www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Deep
neck
abscesses:
study
of
101
cases
夽
Thiago
Pires
Brito
∗,
Igor
Moreira
Hazboun,
Fernando
Laffitte
Fernandes,
Lucas
Ricci
Bento,
Carlos
Eduardo
Monteiro
Zappelini,
Carlos
Takahiro
Chone,
Agrício
Nubiato
Crespo
UniversidadeEstadualdeCampinas(UNICAMP),FaculdadedeCiênciasMédicas,DepartamentodeOtorrinolaringologia, Campinas,SP,Brazil
Received28October2015;accepted12April2016 Availableonline5May2016
KEYWORDS Neckabscess; Neckinfection; Neckspaces
Abstract
Introduction:AlthoughtheincidenceofDeepCervicalAbscess(DCA)hasdecreasedmainlyfor theavailabilityofantibiotics,thisinfectionstilloccurswithconsiderablefrequencyandcanbe associatedwithhighmorbidityandmortality.
Objective: This study aimed to present our clinical-surgical experience with deep neck abscesses.
Methods:A retrospectivestudy analyzed 101 patients diagnosed with deepneck abscesses causedbymultipleetiologies,assistedatamedicalschoolhospitalduring6years.One hun-dredonepatientswereincludedand27(26.7%)wereyoungerthan18yearsold(thechildren group),74patients(73.3%)wereolderthan18yearsold(theadultsgroup).Thefollowing clin-icalfeatureswereanalyzedandcompared:age,gender,clinicalsymptoms,leukocytecount, theaffectedcervicalarea,lifestylehabits,antibiotictherapy,comorbidities,etiology,bacterial culture,timeofhospitalization,theneedoftracheostomyandcomplications.
Results:There was predominanceinthemale gender(55.5%)andyoung people(meanage 28.1years).Allofthe51patientswithassociateddiseasecomorbiditywereadults.Themost frequentetiologieswerebacterialtonsillitis(31.68%)andodontogenicinfections(23.7%).The mostcommon cervicalareas affected were theperitonsillar (26.7%), submandibular/mouth floor (22.7%)andparapharyngealspaces (18.8%).Inchildren group,thesitemostcommonly involvedwas theperitonsillarspace(10patients, 37%).In adultsgroup,thesitemost com-monlyinvolvedwasmultispace(31patients,41.8%).Streptococcuspyogenes(23.3%)wasthe mostcommonmicroorganismpresent.Amoxicillinassociatedwithclavulanate(82.1%)wasthe
夽 Pleasecitethisarticleas:BritoTP,HazbounIM,FernandesFL,BentoLR,ZappeliniCE,ChoneCT,etal.Deepneckabscesses:studyof
101cases.BrazJOtorhinolaryngol.2017;83:341---8.
∗Correspondingauthor.
E-mail:[email protected](T.P.Brito).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.04.004
moreusedantibiotic.Themaincomplicationsofabscessesweresepticshock(16.8%), pneu-monia(10.8%)andmediastinitis(1.98%).Tracheostomywasnecessaryin16.8%ofpatients.The mortalityratewas1.98%.
Conclusion:TheclinicalfeaturesandseverityofDCAvariedaccordingtodifferentagegroups, perhapsduetothelocationoftheinfectionandahigherincidenceofcomorbidityinadults. Thus,DCAinadultsismorefaciletohavemultispaceinvolvementandleadtocomplications andseemstobemoreseriousthanthatinchildren.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Abscessocervical; Infecc¸ãocervical; Espac¸oscervicais
Abscessoscervicaisprofundos:estudode101casos
Resumo
Introduc¸ão:Emboraaincidênciadosabscessoscervicaisprofundos(ACP)tenhadiminuído prin-cipalmentepeladisponibilidadedosantibióticos,essainfecc¸ãoaindaocorrecomfrequência considerávelepodeserassociadaaaltamorbidadeemortalidade.
Objetivo:Esteestudotevecomoobjetivoapresentarnossaexperiênciaclínico-cirúrgicacom abcessoscervicaisprofundos.
Método: Um estudo retrospectivo realizado em um hospital universitário analisou 101 pacientes,duranteseisanos,diagnosticadoscomabscessoscervicaisprofundoscausadospor múltiplasetiologias.Foramincluídos101 pacientes,sendoque27 (26,7%)tinhammenos de 18 anos(grupo das crianc¸as) e74 (73,3%)tinhammais de 18 anos(grupo dos adultos).As seguintescaracterísticasclínicasforamanalisadasecomparadas:idade,sexo,sintomas clíni-cos, área cervicalacometida, hábitos de vida, antibioticoterapia, comorbidades, etiologia, culturabacteriana,tempodeinternac¸ão,necessidadedetraqueotomiaecomplicac¸ões.
Resultados: Houvepredominânciadosexomasculino(55,5%)edejovens(idademédiade28,1 anos). Todosos 51 pacientescom comorbidade associada eram adultos. Asetiologias mais frequentesforamtonsilite bacteriana(31,68%) einfecc¸ões odontogênicas (23,7%).As áreas cervicaisacometidas mais comunsforama peritonsilar (26,7%), submandibular/assoalhoda boca(22,7%)eespac¸osparafaríngeos(18,8%).Nogrupodascrianc¸as,olocalmaiscomumente envolvidofoioespac¸operitonsilar(10pacientes,37%).Nogrupodosadultos,houvepredomínio deacometimento demúltiplosespac¸os (31pacientes,41,8%).Streptococcus pyogenes foio microrganismo presente mais comum(23,3%). A amoxicilina associadaao clavulanatofoi o antibióticomaisusado(82,1%).Asprincipaiscomplicac¸õesdosabscessosforamchoqueséptico (16,8%),pneumonia(10,8%)emediastinite(1,98%).Atraqueostomiafoinecessáriaem16,8% dospacientes.Ataxademortalidadefoide1,98%.
Conclusão:AscaracterísticasclínicaseagravidadedoACPvariaramdeacordocomdiferentes faixasetárias,possivelmentedevidoàlocalizac¸ãodainfecc¸ãoeàmaiorincidênciade comor-bidadesem adultos. Assim, oACP em adultos acomete mais facilmente múltiplosespac¸os, apresentamaiscomplicac¸õeseparecesertambémmaisgravedoqueemcrianc¸as.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Deep cervical abscesses (DCA)is definedby the presence of pus in the spaces and fasciae of the head and neck. DCA can be categorized into retropharyngeal, peritonsil-lar, masseteric, pteropalatine maxillary, parapharyngeal, submandibular, parotid and floor of mouth abscesses.1 Despite the improvements in diagnostic tests and the availabilityof modernantibiotic therapy, thoseinfections continuetocausesignificantmorbidityandmortalityrates, especiallywhenthereisnoearlytreatment.2Itoccurswith
anti-inflammatory drugs may mask presentations. It is sometimes difficult to findthe origin of DCA because the primarysourceofinfectionmayprecedeitbyweeks.5
DCA are potentially fatal and require an aggressive diagnostic and therapeutic management to avoid life-threatening complications, such as airway obstruction, cervical necrotizing fasciitis, jugular vein thrombosis, disseminatedintravascular coagulationempyema, medias-tinitis, aspiration pneumonia or thrombosis/aneurysm of the carotidartery. Usually polymicrobial,DCA occur from previous uncontrolled infections such as tonsillitis, den-tal infections, surgery, or trauma to the head and neck lymphadenitisafterupperairwaysinfection.2,6Itis neces-sary toinvestigate risk factors such asinfections, foreign bodies,trauma,immunosuppressionandaddictionto intra-venousdrugs.Concomitantdiseasessuchascongenitalcysts andfistulas,TB,diabetesmellitus,HIV,tumors,deficiency statesandsoonshouldalsobetakenintoconsideration.7 Theclinical manifestationsarediverse anddepend onthe affected cervical area. Moreover,an inappropriateuse of antibiotics may change the clinical presentation of infec-tions of thiskind, making themelusive.4 Patientsmay be mildly symptomatic and present with symptoms of fever and pain, or experience more severe or life threatening symptoms such as dyspnea airway obstruction and septic shock.
Thisstudyaimedtoreportourclinicalexperienceof sub-missionofdeepneckspaceinfectionsbythedescriptionof 101patientsdiagnosedinthelast6years.
Methods
Wereviewedthemedicalrecordsof101patientsdiagnosed with cervical infection spaces served by the Otolaryngol-ogy, Head and Neck surgery from a Brazilian Hospital of MedicalSchoolduringtheperiodfromJanuary2007to Jan-uary2013. Allpatientssigneda documentauthorizingthe useofdatafromtheirrecords(thatisastandard hospital procedure).
In all cases, the patients underwent a surgical proce-dure to drain pus. The diagnosis of deep neck abscess was suspected by clinical history and confirmed by Com-puted Tomography (CT)or surgery. This analysisexcluded patients with cervical infections who did not require surgery, such as cellulites, and superficial or limited infections. All patients were submitted to antibiotic therapy and, when possible, samples for culture and sensitivity.
We analyzed and compared the following clinical fea-tures:age,sex,clinicalsymptoms,leukocytecount,cervical area affected, lifestyle habits, antibiotic use, comorbidi-ties, etiology, bacterial culture, length of stay, need for tracheostomyandcomplications.
Alldescriptivedatawerereportedin percentages. Sta-tistical evaluationswere performed witha 2 sided t-test corrected for inequalityof variancesanddegreesof free-dom.Fisherexacttestand2testwereusedtocomparethe categoricalvariable.SPSS(13.0,SPSSInc,Chicago,IL)were usedtoanalyzethedataandap-value<0.05wasconsidered statisticallysignificant.
30
25
20
15
10
5
0
81-90
Age groups (years)
Number of patients (%)
0-10 11-20 21-30 31-40 41-50 51-60 61-70 71-80
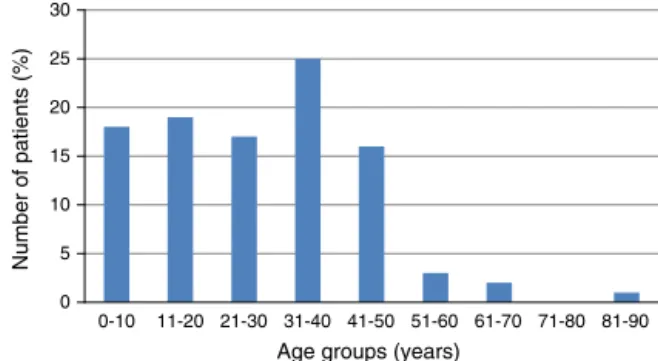
Figure1 Subjectsdistributionaccordingtoage.
Results
Population
Ofthe101patients,56weremaleand45female,55.5%and 44.5%respectively.Theiragesrangedfrom1to81yearswith ameanageof28.1years.Mostpatientswereyoung,the2nd and4thagegroups.Amongchildren,themeanagewas8.4 years,witha slight male predominance (57% of patients) (Fig.1).
Symptomsandtimetodiagnosis
Themostcommonsymptomsatdiagnosiswerefever(86.1%) andneckpain(81.1%).Othersymptomswereodynophagia (75.2%),cervical edema(60.3%)andtrismus(47.5%). Thir-teenpatients(12.8%)hadsymptomsofairwayobstruction, eightmalesandfivefemaleswithameanageof31.3years. Fifteenpatients(14.8%)hadsignsofbacteremiaatthetime ofdiagnosis,andthosecollectedbloodcultures.Themean timefromsymptomonsettothedemandforhealthservices waseightdays(range2---20days).
Lifestyleandcomorbidities
Nineteenpatients(18.8%)weresmokers,24patients(23.7%) alcoholics and 10 patients (9.9%) drug users. The most prevalent comorbidities were hypertension (19 patients, 18.8%),diabetes mellitus(DM)(13patients,12.8%).Other less prevalent comorbidities were obesity (10 patients, 9.9%),hypothyroidism(4patients,3.9%)andhepatitisC(3 patients, 2.9%). In two patients there wasan association withHIV(%).Theadultpatientsexhibitmorecomorbidities thanchildren(p<0.01)(Table1).
Etiology
Table1 Comparisonofchildrenandadults.
No.ofpatients No.ofmultispace No.ofcomplication Death No.ofcomorbidity
Children 27 2 8 0 0
Adults 74 31 40 2 51
p-Value <0.001 0.005 >0.10 <0.001
35
30
25
20
15
10
5
0
Number of patients (%)
Fasciitis Adenitis
Foreign body Lympadenitis Undeter mined
Odontogenic Tonsilite
Etiology
Figure2 Etiologyofdeepcervicalabscesses.
related to odontogenic infection there was a history of recentdentalmanipulation(Fig.2).
Spacesandcervicallymphnodes
Neck CT scan was performed to diagnose and assess the extent of infection in 71.2% of patients. The remaining patients had diseaseextension intraoperatively detected. Peritonsillarcervical areawasthemost affectedin 26.7% ofcases(27patients).Theotherareasaffectedin descen-dingorderwere:submandibular/floorofmouth(23patients, 22.7%),parapharyngeal (19 patients,18.8%), retropharyn-geal(18patients,17.8%),chewing(8patients,7.92%)and jugular-carotid(4patients,3.96%)(Fig.3).
AsTable2shows,thesitemostcommonlyinvolvedin chil-drengroup wasthe peritonsillarspace (10patients,37%), followedbyparapharyngealspace(9patients,33.3%),the
35 30 25
20
15 10
5 0
Affected area
Nu
mb
er
of p
a
tien
ts (%
)
Super ior mediastin
um
Jugular-carotid Masticator y
Retrophar yngeal
Paraphar yngeal
Submandib ular
Peritonsillar Multiple spaces
Figure3 Extentofinfeccionbydeepcervicalabscesses.
submandibularspacein4patients(14.8%)andthe retropha-ryngeal space in 4 patients (14.8%). In adults group, the sitemostcommonlyinvolved wasmultispace(31patients, 41.8%), followed by submandibular space in 19 patients (25.6%),theperitonsillarspacein17patients(22.9%).The adult patients developedmultispace infectionmore often thanthechildren(p<0.01)(Table1).
Therewastheoccurrenceofmultiplecervicalspacesin 33patients(32.7%).Whenpresent,lymphadenopathymost oftenreached levelsII andIII.Therewasextensiontothe superiormediastinumin2patients(1.9%).
Bacteriologyandleukogram
All patients received antimicrobial therapy. Amoxi-cillin+clavulanate was the most used antibiotics as first-line treatment (82.1% of cases), followed by cef-triaxone plus metronidazole combination. The change
Table2 Distributionofthesitesofdeepneckabscesses.
Childrenn(%)(n=27) Adults’n(%)(n=74) Total(n=101)
Multispace 2(7.4) 31(41.8) 33(32.6)
Parapharyngealspace 9(33.3) 10(13.5) 19(18.8)
PeritonsillarSpace 10(37) 17(22.9) 27(26.7)
Submandibularspace 4(14.8) 19(25.6) 23(22.7)
Retropharyngealspace 4(14.8) 14(18.9) 18(17.8)
Masticatorspace 0 8(10.8) 8(7.92)
Jugular-carotidspace 0 4(5.4) 4(3.96)
Table3 Complicationsofdeepneckabscesses.
Childrenn(%)(n=8)a Adults’n(%)(n=40)a Allpatients(n=101)a
Mediastinitis 0 2(5) 1.98%
Jugularveinthrombosis 0 1(2.5) 0.99%
Emergencytracheostomy 0 8(20) 7.92
Pneumonia 3(37.5) 8(20) 10.80%
Septicshock 3(37.5) 14(35) 16.80%
Surgicalrapprochement 2(25) 7(17.5) 8.90%
a Anindividualpatientmayhave2ormorecomplications.
25
20
15
10
5
0
Microorganism
Nu
mb
er
of p
a
tien
ts (%
)
Neisser ia sp
S. pneumoniae S. vir
idans S. aureus
S. constelatusS. inter medius
S. p
yogenes Others Polymicrobial
Figure4 Bacterialgrowthcultureindeepcervical abscesses.
of antibiotic depended on the culture results or clinical outcome.
Material for culture was obtained in 76.2% patients. There wasnobacterial growth in 14.5%of cases. Polymi-crobial culture was detected in 18.8% of patients, being Streptococcus pyogenes+Streptococcus pneumoniae the mostfrequentassociation.S.pyogeneswasthemost com-mon microorganism present in 25 patients (23.3%). The prevalenceofotherorganismswasasfollows:Streptococcus intermedius(20patients,18.6%),Streptococcus constelat-tus(16patients,14.9%),Staphylococcusaureus(13patients, 12.1%), Streptococcus viridians (9 patients, 8.4%), Strep-tococcuspneumonia (8patients, 7.4%) and Neisseriaspp. (7patients,6.5%).Othermicroorganisms(Corynebacterium spp.,Eikenellacorrodens,Enterococcusfaecium,Klebsiella pneumoniae and other Streptococci) were less frequent, totaling12 patients (11.8%). Seventeen patientshad clin-icalsignsofsepsisonarrivalat theemergencyroom,and blood tests were made, resulting positive in 13 patients (12.8% oftotal), withthemost prevalentoccurrence also ofStreptococcuspyogenes(Fig.4).
Complications,tracheostomyandmortality
The complications of deep neck infection are shown in Table 3. Complicationswere found in 48 patients (8 chil-dren, 40 adults). Of the 8 patients of children with complications, 3 had pneumonia, 3 had Septic shock and 2 hadsurgical rapprochement. The main complicationsof cervical abscesses included sepsis (17 patients, 16.8%),
pneumonia(11patients, 10.8%),mediastinitis (2patients, 1.9%)andjugularveinthrombosis(1patient,0.9%).Surgical rapprochement was required in 9 patients (8.9%), proba-blybecauseofthereorganizationofinfectioninstores(%). Theadultpatientsdevelopedinfectiouscomplicationsmore oftenthanthechildren(p=0.005)(Table1).
The upper airway obstruction and the impossibility of intubationforcedthetracheostomyin17patients(16.8%). Of these, 8 (7.9%) underwent emergency tracheostomy becauseofrespiratoryfailure.
There were 2 deaths (1.9% mortality rate). The first casewasa19year-oldhealthyfemalewithextensive cer-vical abscess associated with descending mediastinitis of undeterminedetiology.Thedeathoccurredonthe3rd post-operativedayandshehadsepsiswithpositivebloodculture for Streptococcuspyogenes.The second case was ofa 49 year-olddiabetic malewithabscess of odontogenic etiol-ogy(Ludwig’sAngina)extendingtothesubmandibularneck spaces/floor of the mouth and parapharyngeal space. He presentedsepsiswithpolymicrobialbloodcultures( Strep-tococcusviridians+Neisseriaspp.).
Theaveragehospitalstaywas9.7dayswithavariation between 2:45 days. Abscess complications prolonged the hospitalstayin about fivedays(averagelength ofstay of 14.8days).
Discussion
Deep neck abscesses are diseases of major importance due to its frequency and severe complications. The inci-denceisestimatedataround10/100,000inhabitants/year, withatendencytoincrease,especiallyinchildrenunder5 years,1inwhomtheestimatedincidenceisabout2/100,000 inhabitants/year.1Theinfectionshavenopreferenceforage orsexandcanaffectanyone.Inagreementwith Eftekhar-ianetal.studies,oursobserved ahigherincidenceinthe youngmalepopulationwithameanageof28.1years.8 How-ever, Huang et al. and other studies are also showing an upwardtrendintheincidenceofinfectionsinolderpatients andpatientswithsystemicdiseases.9Inthisgroup,defense mechanismswouldbeless efficient,recovery ratesslower andcomplicationswouldbemorefrequent.
incidence,having odontogenicinfections asthe most fre-quentcause.6,10,11Inourstudy,thebacterialtonsillitiswas themostcommoncause(31.68%),followedbyodontogenic infection(23.7%),totaling55.3%ofoursample.Other stud-ieshaveshownanincreaseassociatedwithintravenousdrug abuseand neck trauma infections, although we have not identifiedtheseetiologies.12
InastudybyCoelhoetal.,dentalfocuswastheoriginof abscessesin37%ofpatients,whereaspharyngealtonsiland disorderswerepresent in20%ofcases,notbeingpossible toidentifythesource ofinfectionin33%of patients.13 To Sennesetal.,odontogenicinfectionwasthecausein42.1% ofpatients,tonsillitisin17.5%,postupperairwayinfections in15.8%andunknowncausein8.8%14lymphadenitis.Among other causes,post upper airways infection,lymphadenitis andforeignbodyingestionwerestillfoundin17.8%ofcases, adenitis(submandibular andparotid)at 7.8%and39.6%in thefasciitis. Otherauthorsalsoreportedasignificant pro-portionofDCAwithunknownprimaryorigin,reachingupto 50%ofcases.2,6,15,16 In14.8%ofourpatients,theinfection etiologycouldnotbedetermined,probablybecausethe ini-tialinfectionwasnotpromptlydiagnosed, althoughithas preceded the abscess for weeks. Thus, the average time fromsymptomonsettodiagnosis of DCAin ourstudy was 8days,butreachedupto20daysandthemainsymptoms werefeverandneckpain.
The knowledge of the anatomic relationships between neckspacesisimportantforthetherapeuticmanagement, sincethefascialimitingthesespacesareimportant anatom-icalbarriers tothe spread of infection,but also serve to directinfectiononceitsnaturalresistanceisovercome.17
Mostpreviousstudies1,18,19 reportedthatchildrenarea relatively low proportion of their patients with DCA. We found,however,thattheproportionofpatients whowere under18yearsofagewerehigh(27cases,26.7%),andnone of themhad DM or other associated diseases. Other indi-cators of health care utilization such asmedication used beforeandfrequencywerenotpossibletoobtain because mostpatientsreceivedtreatmentfor theiracuteepisodes at remote locations, either by their primary care physi-ciansorbythereferringotolaryngologist.However,probably thismaybecausedbythehistoryofantibioticsabuseand theantibioticresistanceexplainedbyindiscriminateuseof antibiotics, especially in colds and other viral infections, which are more prevalent in children than in adults.20,21 Previousantibioticuseiscorrelatedwithhigherrecoveryof resistantorganismsandincreasedincidenceof -lactamase-producing bacteria.22,23 Ultimately, the resistance had an effect on the incidence of deep neck infection.24 Larger prospectivestudies areneeded to address many of these limitationsandtofurtherdelineatetherolefor understand-ingthedifferentcharacteristics betweenthechildrenand adultswithdeepneckinfection,helpinginaccurate evalu-ationandpropermanagement.
Most studies5,25 reported the retropharyngeal space as the most common involved space in children, but we found the peritonsillar space the most common involved in children group (10---27 patients, 37%), closely followed byparapharyngealspace(9---27patients,33.3%).However, thereis onestudy4showedthattheparapharyngealspace was as the most common involved space in children. It mightbeexplainedbeacauseinfectionsintheperitonsillar,
submandibular, masticatory,andparotidspacecanusually spreadtotheparapharyngealspace.9 Multispaceinfection wasfoundin31patients(41.8%)inadultsandin2patients (7.4%)inchildren(p<0.001).Adultswereeasiertoget mul-tispaceinfectionthanchildren;thismightrelatetoahigher incidence of disease comorbidity in adults. Patients with disease comorbidity tend to have poorer defense against infections and thus result in higher rates of more severe infection in the form of multispace infections.18 In both deathstherewasinvolvementofmultiplecervicalspaces.
TheDCAmicrobiologyischaracterizedbygenerallybeing polymicrobialinfections, includingaerobicand anaerobic, gram positive particularly. Among the agents commonly found are: Streptococcus viridans, Streptococcus milleri, Prevotella spp., Peptosstreptococcus spp. and Klebisiella pneumoniae, the latter being more common in diabetic patients.26 SennesfoundStreptococcusviridansin41.5%of thecases,Staphylococcusaureusin20.7%ofthem,and3.8% withHaemophilusinfluenza.14 In ourstudy,Streptococcus
pyogeneswasthemostfrequentlydetectedagent(23.3%), whichcanbeexplainedbythehigherincidenceof periton-sillarinfections.Fromallpatients,14.5%showednogrowth ofbacteriainculture,whichcanbeexplainedbytheuseof highdosesofintravenousantibioticsbeforeabscesssurgical drainage.27 In 12.8% of patients, it was detected positive bloodculture,whichshowsthehighpossibilityofsystemic spreadofaninfectioninitiallyuncontrolled.
Many studies have shown the association of DM with DCA.9,28 Huangetal.9,20 andLeeetal.18 indicatedthatold patientswithDMweresusceptibletodeepneckinfection. In DMpatients,hyperglycemia mayimpairseveral mecha-nisms of humoral host defense, such asvariedneutrophil functions:adhesion,chemotaxisandphagocytosisandresult in predisposition to infection and complications.29 Huang et al. found high rates of infection withKlebsiella pneu-moniae in diabetic patients.9 The prevalence of diabetic patientsinourstudywaslow(12.8%),withStaphylococcus aureus(5patients)andStreptococcuspyogenes(4patients) as the microorganisms most commonly found. In one of thelethaldevelopments,thepatientwithpoorlycontrolled diabetes had the blood culture positive for Streptococcus viridians+Neisseriaspp.
The management of DCA involves surgical drainage associated with use of intravenous antibiotics. Computed tomography withcontrastwasthetest ofchoicefor diag-nosingandassessingtheabscessextent.Althoughithashigh sensitivity,thetest specificityislow,for exampleincases of lymphnode clusters without associatedabscess, which canleadtounnecessarysurgicalprocedures.30Ohetal.and otherresearchershavedemonstratedtheefficacyofneedle drainageofabscessguidedbyultrasound,withnoincrease incomplicationrates.27Ingeneral,thisconservative treat-mentiseffectiveinsmallcollectionsandwithnoevidence ofimminentcomplications.Ourservicehaslittleexperience inthistreatment,preferringtheopensurgical drainagein allcases.
empiricalcoverage,apenicillinwitha-lactamaseinhibitor combination(suchasamoxicillinandclavulanicacid),ora -lactamantibiotic-resistant(suchascefuroxime,meropenem or imipenem) in combination witha drug,which is highly effectiveagainstmostanaerobes(suchasmetronidazoleor clindamycin).17,28 Afebrile after 48h, thepatient was dis-chargedwithaprescriptionoforalantibiotic.
Despitethewidespreaduseofantibiotics,several unde-sirableandlife-threateningcomplicationsofDCAareknown asdescendingmediastinitis, jugularveinthrombosis, peri-carditis, pleural empyema, arterial erosion,upper airway obstructionandsepsis.Inourstudy,thereweretwocases ofmediastinitis,bothinadultsandinvolvingmultipleneck spaces,anddeathinsepticshockinoneofthem(Table1). In mediastinitis,the patientoften complains of increased chest pain or dyspnea. The extent of disease occurs via anteriorvisceralspaceandmortalitycanreachhalfofthe cases,requiringcombinedthoracicdrainage.31The obstruc-tionoftheupperairwayandconsequentrespiratoryfailure forcedtheemergencytracheostomyin7.9%ofpatients. Har-Eletal.describethatthe involvementofthefloorof the mouthandtheretropharyngealspacearemoreassociated withairwayobstructionandgreaterneedfortracheostomy, procedurenecessaryin75%ofthecases.10 Itis interesting tonote that in ourstudy,especiallyin patients with sec-ondary involvement of the masticatory muscles, trismus, tracheostomywasnecessarybecauseoftheimpossibilityof intubation, evenwithout the presenceof respiratory fail-ure.Ourmortalityratewas1.9%,similartothatdescribed byHuangetal.(1.6%).9
We presented here relevant information about clinical andsurgicalDCAoutcomes.However,thecourseand sever-ity of the same infection in different patients can vary widely,requiringanexperiencedteamtodealwithit.
Conclusions
Deepneckinfectionsconstituteamedicalandsurgical emer-gency. The clinical features and severity of DCA varied accordingtodifferentagegroups,perhapsduetothe loca-tionoftheinfectionandahigherincidenceofcomorbidity inadults.Thus,DCAinadultsismorefaciletohave multi-spaceinvolvementandleadtocomplicationsandseemsto bemoreseriousthanthatinchildren.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GorjónPS,PérezPB,MartínACM,DiosJCP,AlonsoSE,Cabanillas MIC.Infeccionescervicalesprofundas. Revisiónde286casos. ActaOtorrinolaringolEsp.2012;63:31---41.
2.SakagushiM,Sato S,Ishiyama T,Katsuno S,TagushiK. Char-acterizationand managementofdeep neckinfection.JOral MaxillofacSurg.1997;26:131---4.
3.Raffaldi I, LeSerre D,Garazzino S, Scolfaro C,Bertaina C, MignoneF,etal.Diagnosisandmanagementofdeepneck infec-tionsinchildren:theexperienceofanItalianpaediatriccentre. JInfectChemother.2015;21:110---3.
4.YangW, HuL, Wang Z,NieG,Li X, LinD,etal. Deepneck infection:a reviewof130cases inSouthernChina. Medicine (Baltimore).2015;94:e994.
5.Abdel-HaqNM,HarahshehA,AsmarBL.Retropharyngealabscess inchildren:theemergingroleofgroupAbetahemolytic strep-tococcus.SouthMedJ.2006;99:927---31.
6.LeeJK,KimHD,Lim SC.Predisposingfactorsofcomplicated deep neckinfection:ananalysisof158cases.YonseiMedJ. 2007;48:55---62.
7.HasegawaJ,HidakaH,TatedaM,KudoT,SagaiS,MiyazakiM, etal.Ananalysisofclinicalriskfactorsofdeepneckinfection. AurisNasusLarynx.2011;38:101---7.
8.EftekharianA,RoozbahanyNA,VaezeafsharR,NarimaniN.Deep neckinfections:aretrospectivereviewof112cases.EurArch Otorhinolaryngol.2009;266:273---7.
9.HuangTT,LiuTC,ChenPR,TsengFY,YehTH,ChenYS.Deep neck infection: analysis of 185 cases. Head Neck. 2004;26: 854---60.
10.Har-ElG,AroestyJH,ShahaA,LucentFE.Changingtrendsin deepneckabscess.OralMedOralPathol.1994;77:446---50.
11.LarawinV,NaipoJ,DubeySP.Headandneckspaceinfections. OtolaryngolHeadNeckSurg.2006;135:889---93.
12.SethiDS,StanleyRE.Deepneckabscesses----changingtrends.J LaryngolOtol.1994;108:138---43.
13.CoelhoMS,RamosG,PrestesLC,SoccolA,OliveiraMSB,Lobo P.Deepneckinfections---classificationinlevelsofseverity.Int ArchOtorhinolaryngol.2009;13:184---8.
14.Sennes LU, Imamura R, Júnior FVA, Frizzarini R, Tsuji DH. Infecc¸õesdosespac¸oscervicais:estudoprospectivede57casos. RevBrasOtorrinolaringol.2002;68:388---93.
15.Wang LF, Kuo WR, Tsai SM, Huang KJ. Characterizations of life-treateningdeepcervicalspaceinfections:areviewofone hundredninety-sixcases.AmJOtolaryngol.2003;24:111---7.
16.GidleyPW,GhorayebBY,eStiernbergCM.Contemporary man-agementofdeepneckspaceinfections.OtolaryngolHeadNeck Surg.1997;116:16---22.
17.VieiraF,AllenSM,StocksRSM,ThompsonJW.Deepneck infec-tion.OtolaryngolClinNAm.2008:459---83.
18.LeeYQ,KanagalingamJ.Deepneckabscesses:theSingapore experience.EurArchOtorhinolaryngol.2011;268:609---14.
19.HuangTT,TsengFY,LiuTC,HsuCJ,ChenYS.Deepneckinfection in diabeticpatients: comparisonof clinicalpicture and out-comeswithnondiabeticpatients.OtolaryngolHeadNeckSurg. 2005;132:943---7.
20.MontoAS.Studiesofthecommunityandfamily:acute respira-toryillnessandinfection.EpidemiolRev.1994;16:351---73.
21.Heikkinen T, Jarvinen A. The common cold. Lancet. 2003;361:51---9[PubMed].
22.BrookI,GoberAE.Prophylaxiswithamoxicillinorsulfisoxazole forotitismedia:effectontherecoveryofpenicillin-resistant bacteriafromchildren.ClinInfectDis.1996;22:143---5.
23.BrookI,GoberAE.Resistancetoantimicrobialsusedfortherapy ofotitismediaand sinusitis:effectofpreviousantimicrobial therapyandsmoking.AnnOtolRhinolLaryngol.1999;1087Pt 1:645---7.
24.CoticchiaJM,GetnickGS,YunRD,ArnoldJE.Age-,site-,and time-specificdifferencesinpediatricdeepneckabscesses.Arch OtolaryngolHeadNeckSurg.2004;130:201---7.
25.DawesLC,BovaR,CarterP.Retropharyngealabscessinchildren. ANZJSurg.2002;72:417---20.
27.SethiDS,StanleyRE.Parapharyngealabscesses.JLaryngolOtol. 1991;105:1025---30.
28.ParhiscarA,Har-ElG.Deepneckabscess:aretrospectivereview of210cases.AnnOtolRhinolLaryngol.2001;110:1051---4.
29.Hostetter MK. Handicaps to host defense: effects of hyper-glycemiaonC3andCandidaalbicans.Diabetes.1990;39:271---5.
30.Miller WD, Furst IM, Sandor GKB, Keller MA. A prospec-tive, blinded comparison of clinical examination and
com-puted tomography in deep neck infections. Laryngoscope. 1999;109:1873---9.