REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
The
effect
of
intra-articular
levobupivacaine
on
shoulder
cartilage
at
different
doses----experimental
study
Mustafa
Soner
Özcan
a,
Mahmut
Kalem
b,
Meneks
¸e
Özc
¸elik
c,
Ercan
¸ahin
S
d,∗,
Sanem
C
¸akar
c,
Nazlı
Hayırlı
e,
Oya
Evirgen
c,
Feyhan
Ökten
caOccupationalDiseasesHospital,DepartmentofAnesthesiologyandReanimation,Ankara,Turkey bAnkaraUniversity,FacultyofMedicine,DepartmentofOrthopedics&Traumatology,Ankara,Turkey cAnkaraUniversity,FacultyofMedicine,DepartmentofAnesthesiologyandReanimation,Ankara,Turkey dBülentEcevitUniversity,FacultyofMedicine,DepartmentofOrthopedics&Traumatology,Zonguldak,Turkey eAnkaraUniversity,FacultyofMedicine,DepartmentofHistologyandEmbriology,Ankara,Turkey
Received26May2015;accepted17August2015 Availableonline20April2016
KEYWORDS
Glenohumeraljoint;
Chondrolysis; Levobupivacaine
Abstract
Backgroundandobjectives: Inthisstudyitwasaimedtoexaminethehistologicaland morpho-metriceffectsoncartilagestructureofintra-articularapplicationoflevobupivacainetothe shoulderjoint.
Methods:IntwentyNewZealandadultmalerabbits,35shoulderswereusedforthestudyand preparedin5groupsof7.ThesegroupsweredefinedasGroupsL1,L2,L3andL4whichwere rightshouldersadministered with0.25%and0.5%levobupivacaine,Group Cwhichwere left shouldersasthecontrolgroupandGroupsS1andS2whichwereleftshouldersadministered with0.9%saline.Onthe2ndand15thdaystheanimalswerekilled,theglenohumeraljoints wereevaluatedmacroscopicallythencartilagesamplesweretaken.Thesesampleswere evalu-atedwithMankinscore,andhistomorphometricallybymeasuringthethicknessofthecartilage betweenthesuperficialcartilagelayerandthetidemarkandthethicknessofcalcifiedcartilage betweenthetidemarkandthesubchondralbone.
Results:Macroscopically,onthe15thdaythejointfluidwasseentohavereducedinallthe groups.Aftermicroscopicevaluation,thehighestMankinscore(mean:3.14±2.1/14)wasinthe L4group(15thday0.5%levobupivacaine)andwasfoundtobestatisticallysignificant(p<0.05). Nostatisticallysignificantdifferencewasdeterminedbetweentheothergroups.
∗Correspondingauthor.
E-mail:[email protected](E.S¸ahin). http://dx.doi.org/10.1016/j.bjane.2015.08.008
Conclusions: Histologically,asthehighestMankinscorewasintheL4group,thisindicatesthat inasingleintra-articularinjectionoflevobupivacainealowconcentrationshouldbeselected. Levelofevidence: Level5,animalstudy.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Articulac¸ão glenoumeral; Condrólise; Levobupivacaína
Oefeitodelevobupivacaínaintra-articularnacartilagemdoombroemdoses diferentes----estudoexperimental
Resumo
Justificativaeobjetivo: Nesteestudooobjetivo foiexaminarosefeitos histológicose mor-fométricossobreaestruturadacartilagemdaaplicac¸ãointra-articulardelevobupivacaínaem articulac¸ãodoombro.
Métodos: Trintaecincoombrosde20coelhosNewZealand,machoseadultos,foramusados paraoestudoedivididosemcincogruposdesete.OsgruposforamdefinidoscomoL1,L2,L3e L4,consistindoemombrosdireitosnosquaislevobupivacaínaa0,25%e0,5%foiadministrada;o GrupoC,consistindoemombrosesquerdosfoiogrupocontrole;gruposS1eS2,consistindoem ombrosesquerdosreceberamsoluc¸ãosalinaa0,9%.Osanimaisforamsacrificadosnosegundoe nodécimoquintodia;asarticulac¸õesglenoumeraisforamavaliadasmacroscopicamentee,em seguida,amostrasdecartilagemforamcoletadas.Asamostrasforamavaliadascomoescore deMankine,histomorfometricamente,medindo-seaespessuradacartilagementreacamada superficialea‘‘linha demaré’’ (tidemark)e aespessuradacartilagemcalcificadaentrea tidemarkeoossosubcondral.
Resultados: Macroscopicamente, observou-se no décimo quinto dia que o líquido articular haviareduzidoemtodososgrupos.Apósaavaliac¸ãomicroscópica,omaiorescoredeMankin (média:3,14±2,1/14)foiobservadonogrupoL4(15◦dialevobupivacainaa0,5%),considerado
estatisticamentesignificativo(p<0,05).Nenhumadiferenc¸aestatisticamentesignificativafoi determinadaentreosoutrosgrupos.
Conclusões: Histologicamente,comoomaiorescoredeMankinfoiobservadonoGrupoL4,isso indicaqueemumaúnicainjec¸ãointra-articulardelevobupivacaína,umaconcentrac¸ãobaixa deveserselecionada.
Níveldeevidência:Nível5,estudoemanimais.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Despite better current understanding of pain mechanisms andrecordeddevelopmentsintreatment,cliniciansremain inadequateinthemanagementofpostoperativepain con-troland themajority of patients have complaintsof pain followingsurgery.1Insufficientpaintreatmentisoneofthe
elementsaffectingtherecoveryprocessofthepatientand byextendingthehospitalstay,hasanegativeeffecton mor-bidityandmortalityrates.The mostimportantaimin the treatmentofpostoperativepainistoprovideeffective anal-gesia without causing anyserious sideeffects. Therefore, toavoid side effects of high dosesof morphine, which is thegoldstandard,pre-emptiveanalgesia,peripheralnerve blocks, wound site infiltration and multimodal analgesia programmes have been developed. In this context, intra-articularinjectionsareoneofthemostpopulartechniques. The use of local anaesthetic by intra-articular sin-gle injection or continuous infusion are widely used pain
managementmethodsinshoulderandkneejointsurgery.2,3
They are used to obtain both perioperative analgesia and local and regional anaesthesia.4---7 The local
anaes-thetic which is most frequently used intra-articularly is bupivacaine.8 The injection of different doses of
intra-articularbupivacainehasbeenshowntobeaneffectivelocal anaestheticagent in intraoperative anaesthesiaand post-operativeanalgesia.4,9---12However,ininvitrostudies,there
hasbeen reportedtobe a chondrotoxiceffect of bupiva-caineassociatedwithdoseandtimeandthishasbeenthe reasonforitslimiteduse.13---17
Inpreviousvoluntaryhumantrials,levobupivacainehas been shown tobeaseffective asbupivacaine providinga longerandstrong analgesic effectandwithlowercardiac andcentralnervoussystemtoxicity.18---21However,thereare
alimitednumberofstudiesshowingtheintra-articularuse oflevobupivacaineinshoulderandkneearthroscopy.22---24
theintra-articular applicationtotheshoulderjointof lev-obupivacaine.
Materials
and
methods
Approval for the study was granted by Local University AnimalExperimentsEthicsCommittee.Thestudywas con-ducted at Local University Morphology Campus Animal Laboratoryusing20NewZealandadultmalerabbits,aged 12---15monthsandwithameanweightof3kg. Usingboth shouldersof therabbits,35 shoulderswereprepared in5 groupsof7.Thegroupingwasmadeblindandafterthe pro-cedure, theears were labelledwith thegroup letterand number,thentheanimalswerehoused2toacage.Theright shoulders of the rabbits were defined as Group L receiv-ing0.25% and0.5% levobupivacaine, theleftshoulders as thecontrolgroup,GroupCandthosereceiving0.9%saline, GroupS.
Thelevobupivacaine andsalinegroupsweresubdivided onDay2(0.25%and0.5%levobupivacaineasGroupsL1and L2andGroupS1)andonDay15(0.25%and0.5% levobupi-vacaineasGroups L3andL4andGroup S2)for thetaking ofnecropsymaterial.Astherewasnopreviousdatatobe takenasareferencedefiningthecapsularvolumeofthe rab-bitglenohumeraljointorshowinghowandatwhatdosage levobupivacaineshouldbeadministeredtorabbits,the clin-icalandexperimentalstudiesofbupivacaineonrabbitswere takenintoconsiderationandtheamounttobeadministered wascalculatedas0.5mLfor3kg.15,25
Surgicalprocedure
After6hfasting,sedoanalgesiawasobtainedintherabbits throughintramuscularadministrationofxylazine hydrochlo-ride (5mg·kg−1) and ketamine hydrochloride (5mg
·kg−1).
After sterile preparation, the glenuhumeral joint was located by palpation. With a 38G insulin injector, firstly the jointspace wasconfirmed by aspirationof the intra-articularfluid, then the experimental agent wasinjected intothejointspace.Thepreviouslydefineddosesof0.25% levobupivacainewereadministeredtotherightshouldersof 10rabbitsand0.5%levobupivacainetotherightshouldersof theother10rabbits.Totheleftshouldersof10rabbits,0.9% NaClwasadministeredatthedefineddose.Therabbit shoul-derswerethen separatedinto7groups of5forthetaking ofnecropsymaterialat2and15daysaftertheprocedure.
Macroscopicanalysisandcartilagesampling
The rabbits were sacrificed on the 2nd or 15th day by intraperitoneal high dose anaesthetic agent (sodium thiopental150mg·kg−1) andtheglenohumeral jointswere
opened. After macroscopic evaluation of the surface and colourof theglenohumeral jointcartilage and amount of intra-articularsynovialfluid,cartilagesamplesweretaken fromthehumerusheadwitha4mmdiameter,sharp-ended trocar,which is usedfor cartilage transferin orthopaedic surgery(mosaicplasty).Thepurposeofusingthiswasnotto causeanyiatrogenicdamagetothecartilagefield.
Table1 Histologyhistopathologygradingsystem.
1.Structure
(A)Normal 0
(B)Surfaceirregularities 1 (C)Pannusandsurfaceirregularities 2 (D)Cleftstotransitionalzone 3 (E)Cleftstoradialzone 4 (F)Cleftstocalcifiedzone 5 (G)Completedisorganisation 6 2.Cells
(A)Normal 0
(B)Diffusehypercellularity 1
(C)Cloning 2
(D)Hypocellularity 3
3.Safranin-Ostaining
(A)Normal 0
(B)Slightreduction 1
(C)Moderatereduction 2
(D)Severereduction 3
(E)Nodyenoted 4
4.Tidemarkintegrity
(A)Intact 0
(B)Crossedbybloodvessels 1 Mankin HHGS scoreis thesum ofstructure, cells, Safranin-O stainingandtidemarkintegrity.
Histological
analysis
The samples of cartilage tissue taken were placed in
10% buffered formalin solution for examination by light
microscope. After 48h fixation in the solution,the tissue
samplesweredecalcifiedinacontrolleddecalcification
solu-tion prepared at the ratio of 1:1 of 8% formic acid and
8% hydrochloric acid solutions. Following the
decalcifica-tion process, tissue samples were dehydrated through a
graded series of ethanol and embedded in parafin. The
7m sectionstakenfromtheparaffinblockswerestained
withhaematoxylin---eosin(H&E)forroutineexaminationand
stainedwithGiemsaandGomori’ssinglestagetrichomefor
evaluation of the cartilage extracellular matrix. The
sec-tionswereanalysedandphotographedwithlightmicroscopy
(Leica DM 3000 photomicroscope) for histomorphological
structure.
Forhistomorphometric measurementsH---Estained
sec-tions from each animal were selected. Three fields were
chosen randomly on each section and by using an ocular
micrometre at 10× magnification, the cartilage thickness
between the superficial cartilage layer and the tidemark
and the calcified cartilage thickness between the
tide-markandthesubchondralboneweremeasured.Toachieve
standardisation, themeasurementsweretakenparallelto
the cartilage cell columns. In each section, the number
oftidemarkswasstated.Allsectionswereevaluatedby 2
experiencedhistologistsblindedtothegroupsaccordingto
thehistological/histochemicalgrading system (HHGS),the
Mankin’sScoringSystem,andthepointsoftheMankinscore
a
S
D M
S
CCZ
CCZ S
M
D M
D
CCZ
b
c
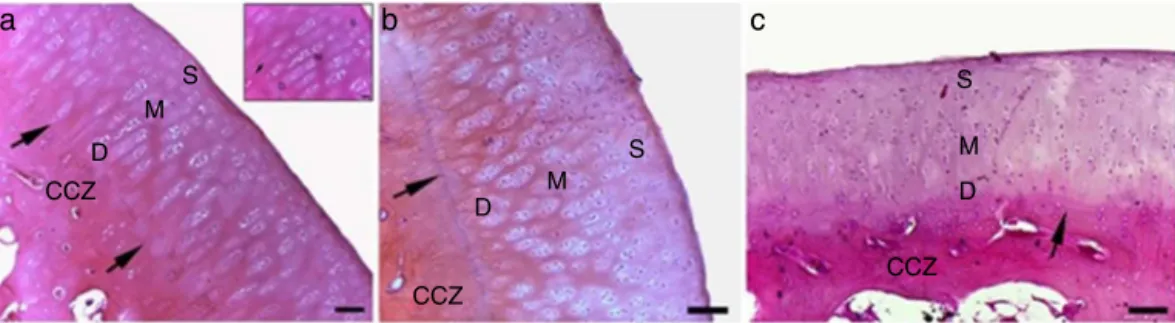
Figure1 Photomicrographofarticularcartilagefromthecontrol(a),S1(b)andS2(c)groups.S,superficialzone;M,middlezone; D,deepzone;CCZ,calcifiedcartilagezone;arrow,tidemark,H&E,10×obj.,bars:100m(inlet40×,bar:30m).
Statisticalanalysis
All the data were compared between the groups sepa-ratelyusingtheKruskal---Wallistest.Thecartilagethickness betweenthesuperficiallayerandthetidemarkandthe cal-cified cartilage thickness between the tidemark and the subchondralbonewerestatisticallyanalysedwiththeAnova test.Avalueofp<0.05wasacceptedasstatistically signif-icant.
Results
Macroscopicevaluation
The appearance of the glenohumeral joint exposed dur-ing the experiment wasexamined. Macroscopically,in all thegroups,thejointsurfacewasregularandnoabnormal colourchangeswereobserved.Theintra-articular synovial fluid wasclear in consistency but the amount wassmall. Whenthegroupswerecompared,theintra-articularfluidin theshouldersoftherabbitsonwhich15thdaynecroscopy wasapplied,was seen tohave reduced towhatcould be describedasnone.
Microscopicevaluation
In the control group (Group C) and the groups to which 0.5mL saline was administered intra-articularly (Groups S1---2), the appearance was normal in the cartilage cells andthestructureofthehyalincartilagesuperficial,middle
(transitional)anddeep(radial)layersandcalcifiedcartilage zoneintheexaminedjointcartilagesections.Thetidemark (thetransitarealine)wasobservedtobeuninterruptedand darkbasophilicstained(Fig.1A---C).
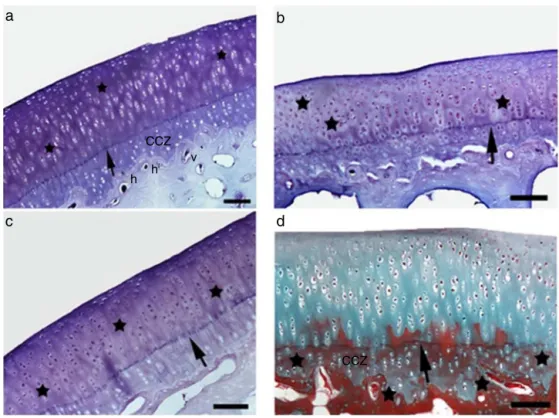
Inthegrouptowhich0.25%levobupivacainewas admin-isteredand2nddaynecropsywasapplied(GroupL1),mild irregularityonthecartilagesurface,anincreasednumberof tidemarksandchondrocytehypertrophyinthemiddlelayer wereobservedandinthegrouptowhich0.5% levobupiva-cainewas administered(Group L2), therewere scattered breaks in the tidemark and irregularity in the column of chondrocytesinthedeeplayer(Fig.2AandB).Anincrease wasseenintheMankinscoreofbothgroupscomparedtothe controlgroup.WhenthecharacteristicsstainedwithGiemsa wereexamined,therewasobservedtobeareductionin car-tilageextracellularmatrixstainingatbothdosescompared tothecontrolgroup.Inthetrichromestainedpreparates,in thegrouptowhich0.5%levobupivacainewasadministered (GroupL2) stainingwasshown in theextracellular matrix structureinthecalcifiedcartilagearea(Fig.3A---D).
Inthegrouptowhich0.25%levobupivacainewas admin-isteredand15thdaynecropsywasapplied(GroupL3),there wasirregularityonthecartilagesurfaceandhypocellularity andinthegrouptowhich0.5%levobupivacainewasapplied (GroupL4),therewasobservedtobeanincreaseinthe num-beroftidemarksandareductioninthenumberofcellsin themiddleanddeeplayers(Fig.4).Whenthecharacteristics wereexamined withGiemsaandtrichromestaining,there wasareductionincartilageextracellularmatrixstainingat bothdosescomparedtothecontrolgroupandfissureswere observedextending from thesurface asfar asthe transit
a
b
D
a
b
c
d
CCZ
CCZ h
v
h
Figure3 ExtracellularmatrixstainingofarticularcartilagefromtheC(a),L1(b),L2(candd)groups.(a)Arrow,tidemark;stars, normalstainingofextracellularmatrix;CCZ,calcifiedcartilagezone;h,haverscanal;v,valkmanncanal.(bandc)Stars,reduction incartilageextracellularmatrixstaining,Giemsa.(d)Stars,extracellularmatrixstructureinthecalcifiedcartilagearea,Gomori’s trichromestain,10×obj.,bars:100m.
a
S
M
D
CCZ
M S
D
b
Figure4 Photomicrographofarticularcartilagefrom theL3(a),L4(b)groups.S,superficialzone; M,middlezone;D, deep zone;CCZ,calcifiedcartilagezone;arrows,tidemark;stars,hypocellularity;thickarrow,surfaceirregularity,H&E,10×obj.,bars: 100m(inlet:multipletidemarks,40×obj.,bar:30m).
a
b
CCZ
CCZ
CCZ
BM
BM BM
c
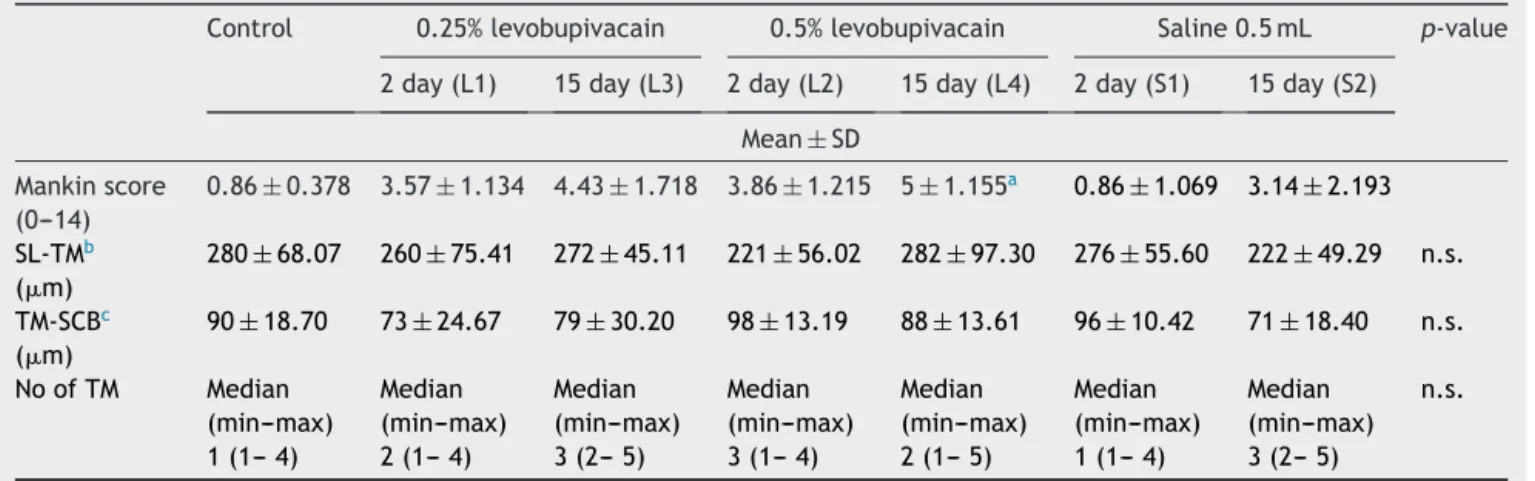
Table2 Histopathologicaldataandstatisticalanalysisofthegroups.
Control 0.25%levobupivacain 0.5%levobupivacain Saline0.5mL p-value 2day(L1) 15day(L3) 2day(L2) 15day(L4) 2day(S1) 15day(S2)
Mean±SD Mankinscore
(0---14)
0.86±0.378 3.57±1.134 4.43±1.718 3.86±1.215 5±1.155a 0.86±1.069 3.14±2.193
SL-TMb
(m)
280±68.07 260±75.41 272±45.11 221±56.02 282±97.30 276±55.60 222±49.29 n.s.
TM-SCBc
(m)
90±18.70 73±24.67 79±30.20 98±13.19 88±13.61 96±10.42 71±18.40 n.s.
NoofTM Median (min---max) 1(1---4)
Median (min---max) 2(1---4)
Median (min---max) 3(2---5)
Median (min---max) 3(1---4)
Median (min---max) 2(1---5)
Median (min---max) 1(1---4)
Median (min---max) 3(2---5)
n.s.
a ThehighestMankinscorewasseeninGroupL4(p<0.05).
b Cartilagethicknessbetweenthesuperficiallayer(SL)andthetidemark(TM).
c Calcifiedcartilagethicknessbetweenthetidemark(TM)andthesubchondralbone(SCB).
region.Inthetrichromestainedpreparates,inthegroupto which0.25% levobupivacainewasadministered(Group L3) there wasreduced staining in the extracellular matrix in thesurfacecartilageareaandhypocellularity.Inthegroup towhich0.5%levobupivacainewasadministered(GroupL4) stainingwasshownintheextracellularmatrixstructurein thecalcifiedcartilage area(Fig.5).An increasewasseen in the Mankinscore in both groups comparedto the con-trolgroupandthehighestscorewasseentobeinGroupL4 (p<0.05)(Figs.4and5)(Tables1and2).
TheMankinscorewashigherinGroupsL1,L2andL3than inthecontrolgroupandGroupS1andthiswasstatistically significant (p<0.05).The Mankinscore inGroup S1was a similarvaluetothatofthecontrolgroup.Inthehistological examinationinGroupS2,theMankinscorewasfoundtobe atastatisticallyhighvaluecomparedtothatofthecontrol group(p<0.05).
No statistically significant difference was determined betweenthegroupsinthecomparisonofthemeanvalues ofcartilagethicknessbetweenthesuperficiallayerandthe tidemarkandthecalcifiedcartilagethicknessbetweenthe tidemarkandthesubchondralbone(p>0.05).
Nostatisticallysignificantdifferencewasdeterminedin the comparison between the control and study groups in termsoftidemarknumbers(p>0.05).
Discussion
Although perioperative intra-articular local anaesthesia administrationisthoughttobesafe,inrecentyears,there have been many studies examining the effects of local anaesthetics on joint cartilage.13---17,25---29 Previous studies
have been oriented todrawtheattention of orthopedists andanesthesiologiststothepotentialdamagewhichcould occur in the joint cartilage from the intra-articular use of local anaesthesia either alone or with other medica-tionsandasasingleinjectionor asacontinuousinfusion. As a result of a review by Piper et al. of chondrotoxic-ity of local anaesthetics, it was reportedthat high doses
shouldbeavoidedandtheresultsofasingleintra-articular injectionwerenotclear andtherewasaneed forfurther studies.25
In a study by Baker et al., the 24h effect of in vitro differentdoses of bupivacaine, ropivacaineand levobupi-vacainewasexaminedinhumanchondrocytecultureandit wasreportedthatasignificantlyincreasedlevelof chondro-cytedamagewasseenathighdosesofthelocalanaesthetic groups. It wasreported that the chondrotoxic effect was dose-dependent.27Similarly,inastudybyGüngöretal.,
dif-ferentconcentrations of levobupivacaine andbupivacaine wereaddedtoratcartilagecellculturesandafter48hthe chondrotoxiceffectwasreportedtobedose-dependent.28In
thecurrentstudy,paralleltobothofthosepreviousstudies, itwasobservedthatingroupsadministeredwithdifferent concentrationsoflevobupivacaineasasingleintra-articular injection,at both the2ndandthe15thday, thecartilage wasaffected.
The Mankin score was significantly high in Group L4. Different from the previous studies, in Group L4, histo-logically there was seen to be the formation of fissures extendingtothe mid transitlayer,a hypocellular appear-ance, tidemark irregularity, a mild and moderate degree oflossofstainingin thecartilageextracellularmatrix. As therewasseentobegreaterdegenerationofthejoint car-tilage, it was thoughtthat the chondrotoxic effectcould continue over time. Taking into consideration that car-tilage damage may develop over time with the use of intra-articularlevobupivacaine,thisfindingshows alsothe necessityofusingalowdose.Insupportofthefindingsof our study, Molinos et al. have considered that the chon-drotoxiceffectoflevobupivacainewastime-dependent,so following total knee replacement surgery, samples taken fromhumancartilagewereexposedfor15,30and60minto 0.5%levobupivacaine,0.5%bupivacaineand0.5% physiolog-icalsalineincellcultures.Thegreatestchondrotoxiceffect asobservedtooccurafter1h associatedwithexposureto levobupivacaine.29
considered that diminished cartilage nutritiondue tothe fluiddilution maybe thetoxic effectsof levobupivacaine and this effect would become more evident in the late stage.Hyalincartilage, which covers thesurface of syno-vialjoints,isanavascularstructuredependentonsynovial fluidfor metabolicneeds.Any fluidadministeredintothe jointspacecanchangethecompositionofsynovialfluidor diluteitandthusinthissituationthejointcartilage nutri-tionis disrupted. As the knee jointcartilage is thickand theintra-articularcavityiswide,thereisalower possibil-ityofimpairednutritionofthejointcartilagewhichwould occur due to pressure and fluid dilution. Because of the anatomicalandhistologicalstructureof theshoulder joint andcartilage, it is thoughtthat it couldbe more greatly affected by a single intra-articular injection of high-dose localanaesthetic.
Asnostatisticallysignificantdifferencewasfoundinthe measurements of the cartilage layers compared to those ofthecontrol group,itcan bethoughtthattherewasno changerelatedtothecartilagelayerthickness.Thevalues weresimilartothosereportedinliteratureinstudiesrelated tothecalcifiedcartilagelayer.30
Althoughmainlimitationofourstudyisthatthechoosen animalmodel doesnot representtheclinical situation,as wedealwithinjuredordiseasedshoulders.
Inouranimalstudyithasbeenshownthat,asingle intra-articularinjectionoflevobupivacaine alowconcentration andlowamountoftotalintra-articularfluidshouldbe pre-ferredinconsiderationoflong-termchondrotoxiceffects.
Summary
Althoughfurtherstudiesmustbedoneforfinal recommen-dations,according toourstudy,clinicaluse ofsingledose intra-articular levobupivacaine should be choosen at low dosesforartroscopicshouldersurgery.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.RawalN.Postoperativepaintreatmentforambulatorysurgery. BestPractResClinAnaesthesiol.2007;21:129---48.
2.Zeidan A, Kassem R, Nahleh N, et al. Intraarticular tramadol---bupivacaine combination prolongs the duration of postoperative analgesia after outpatient arthroscopic knee surgery.AnesthAnalg.2008;107:292---9[Epub19.07.08]. 3.AxelssonK,GuptaA,JohanzonE,etal.Intraarticular
admin-istration of ketorolac, morphine, and ropivacaine combined with intraarticular patient-controlled regional analgesia for painreliefaftershouldersurgery:arandomized,double-blind study.AnesthAnalg.2008;106:328---33[Epub01.01.08]. 4.Moiniche S, Mikkelsen S, Wetterslev J, et al. A systematic
reviewofintra-articularlocalanesthesiaforpostoperativepain relief afterarthroscopic kneesurgery.Reg AnesthPain Med. 1999;24:430---7.
5.BanerjeeS,PulidoP,AdelsonWS,etal.Theefficacyof continu-ousbupivacaineinfiltrationfollowingarthroscopicrotatorcuff repair.Arthroscopy.2008;244:397---402.
6.Barber A, Herbert A. The effectiveness of an anesthetic continuous-infusion device on postoperative pain control. Arthroscopy.2002;18:76---81.
7.Parker D, Streem K, Schmitz L, et al. Efficacy of contin-uous intra-articular bupivacaine infusion for postoperative analgesia after anterior cruciate ligament reconstruction: a double-blinded,placebo-controlled,prospective,and random-izedstudy.AmJSportsMed.2007;354:531---6.
8.BallieulJ,JacobsF,HerregodsS,etal.Theperi-operativeuse ofintra-articularlocalanesthetics:areview.ActaAnaesthesiol Belg.2009;60:101---8.
9.TuncerB,BabacanA,ArslanM.Thepre-emptiveanalgesiceffect ofintra-articularbupivacaineinarthroscopickneesurgery.Acta AnaesthesiolScand.2005;49:1373---7.
10.MauerhanR, CampbellM,MillerS,et al.Intra-articular mor-phineand/orbupivacaineinthemanagementofpainaftertotal kneearthroplasty.JArthroplasty.1997;12:546---52.
11.Geutjens G, Hambidge E. Analgesic effects of intraartic-ular bupivacaine after day-case arthroscopy. Arthroscopy. 1994;10:299---300.
12.Heard O, Edwards T, Ferrari D, et al. Analgesic effect of intraarticularbupivacaineormorphineafterarthroscopicknee surgery:arandomized,prospective,double-blindstudy.Anesth Analg.1992;74:822---6.
13.ChuR,IzzoJ,PapasE,etal.Invitroexposureto0.5% bupiva-caineiscytotoxictobovinearticularchondrocytes.Arthroscopy. 2006;22:693---9.
14.DragooL,KorotkovaT,KanwarR,etal.Theeffectoflocal anes-theticsadministeredviapainpumponchondrocyteviability.Am JSportsMed.2008;36:1484---8.
15.GomollH,KangW,WilliamsJ,et al.Chondrolysisafter con-tinuousintra-articular bupivacaineinfusion: an experimental model investigating chondrotoxicity in the rabbit shoulder. Arthroscopy.2006;22:813---9.
16.HansenB,BeckC,BeckE,etal.Postarthroscopicglenohumeral chondrolysis.AmJSportsMed.2007;35:1628---34.
17.PiperS,KimH.Comparisonofropivacaineandbupivacaine tox-icityinhumanarticularchondrocytes.JBoneJointSurgAm. 2008;90:986---91.
18.FosterR,Markham A.Levobupivacaine:a reviewofits phar-macology and use as a local anaesthetic. Drugs. 2000;59: 551---79.
19.Gristwood R. Cardiac and CNS toxicity of levobupivacaine: strengthsofevidenceforadvantageoverbupivacaine.DrugSaf. 2002;25:153---63.
20.Mazoit X, Decaux A, Bouaziz H, et al. Comparative ven-tricular electrophysiologic effect of racemic bupivacaine, levobupivacaine,andropivacaineontheisolatedrabbitheart. Anesthesiology.2000;93:784---92.
21.BurlacuL,BuggyJ.Updateonlocalanesthetics:focuson lev-obupivacaine.TherClinRiskManag.2008;4:381---92.
22.Das A, Majumdar S, Kundu R, et al. Pain relief in day carearthroscopickneesurgery:a comparisonbetween intra-articular ropivacaine and levobupivacaine: a prospective, double-blinded,randomizedcontrolledstudy.SaudiJAnaesth. 2014;8:368---73.
23.Sahin SH,Memis¸D,CelikE, etal. Postarthroscopyanalgesia using intraarticular levobupivacaine and intravenous dexke-toprofen trometamol. Knee Surg Sports Traumatol Arthrosc. 2014.
24.ErdenA,AltinelS,SaricaogluF,etal.Effectofintra-articular injectionoflevobupivacaineonarticularcartilageandsynovium inrats.Anaesthesist.2012;61:420---3.
25.PiperL,KramerD,KimT,etal.Effectsoflocalanestheticson articularcartilage.AmJSportsMed.2011;39:2245---53. 26.DoganN,ErdemF,ErmanZ,etal.Theeffectsofbupivacaineand
27.BakerF,WalshM,ByrneP,etal.Invitroassessmentofhuman chondrocyteviabilityaftertreatmentwithlocalanaesthetic, magnesiumsulphateornormal saline.KneeSurgSports Trau-matolArthrosc.2011;19:1043---6.
28.GungorI,YilmazA,OzturkM,etal.Bupivacaineand levobupi-vacaineinduceapoptosis in ratchondrocyte cell cultures at ultra-lowdoses.EurJOrthopSurgTraumatol.2014;24:291---5.
29.MolinosJ, GarciaM, CorralesA, et al.Effect of levobupiva-caineonarticularchondrocytes:anin-vitroinvestigation.EurJ Anaesthesiol.2014.