildren with disabilities duringtheinclusionprocess,throughthePediatric Evalua-tionofDisabilityInventory(PEDI).
Method
This wasananalytical cross-sectionalstudy carriedoutin the municipal elementary schools of the City Hall of São Paulo,theRegionalEducationBoard---DistrictofPenha,East Zone of SãoPaulo, Brazil. Eachof the 13regional educa-tionboardsareresponsibleforagroupofschoolsandhave asupportservicefortheinclusion,Cefai---Centerfor Educa-tionandTrainingSupportforInclusion(CentrodeEducac¸ão e Formac¸ão de Apoio à Inclusão). This service supervises the monitoring of students with disabilities through sys-tematicvisitstoschools,educationalevaluation,meetings withteachersand coordinators, contactwithparents and themappingofcareintheregion.Theschoolswithhigher numbers of children with special needs also have rooms to support inclusion, called SAAI---Support and Monitoring of Inclusion Rooms. These rooms are intended for edu-cational support as a complementary, supplementary or exclusive service offered to students who have a dis-ability(http://portal.sme.prefeitura.sp.gov.br/Main/Page/ PortalSMESP/Atendimento-Educacional-Especializado).
Of the 33 schools of the DRE---District of Penha, East Zone of São Paulo, 31 had children with disabilities enrolled in them, which were included in this study.The researcher contacted the principal or teachers of these schoolsanddisclosedtheobjectivesandproceduresofthe research.Onthisoccasion,informationabouttheinclusion process developed at each school---accessibility, qualified teachers,systematicmeetingswithparents,their difficul-ties, including discussion and shared definition of school gradeprogression---werealsoobtained.
This population consisted of children aged 7---10 years, undergoing school inclusion process in elementary school---1stto4thgrades(beforeelementaryschoolstarted toinclude9thgrade),in2007.Thetotalnumberofchildren withdisabilitiesthathadadiagnosticreportwasconsidered; the listof the children wasprovided byCefai---Center for Education andTrainingSupportforInclusion---Regional Dis-trictofPenha,totaling200childrenin2007.Fromthelist ofstudents, parentsor caregivers wereinvitedto partici-pate;theinterviewwasscheduledandcarriedoutatschool bytheresearcher.Ofthe200children,19wereexcluded: 16forbeingabsentorduetodifficultiesincompletingthe questionnaireand3duetorefusaltoparticipate.Thus,the finalstudypopulationconsistedof181children.Regarding thetypeofdisability,thisstudyadoptedthenomenclature usedbyCefai,whichisdescribedbelow:
Typical behavior: group of children with a diagnosis of
hyperactivity, psychiatric diseases, behavioral disorders andacquired cognitiveimpairment,includingmental dis-abilitiesatalllevels.
GDD---global developmental disorder: group of children
with autism of all types (mild, moderate, severe) and Asperger’s.This termis usedbythe MunicipalEducation Secretariat(SME---SecretariaMuinicipaldeEducac¸ão)---and
corresponds totheInternational ClassificationofDisease (ICD)10---F84.
Physicaldisability:disabilitiesduetomissinglimbs,
asym-metric limbs, as well as bone deformities and motor disabilities.
Geneticsyndromes:groupwithadiagnosisofgenetic
syn-dromes.
Downsyndrome(DS):Cefaiclassifiesthisgroupseparately.
Multiple disabilities: Childrenwith twoor more
disabil-ities. This group includes children that have disabilities associatedtoanyotherdisorder/disease.Example:motor disabilities andepilepsy; hearing and visualimpairment, amongothers.
Otherdisabilities:correspondtothediagnosesofdiseases
such as amplified musculoskeletal pain syndrome, visual impairment,dyslexia,speechdisordersandothers.
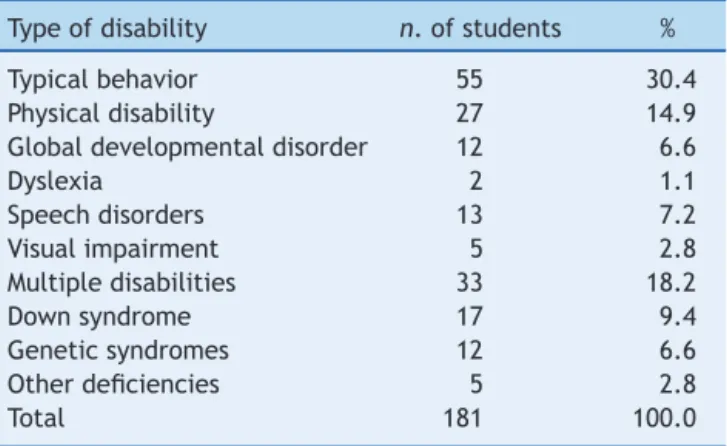
Table1shows thedistributionof studentsaccording to thetypeofdisability.Itcanbeobservedthattypical behav-ioris themost commonone,followed bythe groups with multipledisabilitiesandphysicaldisabilities.
Thecaregiverwasinterviewedusingastructured ques-tionnaire.Acaregiverwasconsideredasanyone,regardless ofthedegreeofkinship,whoaccompaniedthechildrenin theirdailylivesduringdailyactivities.
Theevaluationoftheneedforcaregiverassistancewas carried out through the Pediatric Evaluation of Disability Inventory---PEDI.ThePediwasdevelopedbyHaleyetal.in 1992andvalidatedfortheBrazilianpopulation byMancini in2005.Itisastructuredquestionnaireconsistingofthree parts.Part Ievaluatesthe functionalabilitiesof thechild in the areas of self-care (73 items), mobility (59 items) and social function (65 items), with a score of 1 when the child performs the assessed item and of 0 when the child cannot perform it. Part II is related to the need for help provided by the caregiver for the performance of20 itemsin the sameareas evaluatedinthe firstpart, self-care,mobility andsocial function,withthe following scores: 5---Independent, 4---Supervision, 3---Minimum assis-tance,2---Moderateassistance,1---Maximum assistanceand 0---Totalassistance.Examples ofcaregiverassistance: Self-care---eats and drinks at regular meals; Mobility---mobility indoors,canwalk15metersanddoesnotincludeopening
Table1 Typeofdisabilityofchildrenundergoingthe inclu-sionprocess.DiretoriaRegionaldeEnsino---Penha,SãoPaulo (2007---2009).
Typeofdisability n.ofstudents %
Typicalbehavior 55 30.4
Physicaldisability 27 14.9 Globaldevelopmentaldisorder 12 6.6
Dyslexia 2 1.1
Speechdisorders 13 7.2
Visualimpairment 5 2.8
Multipledisabilities 33 18.2
Downsyndrome 17 9.4
Geneticsyndromes 12 6.6
Otherdeficiencies 5 2.8
doorsorcarryingobjects;Socialfunction---functional under-standing, understanding requests and instructions. The interviewedcaregiversindicatedtheoptionthatwasrelated totheassistancerequiredbyeachchildineachofthe func-tions.PartIIIofthetoolevaluatesthechanges/adjustments necessaryinthechild’senvironmentfortheactivities.The researcherwastheonlyonetoapplythePEDIafter train-ingrecommendedbytheauthors;althoughthePEDIcanbe appliedwithoutthepresenceofthepatient,thisstudyused theinterviewmethodsimultaneouslytodirectobservation ofthechild.8
Inthisarticle,weanalyzedtheresultsregardingthe care-giverandtheneed for caregiver assistance(Part II ofthe PEDI).Theanalyseswiththeoriginalscoreofitems(means) weretransformedinto0---100scales,assuggestedby McDow-ellandNewell.9
Transformedscale
=(originalscore−lowestpossiblescore)
originalscaleamplitude ×100
Student’s t test or analysis of variance (ANOVA) was usedtocomparethesubscalesbetweenthestudyvariables, considering a 5% significance level. Comparisonsbetween the three scales (self-care, mobility and social function) werecarriedoutforeach groupofchildrenwithdifferent diagnosesthroughanalysisofvariancewithrepeated meas-ures(univariate). Whentherewasa significant difference between thescales, this differencewas identifiedby the Bonferroni’smultiplecomparisontest.
Thisstudywasapproved,on07/20/2007,bythe Institu-tionalReview BoardofUniversidadeFederal de SãoPaulo (CEP:1115/07).
Results
Of the 181 interviewed caregivers, 92.3% were females. Table2describestheeducationallevelofcaregivers.Itwas observed that more than 50% of the caregivers had com-pletedelementaryschoolorhadmoreyearsofstudy.
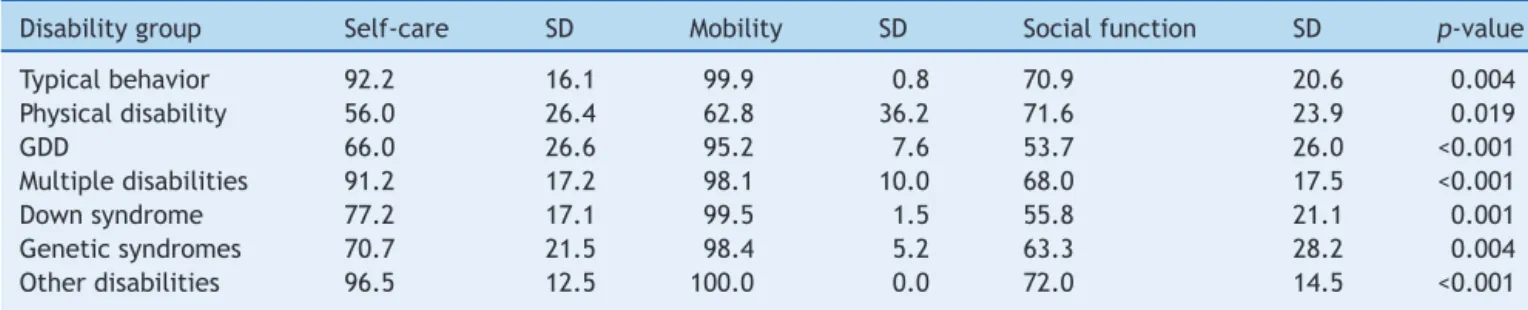
Table3shows themeanscoresobtainedfromthe care-giverinrelationtotheneedforassistanceforeachofthe functionsinthe threeareas---self-care,mobility andsocial function. There was a significant difference between the threescalesin the areas of self-care,mobility and social functionforalltypesofdisabilities.Socialfunctionwasthe mostaffectedinalltypesofdisabilities,exceptforphysical
Table 2 Educational level of caregivers of children undergoing the inclusion process. Diretoria Regional de Ensino---Penha,SãoPaulo(2007---2009).
Levelofschooling Numberof caregivers
%
Illiterate 07 3.0
Didnotfinish5thyear ofelementaryschool
17 9.4
Finished5thyearofelementary school
24 13.3
Didnotfinish9thyear ofelementaryschool
31 17.1
Finished9thyearofelementary school
33 18.2
Didnotfinishhighschool 5 2.8 Finishedhighschool 54 29.8 Didnotfinishcollege/university 4 2.2 Finishedcollege/university 6 3.3
Total 181 100.0
disability,whichshowedthelowestmeanforself-care.Also noteworthy wastheglobal developmentaldisorder, which showedlowervaluesforsocialfunction.Themobilityscale achieved,onaverage,betterresultsforalltypesof disabil-ities,withtheexceptionofphysicaldisability.
Foranitemizationoftheseresults,theanalysisof multi-plecomparisonswascarriedoutforeachtypeofdisability, ofwhichresultsareshownbelow:
Typical behavior---there was a statistically significant difference between the mean values obtained with self-care×mobility (p-value=0.003) and mobility×social
function(p=0.004).
Physicaldeficiencygroup---therewasastatistically signif-icantdifferencebetweenthemeanvaluesobtainedwith self-care×socialfunction(p=0.019).
GDD---there was a statistically significant difference between the mean values obtained between self-care×mobility (p=0.001); self-care×social function
(p=0.030);mobility×socialfunction(p<0.001).
Multiple disabilities---there was a statistically significant differencebetweenthemeanvalueswithself-care×social
function(p<0.001)andmobility×socialfunction(p<0.001).
Downsyndrome---therewasa statisticallysignificant dif-ferencebetweenthemeanvalueswithself-care×mobility
Table3 Needfor assistancereportedby thecaregiver,accordingtothe typeofdisability.Meansandstandarddeviations obtainedintheareasofself-care,mobilityandsocialfunction.DiretoriaRegionaldeEnsino---Penha(2007---2009).
Disabilitygroup Self-care SD Mobility SD Socialfunction SD p-value
Typicalbehavior 92.2 16.1 99.9 0.8 70.9 20.6 0.004
Physicaldisability 56.0 26.4 62.8 36.2 71.6 23.9 0.019
GDD 66.0 26.6 95.2 7.6 53.7 26.0 <0.001
Multipledisabilities 91.2 17.2 98.1 10.0 68.0 17.5 <0.001
Downsyndrome 77.2 17.1 99.5 1.5 55.8 21.1 0.001
Geneticsyndromes 70.7 21.5 98.4 5.2 63.3 28.2 0.004 Otherdisabilities 96.5 12.5 100.0 0.0 72.0 14.5 <0.001
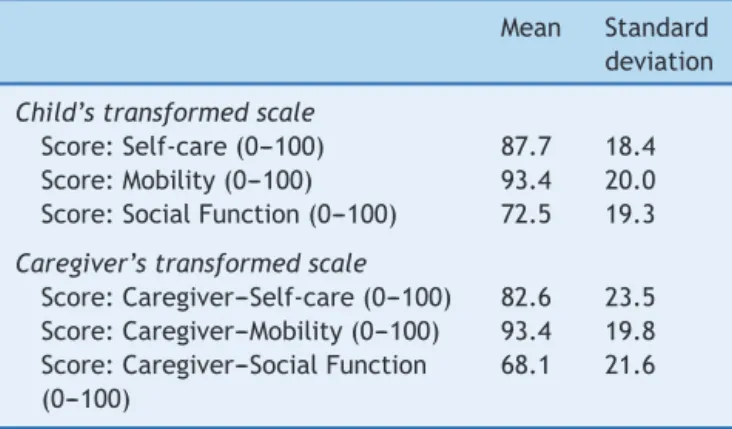
Table 4 Functional abilities of children undergoing the inclusionprocess andthe needfor assistancereportedby thecaregiver,accordingtotheareasofself-care,mobility andsocialfunction.DRE---Penha,SãoPaulo(2007---2009).
Mean Standard deviation
Child’stransformedscale
Score:Self-care(0---100) 87.7 18.4 Score:Mobility(0---100) 93.4 20.0 Score:SocialFunction(0---100) 72.5 19.3
Caregiver’stransformedscale
Score:Caregiver---Self-care(0---100) 82.6 23.5 Score:Caregiver---Mobility(0---100) 93.4 19.8 Score:Caregiver---SocialFunction
(0---100)
68.1 21.6
(p<0.001); self-care×social function (p<0.001); and
mobility×socialfunction(p<0.001).
Genetic syndromes---there was a statistically significant differencebetween themean valuesobtained with self-care×mobility (p=0.003) and mobility×social function
(p=0.004).
Otherdisabilities---therewasastatisticallysignificant dif-ference between the mean values with self-care×social
function(p=0.002)andmobility×socialfunction(p<0.001).
Itcanbeobservedthattheself-careandsocialfunction areasshow,inmostcases,adifferenceinrelationto mobil-ity,exceptforphysical disability.Theseareas are,for the caregivers, theones that requiretheir participation,i.e., theonesthatmostoftenrequiretheirhelp.
Table 4 shows the scores obtained by the children (Child’s Transformed Scale) according to the child’s func-tional abilities referred by the caregiver and the results obtained regarding the need for caregiver assistance for these activities---Caregiver’s Transformed Scale. One can observethatthemeansobtainedbychildrenintheassessed activities are similartothe need for caregiver assistance ineveryarea,andthatsocialfunctionistheareawiththe lowestscores.
Discussion
ThisstudywascarriedoutinaregionofSãoPaulocityand, althoughtherearedifferencesinrelationtothe socioeco-nomicstatusofeachregion,regardingtheactionsdeveloped byschoolsintheinclusionprocessandresourcesforsocial support,theresultsofthisstudy,whichdescribesthecare needs of children with disabilities, disclose the daily life facedbyparentsofthesechildren.Theyalsoindicate pos-sibleactionstobedevelopedwithfamiliesasan essential partoftheinclusionprocess.
Differentaspectscanhaveapositiveornegativeeffect on the parents’ performance potential, especially those regarding education. Lopes and Corrêa10 describe that since a very early age, the disabled child and his family are referred to different health or education profession-als, which, in turn, giveseveral recommendations on the
necessarycare.Therefore,theparentsarethemainagents whoact for the stimulationor training of some functions andare also responsible for the exchangeof information betweentheschoolandthefamilyunit,onhowthechild performssome activitiesand thedegree of independence whenperformingthem.11,12
The parents’ behavior strongly influencesthe develop-mentofchildrenandtheirwell-being.Positiveinteractions with one’s children are associated with their positive cognitive,behavioralandpsychosocialdevelopment.A lon-gitudinalstudythatfollowedsincebirthagroupofCanadian children and young individuals with neurological disor-ders and behavioral problems found that the caregiver’s demeanormightinfluencethechildren’sdevelopment.The authorsalso considered sociodemographic characteristics, concludingthatparentsofchildrenwithseveralhealth prob-lemshavelesspositiveandlessconsistentattitudes,which caninfluencetreatmentefficiency.12
Thus,theinclusionprocessofa disabledchilddepends onfamilysupport,aswellasonthecaregiver’seducational level.Inourstudy,approximately50%ofcaregivers,inmost cases the child’s mother, had elementary school or more yearsofschooling,whichisapositivefactortounderstand theguidelines,seekaccesstohealthservicesandother sup-portequipmenttocareforthedisabledchild.Thefactthat thesechildrenareincludedintheeducationalsystemmay alreadybetheresultofafamilyprofilethathasaccessto information,knowstheirrights,andvaluesandrecognizes theimportanceforthechildtoattendschool.
Theinclusionprocessrequires,ontheotherhand, inte-grationwithotherareas,especiallyhealthandsocialcare. The Brazilian Constitution(1988) guarantees the equality ofconditions tohave accesstoand remain at schooland emphasizestheGovernment’sresponsibilitytoprovide edu-cation,includingthosethatitdidnothaveaccesstoitat an adequate age, aswell as specialized educational ser-vicesforindividualswithdisabilities,preferablywithinthe regularschoolsystem.7However,manybarriersneedtobe overcomeforitsimplementation.Historically,thecare ini-tiativesforindividualswithdisabilitiesweremainlyfocused onphilanthropy,institutionalizationandsegregation.13 The progressiveexpansionofthemunicipalities’role,thechange in the concept of segregation into an inclusion one and healthpoliciesthatseekintegratedactionsconstitutea pos-sibilitytoovercomemorelimitedactionsaimedatspecific typesofdisability.14Theresultsofthisstudyshowthatforall typesofdisabilities,includingphysicalones,thereisgreater need for parentalhelp in relation to self-care and social functionactions.Therefore,specificactionsfocusedonthe disabilityaloneandnotonthechildrenandtheir families willnotbeabletopromoteanactualinclusion.
Thecareofchildrenwithdisabilitiesrequiresacare sys-temthatwillsponsortheparticipationanddevelopmentof partnershipsof thesefamilieswithhealth, education sys-temsandsocialsupportnetworks,reorganizingthespecific needsofparentsandsiblingsofchildrenwithdisabilitiesin ordertoofferstrategiessotheycanachievephysical, emo-tionalhealth andwell-being, includingsupportgroups for thefamilyandmentalhealthservices.15,16
socioeconomicaspectsofthe familymembers,which also influencedthesocialsupportreceivedbythecaregivers.17
Mantoandescribestheevolutionoftheconceptsof dis-ability and maladjustment, stating that the individual’s characteristics for a long time constituted the only goal of educational interventions. However, the author points out that, currently, no educational model can ignore the functioncharacteristicsofindividualswithintellectual dis-abilities, without considering their interaction with their familiesand withthe environment.18 Silveira etal.19 ana-lyzed the concepts of educators and family members of childrenwithmultipledisabilitiesundergoingtheinclusion process.Theresultsindicatedthatparentsperceivedtheir children’sdisabilities assomethingthat caused great suf-fering and social impairment and that, similarly to the teachers,theydidnotbelievetheschoolinclusionofthese children waspossible, as theythought the regularschool wasunpreparedtowelcomethem.
According to Sá and Rabinovich,20 in the study ‘‘Understandingthe familyof the child withphysical dis-abilities’’,thefamilysupportnetworkfavorstheformation of bonds and the structuring of the life of the physically disabledchild, expanding theirpossibilitiesfromthe self-esteemarisingfromaffectivity.Throughthecarerelations, familytransmits valuessuch astolerance andrespect for differences,corroboratingtoanadequatedevelopment.
Inthisstudy,socialfunctionwasthemostoftenaffected one,includinginchildrenwithphysicaldisabilities, corrob-oratingtheimportanceofthefamilyandtheschoolintheir inclusion process. The PEDI showed to be a tool capable ofprovidinga moredetailedidentification of the difficul-tiesin each ofthe functionalabilities, withthepotential tocontribute toa more targetedintervention of parents andeducators,aimedtoovercomethoseneedswhen pos-sible. The results of actions and strategies developed by parentsand teacherscan bemeasured, asthe PEDI iden-tifiesthechildren’sabilities,their needfor care provided byacaregiverandindicatesaredirectionoftheseactions.
In other studies, the PEDI showed to be effective in assessing differences in functional performance and the need for caregiver assistance, encouraged and helped to identifylossesregardingthechild’sperformance,allowing thecaregivertoaccompanytheevolutionoftreatmentand collaboratewiththetreatmentplan.21,22
Althoughitwasinitiatedin2007,theprocessofinclusion of children withdisabilities in regular schools constitutes apermanentchallenge.Theresults ofthisstudy can con-tributetothediscussionofbenefitsobtainedbyusingtools toassesscapacitiesandneedsofchildrenwithdisabilities whilemonitoringthisprocess.Itiswellestablishedthatthe educationofthechildwithdisabilityisacomplexactivity, asitrequiresadjustmentstothecurriculumthatnecessitate carefulmonitoringbyeducatorsandparents.Ontheother hand,attendinga regularschool willallow thechild with disabilityto progressively acquireknowledge that willbe demandedbysocietyandofwhichbasesareindispensable fortheindividual’sformation.
The PEDI,togetherwithother toolsfor theassessment andmonitoringofthechildundergoingtheinclusionprocess cancontributetotheidentificationoflimitsandmore spe-cificinterventionpossibilities, notonlyfor eachchild,but alsoforallchildrenwithdisabilities,throughdirectactions
ofeducatorsandtheworkdevelopedwiththeirfamily mem-bers. Inthis study,itsusemoreobjectively demonstrated thatthesocialfunctionistheonethatrequiresmore assis-tance from the caregiver, who, in addition to guidance, needssupporttoface thedemands ofthis condition.The heavyemotionalburdeninvolvedinthecareofchildrenwith disabilitieshasbeenwellestablishedandtheresponsethe familywillgivetothischallengewilldependonpast expe-riences,theeconomicsituation,aswellasculturalaspects and family relationships. The school, parents and society shouldallbeinvolvedinthisprocess.
Basedonthethesis
Identificationofincapacitiesindisabledchildrenattending municipal schools belonging to DRE---DiretoriaRegional de Ensino---Penha---SãoPaulo,throughPEDI---PediatricEvaluation ofDisabilityInventory,presentedatUniversidadeFederalde SãoPaulo---2011.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.DessenMA,SilvaNL.Deficiênciamentalefamília:umaanálise daproduc¸ãocientífica.Paideia.2000;10:12---23.
2.Batista SM,Franc¸a RM. Família de pessoas com deficiência: desafiosesuperac¸ão.RevdivulgtéccientICPG.2007;3:117---21.
3.NunesMA.Operfildocuidadordacrianc¸aportadoradeparalisia cerebral.RevMeioAmbSaude.2007;2:1---21.
4.Brazil.PresidênciadaRepública.Lein◦9.394,dedezembrode
1996.Estabeleceasdiretrizesebasesdaeducac¸ãonacional. Brasília:DiárioOficial;1996.
5.PupoDT,MeloAM,FerrésSP.Acessibilidade:discursoeprática nocotidianodabiblioteca.Campinas:BibliotecaCentralCésar Lattes;2006.
6.CarneiroMA. Oacesso de alunos com deficiência àsescolas eclassescomuns:possibilidadeselimitac¸ões.Petrópolis(RJ): Vozes;2007.
7.Brazil---Constituic¸ãodaRepúblicaFederativadoBrasilde1988. Atualizada em 2015. Available at: http://www.trtsp.jus.br/ legislacao/constituicao-federal-emendas[cited07.01.16]. 8.ManciniMC.Inventáriodeavaliac¸ãopediátricadeincapacidade
(Pedi)manualdaversãobrasileiraadaptada.BeloHorizonte: EditoraUFMG;2005.
9.McDowell,NewellC.Measuringhealth.Oxford:Oxford Univer-sityPress;1996.
10.LopesGB,KatoLS,CorrêaPR.Ospaisdascrianc¸ascom defi-ciência:reflexõesacercadaorientac¸ãoemreabilitac¸ãomotora. PsicolTeorPrat.2002;4:62---7.
11.PavãoSL,SilvaFP,RochaNA.Efeitodaorientac¸ãodomiciliarno desempenhofuncionaldecrianc¸ascomnecessidadesespeciais. Motricidade.2011;7:21---9.
13.CoelhoAE,LoboST.Gestãoparticipativanaorganizac¸ãodeuma rededereabilitac¸ãoemsaúdepública.RevVirtGestãoIniciat Soc.2004;1:37---45.
14.Brazil---SecretariaNacionaldePromoc¸ãodosDireitosdaPessoa comDeficiência [homepage onthe Internet]. Plano nacional dos direitos da pessoa com deficiência: viver sem limite. Availableat:http://www.pessoacomdeficiencia.gov.br/[cited 14.05.15].
15.Murphy NA, Carbone PS. Council on children with dis-abilities. Parent---Provider---Community partnerships: optimi-zing outcomes for children with disabilities. Pediatrics. 2011;128:795---802.
16.ResegueR,PucciniRF,SilvaEM.Fatoresderiscoassociadosa alterac¸õesdedesenvolvimentoemcrianc¸asdealtorisco acom-panhadasem ambulatóriomultidisciplinar. Sao Paulo MedJ. 2008;126:4---10.
17.FerreiraHG[master’sthesis]Aspectosfamiliaresenvolvidosno desenvolvimentodecrianc¸ascomparalisiacerebral.Ribeirão Preto(SP):USP;2007.
18.Mantoan MT.Educac¸ãoescolar dedeficientesmentais: prob-lemas para a pesquisa e o desenvolvimento. Cad CEDES [homepage on the Internet]. 1998;19. Available at: http:// www.scielo.br/scielo.php?script=sci arttext&pid=S0101-32621998000300009[cited29.04.15].
19.SilveiraFF,Neves MM.Inclusãoescolarde crianc¸ascom defi-ciênciamúltipla:concepc¸õesdepaiseprofessores.PsicolTeor Pesq.2006;22:79---88.
20.Sá SM, Rabinovich EP. Compreendendo a família da crianc¸a comdeficiênciafísica.RevBrasCrescimentoDesenvolvHum. 2006;16:68---84.
21.MourãoLM,AraújoA.Capacidadedoautocuidadodecrianc¸as comparalisiacerebralatendidasemumcentrodereferência. REnfermCentOMin.2011;1:368---76.