REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
The
effect
of
sugammadex
on
postoperative
cognitive
function
and
recovery
Özcan
Pis
¸kin
a,∗,
Gamze
Küc
¸ükosman
a,
Deniz
Utku
Altun
b,
Murat
C
¸imencan
a,
Banu
Özen
c,
Bengü
Gülhan
Aydın
a,
Rahs
¸an
Dilek
Okyay
a,
Hilal
Ayo˘
glu
a,
Is
¸ıl
Özkoc
¸ak
Turan
daDepartmentofAnesthesiologyandReanimation,SchoolofMedicine,BulentEcevitUniversity,Zonguldak,Turkey bProvincialHealthDirectorateofSanliurfa,Sanliurfa,Turkey
cDepartmentofNeurology,SchoolofMedicine,BulentEcevitUniversity,Zonguldak,Turkey
dDepartmentofAnesthesiologyandReanimation,AnkaraNumunePracticeandResearchHospital,Ankara,Turkey
Received29May2014;accepted28October2014 Availableonline23May2015
KEYWORDS
Sugammadex; Neostigmine; Postoperative cognitive dysfunction; MMSE; MoCA
Abstract
Backgroundandobjective: Sugammadex is thefirst selective relaxant binding agent.When
comparedwithneostigmine,followingsugammadexadministrationpatientswakeearlierand
haveshorterrecoverytimes.Inthisstudy,wehypothesizedthatfastandclearawakeningin
patientsundergoinggeneralanesthesiahaspositiveeffectsoncognitivefunctionsintheearly
periodafteroperation.
Methods:Approved by the local ethical committee, 128 patients were enrolled in this
randomized,prospective,controlled,double-blindstudy.Patientswereallocatedtoeither
Sug-ammadexgroup(GroupS)ortheNeostigminegroup(GroupN).Theprimaryoutcomeofthestudy
wasearlypostoperativecognitiverecoveryasmeasuredbytheMontrealCognitiveAssessment
(MoCA)andMiniMentalStateExamination(MMSE).Afterbaselineassessment12---24hbefore
theoperation.Aftertheoperation,whentheModifiedAldreteRecoveryScorewas≥9theMMSE
and1hlatertheMoCAtestswererepeated.
Results:AlthoughtherewasareductioninMoCAandMMSEscoresinbothGroupSandGroupN
betweenpreoperativeandpostoperativescores,therewasnostatisticallysignificantdifference
intheslopes(p>0.05).ThetimetoreachTOF0.9was2.19mininGroupSand6.47mininGroup
N(p<0.0001).Recoverytimewas8.26mininGroupSand16.93mininGroupN(p<0.0001).
Conclusion:We showed that the surgical procedure and/or accompanying anesthetic
pro-cedure may cause atemporary orpermanent regression in cognitive function in theearly
∗Correspondingauthor.
E-mail:[email protected](Ö.Pis¸kin). http://dx.doi.org/10.1016/j.bjane.2014.10.003
postoperativeperiod.However,bettercognitiveperformancecouldnotbeprovedinthe
Sug-ammadexcomparedtotheNeostigmine.
©2015SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan
openaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Sugamadex; Neostigmina; Disfunc¸ãocognitiva nopós-operatório; MMSE;
MoCA
Oefeitodesugamadexsobreafunc¸ãocognitivaerecuperac¸ãonopós-operatório
Resumo
Justificativaeobjetivo: Sugamadexéoprimeiroagente deligac¸ãorelaxante seletivo.Após
aadministrac¸ãodesugamadex,ostemposdedespertarederecuperac¸ãodospacientessão
menores, emcomparac¸ãocomneostigmina. Nesteestudo,ahipótese foi queum despertar
maisrápidoeclarodospacientessubmetidosàanestesiageralpossuiefeitospositivossobreas
func¸õescognitivasnopós-operatórioimediato.
Métodos: Apósaaprovac¸ãodoComitêdeÉticalocal,128pacientesforamincluídosnesteestudo
prospectivo,randômico,controladoeduplo-cego.Ospacientesforamdesignadosparaogrupo
sugamadex(Grupo S)ougruponeostigmina(GrupoN). Odesfechoprimáriodoestudofoi a
recuperac¸ãocognitivanopós-operatórioimediato,deacordocomamensurac¸ãodaAvaliac¸ão
deMontrealdaFunc¸ãoCognitiva(MoCA)ecomoMiniExamedoEstadoMental(MMSE).Apósa
avaliac¸ãoinicial12---24hantesdaoperac¸ão.Apósaoperac¸ão,quandooescoredeRecuperac¸ão
deAldretemodificadoera≥9,otesteMMSEe,umahoradepois,otesteMoCAforamrepetidos.
Resultados: Emboratenhahavidoumareduc¸ãonosescoresdeMoCAeMMSEtanto noGrupo
Squanto noGrupo N,entreosescorespré-epós-operatório,não houvediferenc¸a
estatisti-camentesignificativanasreduc¸ões(p>0,05).OtempoparaatingirTOF0.9foide2,19minno
Grupo Sede6,47minnoGrupo N(p<0,0001).Otempode recuperac¸ãofoide 8,26min no
GrupoSede16,93minnoGrupoN(p<0,0001)
Conclusão:Mostramosqueoprocedimentocirúrgicoe/ouprocedimentoanestésicode
acom-panhamentopode causaruma regressãotemporária ou permanentedafunc¸ãocognitiva no
pós-operatórioimediato.Noentanto,umdesempenhocognitivomelhornãopodeserprovado
nogruposugamadexemcomparac¸ãocomogruponeostigmina.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum
artigo OpenAccess sobumalicenc¸aCCBY-NC-ND(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Patientswhoundergomajorsurgerywithgeneral anesthe-sia mayexperiencememoryimpairmentandregressionof high-executive functions such as ordering, planning, and organization after the operation.1 This intellectual and cognitiveworseningisknownaspostoperativecognitive dys-function (POCD).POCDoften creates temporary cognitive impairmentbut,especiallyinolderpatients,itmaytakethe formofpermanentdecline.1Todate,controlledstudiesand animal modelshave notestablisheddiagnosticcriteriafor POCD,anditsetiologyisnotfullyunderstood.2---4However, animal studies have provided strong evidence that expo-suretoanestheticagentsmaycausepermanentlearningand memoryimpairment.5---8
Sugammadex(Bridion®,MerckSharpandDohme (MSD),
Oss, The Netherlands) is a rapid andselectively effective aminosteroidagentthathasrecentlyentereduse.Through rocuroniumandvecuroniumencapsulation,itcauses rapid recovery independent of the time of administration.9---13 Comparedtopatientsgivenneostigminetorecover,patients givensugammadex have been observed torecoverwith a clearerlevelofconsciousness.
Inthisstudy,wehypothesizedthatfastandclear awak-eninginpatientsundergoinggeneralanesthesiahaspositive effects on cognitive functions in the early period after operation.Totest thishypothesis,postoperativecognitive functionsofpatientswereevaluated,comparingthosegiven neostigmineorsugammadexforrevivalaftergeneral anes-thesiawithrocuronium-basedneuromuscularblock.
Method
This randomized, prospective, controlled, double-blind study wasapproved by the BülentEcevit University Prac-ticeandResearchHospital EthicsCommittee(2012/07-7). Thestudyincludedpatientswithplannedoperationsunder general anesthesia (abdominal surgery; upper extremity orthopedicinterventions;gynecology;plasticsurgery; urol-ogy;ear, nose, and throat; and spinal surgery operations lastingatleast 60min) whocouldread andwriteTurkish, werebetween 18 and60 yearsof age, andhad American SocietyofAnesthesiologists(ASA)scoresofIorII.
diabetes mellitus (DM), neuropsychiatric disease, chronic alcoholor drugaddiction,GlasgowComa Scale (GCS)<15, historyofcardiopulmonaryarrestorstrokeintheprevious 12months,historyofpreviousoperationundergeneral anes-thesia, emergencysurgery, andpostoperative Mini-Mental StateExamination14 (MMSE)score<23andMontreal Cogni-tiveAssessment15(MoCA)score<21.
After receiving informed patient consent, the sugam-madex(Group S) and neostigmine(Group N)groups were createdusingtheclosed-envelopemethod.Toevaluate cog-nitive functions, the MMSE and MoCA tests were carried outbythesameneurologyexpert blindedtothepatient’s groupassignment.Allpatientswerevisited12---24hbefore theoperation.Thepatients’educationallevel, accompany-ingdiseases,anddemographicinformationwererecorded. Beforetheoperationthepatients’memory,attentive exec-utive functions, andmotor skills wereevaluatedwiththe MMSE and MoCA tests as a control cognitive evaluation (T0).Aftertheoperation,in thePACU,whenthe Modified
AldreteRecovery Score16 (MAS)was ≥9 theMMSE and 1h later the MoCA tests were repeated (T1). Neither group
wasgivenpremedication.Duringtheoperationmean arte-rial pressure (MAP), heart rate (HR), peripheral oxygen saturation(SpO2),bispectralindex(BIS),andadductor
mus-cleand nasopharyngeal temperature were monitored and recorded.Forneuromusculartransmissionmonitoringa TOF-WATCH® SX(OrganonTeknikaBV,Netherlands)devicewas
used.The temperature of the operatingroom was set to 21---25◦C.Thepatientswerecovered,andtheskin temper-atureofthe thenarregionwasmonitoredtoensureitdid not fall below 32◦C. All patients were given intravenous (IV)fentanyl(1g/kg)andpropofol(2mg/kg)foranesthesia induction. When BIS values were 40---60, TOF device cali-brationwascompletedandthreeconsecutivesingletwitch controlvalueswere recorded.Then, IV0.5mg/kg rocuro-nium wasadministered and the interval until TOF values reached0(TOF0)wasrecorded.WhenTOF0wasreachedthe
patientswereintubated.Tomaintainanesthesiaallpatients were given 50:50 O2/N2O and 2% sevoflurane titrated to
maintainBIS valuesbetween 40 and 60. Duringthe oper-ation,when TOF values were 25% (TOF25), a dose of one
quarteroftheinitialdoseofrocuroniumwasadministered. Attheendoftheoperation,whenTOF25wasreached,Group
SwasgivenIV2mg/kgsugammadexandGroupNwasgiven IV0.03mg/kg neostigmine+0.01mg/kg atropine. Patients wereextubatedwhentheirTOFvaluesreached90%(TOF90).
TheintervalbetweenTOF25 andTOF90wasrecordedin
sec-onds(TOF25---90).Duringtheoperation,amountsofadditional
medicationandtotalrocuroniumwererecorded.Afterskin suturingwasfinished,anestheticgaseswerestoppedinboth groups. This timewasrecorded astheend of anesthesia. The time fromwhen anesthetic gases were stoppeduntil MAS≥9wasrecordedastherecoveryperiod.Afterthe oper-ation,patientsweretransferred tothePACU.Allpatients weregivenIV1mg/kgtramadolaftertheskinincisionwas finishedfor postoperative pain relief. At 20, 40, 60, and 120min post-operation, visual analog scores17 (VAS) were recorded. When VAS>4 a non-steroidal anti-inflammatory analgesicagentwasadministeredandrecorded.
The primary outcome of the study was early postop-erativecognitive recovery as measured by the MoCA and MMSE.The secondary outcomewastimefromthe startof
thereversaladministrationtotherecoveryofaratioof0.9 in patients receiving rocuronium as NMBA during general anesthesiaforasurgicalprocedure.
Poweranalysis
To test the significance of differences between repeated measuresindependentgroupstheconventionaleffectsize requiredforthettestisassumedtobemedium(d=0.50), sofor thestudytohave80%power itwascalculatedthat bothgroupsneededaminimumsamplesizeof128(n=64).18
Statisticalanalysis
Statistical analyses for this study were completed using the SPSS for Windows 15.0 softwarepackage. Descriptive statistics were used (mean, median, standard deviation, minimumandmaximumvalues)toevaluatedata. Measure-ment values aregiven asmeans and standard deviations. Categoricalvariables(numbervalues)aregivenasnumbers and percentages. The chi-square test was used to com-pare categorical variables.The Levene’s test wasusedto evaluatethehomogeneitywithingroupsforparametric con-ditions.Iftheresultsofthehomogeneitytestsshowedthat parametric conditions were met, mixed ANOVA was used for comparisons between groups; ifparametric conditions were notmet,the Wilcoxon signed-ranktest wasusedto compare measurement values before and after, and the Mann---WhitneyUtestwasusedforcomparisonsof indepen-dentgroups.Significancewasacceptedatp<0.05.
Results
This study was conducted from September 2012 to July 2013with128patients.Thirty-eightpatientswereexcluded becausetheirMMSEandMoCAtargetscoreswerelow,and threewereexcludedbecausetheycouldnotbeextubated attheendoftheoperation.Ofthe87patientsincludedin thestudy,48.2%(n=42)wereinGroupSand51.8%(n=45) wereinGroupN.
Thedemographiccharacteristicsofthepatientsare pre-sentedinTable1.Thetotalamountofrocuroniumconsumed was 67.02±15.85mg in Group S and 62.44±11.65mg in Group N (Table 1). There was a statistically significant difference in average age between the groups (p<0.05). Therewerenosignificantdifferencesbetweenthegroupsin weight,BMI,durationofoperation,durationofanesthesia, andtotalamountofrocuroniumconsumed(p>0.05).
ThetimetoreachTOF0.9was2.19min inGroup Sand 6.47mininGroupN(p<0.0001).Recoverytimewas8.26min inGroupSand16.93mininGroupN(p<0.0001)(Table2).
TheMMSET0andT1scoresinGroupSwere26.98±1.957
and26.90±1.936,andinGroupNwere27.00±2.286and 25.82±2.724, respectively. The MoCAT0 andT1 scores in
GroupSwere23.26±1.988and23.17±2.294andinGroupN were23.56±2.482and23.04±2.868,respectively.Inboth tests the T1 mean was lower than the T0 mean.
Depen-dent groupswerecomparedwiththet-test,andrepeated measurementvalueswerecompared.Todeterminethe dif-ference between the MMSE and MoCA at T0 and T1, the
Table1 Distributionofsociodemograficfactorsandoperativedetailsviagroups.
GroupS(±SD)
(n=42)
GroupN(±SD)
(n=45)
pa
Meanage,years 32.07±11.50 37.38±11.95 <0.05
Gender(F/M) 12/30 22/23 >0.05
Educationyears(<9years/9---12years/>12years) 12/18/12 17/18/10 >0.05 Weight,kg 74.83±14.93 75.33±13.92 >0.05 BMI,kg/cm2 25.25±4.08 26.70±4.63 >0.05
ASAclass(I/II) 17/25 18/27 >0.05
Durationoftheoperation,min 118.86±42.94 115.49±46.51 >0.05 Durationoftheanesthesiology,min 125.21±38.91 124.18±48.39 >0.05 Rocuronium,mg 67.02±15.85 62.44±11.65 >0.05 Tramadol,mg 74.83±14.93 75.33±13.92 >0.05
F,Female;M,Male;BMI,bodymassindex;ASA,AmericanSocietyofAnesthesiologistscore.
a Chi-squaretest(2×n)andIndependentsamplettest.
Table2 TimetorecoveryofTOFratioto0.9(min)andtımetorecoveryofAldrete≥9(min).
GroupS(±SD) GroupN(±SD) pa
TimetorecoveryofTOFratioto0.9 2.19±1.47 6.47±1.92 <0.0001 TimetorecoveryofAldrete≥9 8.26±5.02 16.93±8.00 <0.0001
TOF,trainoffour.
a Independentttestforgroups.
Thetest resultsareillustrated inFig.1,whichshows that althoughtheT0andT1MMSEvaluesinGroupSwerereduced,
theslopeofthereductiondidnotshowastatistically signif-icantdifference(p>0.05).InGroup N,althoughtherewas astatisticallysignificant fallinMMSEvaluesfromT0 toT1
(p<0.05) there was no statistically significant difference between the slope values. Fig. 2 indicates that although therewasareductioninMoCAvaluesinbothGroupsSand
27
26.8
26.6
26.4
26.2
26
25.8
Groups
Estimated marginal means
Group S Group N
T0 T1
Figure1 MMSEscoreslopesofthegroupsfromT0toT1.
NfromT0toT1,therewasnostatisticallysignificant
differ-enceintheslopes(p>0.05)(Table3;Fig.3).
Discussion
In this study, the effects of sugammadex on recovery and cognitive functions were compared with those of
23 23.1 23.2 23.3 23.4 23.5 23.6
Groups
Estimated marginal means
Group S Group N
T0 T1
Table3 MMSEandMoCAscoresatpreoperativeand
post-operativeperiod.
T0(±SD) T1(±SD) pa
GroupS
MMSE 26.98±1.957 26.90±1.936 >0.05 MoCA 23.26±1.988 23.17±2.294 >0.05
GroupN
MMSE 27.00±2.286 25.82±2.724 <0.05 MoCA 23.56±2.482 23.04±2.868 >0.05
T0,preoperative;T1,postoperative. aPairedsamplettest.
neostigmine.AlthoughthesugammadexgroupreachedTOF 0.9 earlier than the neostigmine group and had shorter recovery times, no significant improvement in cognitive recoverywasidentified.
Surgical procedures and accompanying anesthetic pro-ceduresmaycausetemporaryor permanentpostoperative regression in cognitive functions; this situation is known as POCD.4 However, whether the surgical procedure or anesthesia administration causes POCD is not fully understood.2,3,19,20Manyrandomizedcontrolledstudieshave shown that the incidence of POCD increases in patients whoare older or undergoing cardiopulmonary bypassand lowerextremityorthopedicoperations.20 Todeterminethe effectof sugammadexandneostigmineoncognitive func-tion,thisstudyexcludedpatientsabovetheageof60years andthoseundergoingcardiac, cranial,and lower extrem-ity operations. Independent risk factors for development ofPOCD wereeliminated.In addition,therewasa signif-icant difference in average age between the two groups (GroupS:32.07±11.50andGroupN:37.38±11.95). John-sonetal.21foundthattheincidenceofPOCDwasverylow inmiddle-agedindividualsand determinedthattherewas nosignificantdifferenceinPOCDbetweenpatientswhohad undergoneanoperationintheprevious3monthsandhealthy volunteers. Therefore, we believe that the difference in
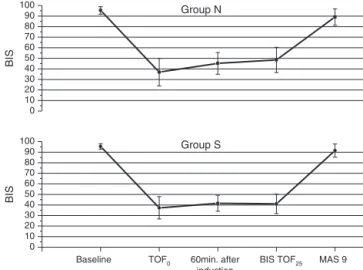
0 10 20 30 40 50 60 70 80 90
100 Group S
BIS
Baseline TOF0 60min. after
induction
BIS TOF25 MAS 9
0 10 20 30 40 50 60 70 80 90
100 Group N
BIS
Figure3 B˙IS valuesin group N and group S patients. B˙IS, Bispectral ˙Index.
agebetween thetwogroups didnotnegativelyaffect the cognitivetestscores.
There is no international consensus on how cognitive function shouldbeevaluatedafteran operation.22 To this end,almost30testshavebeendescribed,buttheir advan-tages have not been demonstrated. The MMSE test is frequentlyusedtoevaluatecognitivefunction after anes-thesiabecauseittakesashortertimetoadminister,andhas been found tobemoreuseful by patientsand physicians. TheMoCAtesthasbecomepopularrecentlyandisused fre-quentlyasitisnotdependentondemographicvariablessuch asageandeducation.23BoththeMMSEandMoCAtestshave high validityand reliability,withTurkish validityand reli-abilitystudies havingbeencompleted.23,24 Basedonthese factors, the MMSE andMoCA tests were usedto evaluate cognitivefunctioninthisstudy.
Thereare somereservations about whenand how fre-quently cognitive evaluation tests should be performed after operations.2,3,20 Factors that may negatively affect the cognitive evaluation scores are painafter the opera-tion,disruptedsleep,andlearning/memorizingofthetests duetotheirfrequentrepetition.1Inthisstudy,toprevent the effects of these factors all patients had a VAS score <4 and MAS score ≥9 before postoperative evaluation. In addition,topreventmemorizingandlearningof the eval-uationtests,thetestswereonlyconductedonceafterthe operation.
It is not known exactly when brain function returns after general anesthesia. Studies have shown that cogni-tivefunctionsareaffectedbyseveralfactorsaftersurgical procedures with anesthesia.1---3,19 As rapid and short-term effective anesthetic agents are metabolized less by the body, theymaycauseless cognitivedysfunction.Matthew et al.,8 in astudy of 921 patients undergoing major non-cardiac surgery, administered to one group a standard anesthetic protocol while theother group receiveda BIS-guided titrated anestheticprotocol. The BIS-guided group wasexposedlesstoanestheticagentsandwasdetermined tohavelessPOCDinthe3monthsaftersurgery.Thisstudy usedBISinboth groupstoreduceexposure toanesthetics andformonitoring.
TOF1.0in8.5min.Inourstudy,thetimetoreachTOF0.9 forpatientsgivensugammadexwas2.19min,andthe recov-erytimewas8.26min,whileforpatientsgivenneostigmine thesetimeswere6.47and16.93min.Thepatientsgiven sug-ammadexwokeandrecoveredearlierthandidthosegiven neostigmine.
Manystudiesoftheeffectsoffastemergenceand recov-ery from anesthesia on postoperative cognitive function havebeenconducted.Broncoetal.27comparedtheeffects ofarapid-startandrecoveryinhalationagent,xenon,with another inhalation agent, sevoflurane, in terms of post-operative recoveryand cognitivefunction.Patientsin the xenongrouphadanearlieremergencetimeandbetter cog-nitive recovery. Coburn et al.28 compared the effects of xenonwithdesfluraneonpostoperativecognitive function in elderly patients; the eye-opening and extubation peri-odswereshorterinthexenongroup;however,theauthors stated that the effects on cognitive function were simi-lar to those of desflurane. Similarly, Rasmussen et al.29 determined that the effects on cognitive function of the fast-acting inhalation agent xenon and fast-acting intra-venous propofol were similar in elderly patients. In our study, to evaluate the cognitive function in both groups, MMSE and MoCA tests were administered at T0 and T1.
AlthoughtherewasanumericalreductioninMMSEandMoCA scoresatT1comparedtoT0,therewasnostatistically
sig-nificant difference in the reduction slopes. Studies have shown that the surgical procedure and/or accompanying anestheticproceduremaycauseatemporaryorpermanent regressionin cognitivefunctionin theearly postoperative period. However,better cognitive performance could not be proved in the sugammadex patients compared to the neostigminepatients.Nopriorstudiescomparingthe cogni-tiveperformanceofsugammadexandneostigminepatients werefound.
Calculatingthesamplesizeforan80%strengthrequired eachgrouptoinclude64patients,foratotalof128; how-ever,exclusioncriteriameantthatthestudywascompleted with87patients.Limitationsintermsoftheprojectduration meantthatbackupgroupswerenotincluded.Thiswasthe most important limitation of thestudy. In addition, post-operative cognitiveevaluation wascompleted only during theearlyperiod.Asaresult,theeffectsofsugammadexon cognitivefunctionwerecomparedonlyintheearlyperiod. Anotherlimitationof thestudy wasthatlowdosesof sug-ammadex (2mg/kg) were used.As a result,the effectof high-dose(16mg/kg)sugammadexonPOCDdevelopmentis unknown.
In conclusion, evaluating cognitive function after an operation is complicated; the many independent risk factorsandmultitude ofevaluation testsaddtothe diffi-culty.
Sugammadexis a verynewagent.Further studies that includemoredetailedstatisticalanalysis,differentdosesof sugammadex, andlarger sample sizes areneeded tofully understandtheeffectsofthisagentoncognitivefunctionin thelatepostoperativeperiod.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FunderKS,SteinmetzJ,RasmussenLS.Methodologicalissuesof postoperativecognitivedysfunction.SeminCardiothoracicVasc Anesth.2010;14:119---22.
2.SauerAM,KalkmanC,DijkDV.Postoperativecognitivedecline. JAnesth.2009;23:256---9.
3.XuT,BoL,WangJ,etal.Riskfactorsforearlypostoperative cog-nitivedysfunctionafternon-coronarybypasssurgeryinChinese population.JCardiothoracSurg.2013;8:204.
4.Ologunde R,MaD.Doinhalationanestheticscausecognitive dysfunction?ActaAnaesthesiolTaiwan.2011;49:149---53. 5.CulleyDJ,BaxterM,YukhananovR,etal.Thememoryeffects
ofgeneralanesthesiapersistforweeksinyoungandagedrats. AnesthAnalg.2003;96:1004---9.
6.BianchiSL, Tran T, LiuC,et al. Brainand behavior changes in12-month-old Tg2576and nontransgenic miceexposedto anesthetics.NeurobiolAging.2008;29:1002---10.
7.WanY,XuJ,MaD,etal.Postoperativeimpairmentofcognitive functioninrats:apossibleroleforcytokine-mediated inflama-tioninthehippocampus.Anesthesiology.2007;106:436---43. 8.Chan MT, Cheng BC, Lee TM, et al. B˙IS-guided anesthesia
decreasespostoperativedeliriumandcognitivedecline.J Neu-rosurgAnesthesiol.2013;25:33---42.
9.BomA,BradleyM,CameronK,etal.Anovelconceptof revers-ingneuromuscularblock:chemicalencapsulationofrocuronium bromidebyacyclodextrin-basedsynthetichost.AngewChem IntEdEngl.2002;4:266---70.
10.StaalsLM,DreissenJJ,VanEgmondJ,etal.Train-of-fourratio recovery oftenprecedes twitchrecovery when neuromuscu-larblockisreversedbySugammadex.ActaAnaesthesiolScand. 2011;55:700---7.
11.GelderG,NiskanenM,LauriliaP,etal.Arandomisedcontrolled trialcomparingsugammadexandneostigminatdiffirentdepths ofneuromuscularblokadeinpatientsundergoinglaparoscopic surgery.Anaesthesia.2012;67:991---8.
12.Jones RK, Caldwell JE, Brull SJ, et al. Reversal of pro-found rocuronium-induced blockade with Sugammadex: a randomized comparison with neostigmine. Anesthesiology. 2008;109:816---24.
13.Khuenl-BradyKS,WattwilM,VanackerBF,etal.Sugammadex providesfasterreversalofvecuronium-inducedneuromuscular blockadecomparedwithneostigmine:amulticenter, random-ized,controlledtrial.AnesthAnalg.2010;110:64---73.
14.FolsteinMF,FolsteinSE,McHughPR.‘Mini-mentalstate’.A prac-ticalmethodforgradingthecognitivestateofpatientforthe clinician.JPsychiatrRes.1975;12:189---98.
15.Montreal Cognitive Assessment test references. http:// mocatest.org/pdffiles/test/MoCA-Test-English71.pdf (last available:06.01.14).
16.AldreteJA,KroulikD.Apost-anestheticrecoveyscore.Anesth Analg.1970;49:924---33.
17.AitkenRC.Measurementoffeelingusingvisualanalogueskales. ProcRSocMed.1969;62:989---93.
18.PortneyLG,WatkinsMP.Foundationsofclinicalresearch appli-cationstopractice.3rded.UpperSaddleRiver,NJ;2009.p. 653---60.
19.MollerJT,CluitmansP,RasmussenLS,etal.Long-term postoper-ativecognitivedysfunctionintheelderlyISPOCD1study.ISPOCD investigators.InternationalStudyofPost-OperativeCognitive Dysfunction.Lancet.1998;351:857---61.
20.Newman S, Stygall J, Hirani S, et al. Postoperative cogni-tive dysfunction after non cardiac surgery. Anesthesiology. 2007;106:572---90.
22.Steinmetz J, Siersma V, Kessing LV, et al. ˙Is postoperative cognitive dysfunction a risc factor for dementia. A cohort follow-upstudy.BrJAnaesth.2013;110:92---7.
23.SeleklerK,CangözB,Uluc¸S.Montrealbilis¸selde˘gerlendirme ölc¸e˘gi (MOB˙ID)’in hafif bilis¸selbozukluk ve Alzheimer hasta-larını ayırt edebilme gücünün incelenmesi. Turk J Geriatr. 2010;13:166---71.
24.Güngen C, Ertan T, Eker E, et al. Standardize mini mental test’in Türk toplumunda hafif demans tanısında gec¸erlilik ve güvenirli˘gi. Turk Psikiyatri Derg. 2002;13: 273---81.
25.Koc F, Turan G, Subası D, et al. Comparison of sugam-madexandneostigmininshorttermsurgery.1694,http://dx. doi.org/10.4328/JCAM.
26.Pongrácz A, Szatmári S, Nemes R, et al. Reversal of neu-romuscular blockadewith Sugammadexat thereappearance offour twitchesto train-of-fourstimulation. Anesthesiology. 2013;119:36---42.
27.BroncoA, ˙Ingelmo PB, ApriglianoM, et al. Xenon anaesthe-siaproducesbeterearlypostoperativecognitiverecoverythan sevofluraneanaesthesia.EurJAnaesthesiol.2010;10:912---6. 28.Coburn M, Baumert JH, Roertgen D, et al. Emergence and
earlycognitivefunctionintheelderlyafterxenonordesflurane anaesthesia:adouble-blindedrandomizedcontrolledtrial.BrJ Anaesth.2007;98:756---62.