PDF EN Jornal Brasileiro de Pneumologia 1 19 english
Texto
Imagem
Documentos relacionados
The probability of attending school four our group of interest in this region increased by 6.5 percentage points after the expansion of the Bolsa Família program in 2007 and
Na hepatite B, as enzimas hepáticas têm valores menores tanto para quem toma quanto para os que não tomam café comparados ao vírus C, porém os dados foram estatisticamente
Copy of a circular letter dated 11 June 1957 transmitted by the Director-General of the World Health Organization inviting the Member States of WHO to indicate whether they wish
A análise fatorial revelou o crescimento econômico e a infraestrutura como os fatores determinantes do desenvolvimento e das desigualdades no TSB, e também possibilitou hierarquizar
didático e resolva as listas de exercícios (disponíveis no Classroom) referentes às obras de Carlos Drummond de Andrade, João Guimarães Rosa, Machado de Assis,
Dos objectivos traçados no nosso trabalho, verificamos que da análise quantitativa da transição das Lux GAAP para as IFRS nas diferentes rubricas, bem como nos
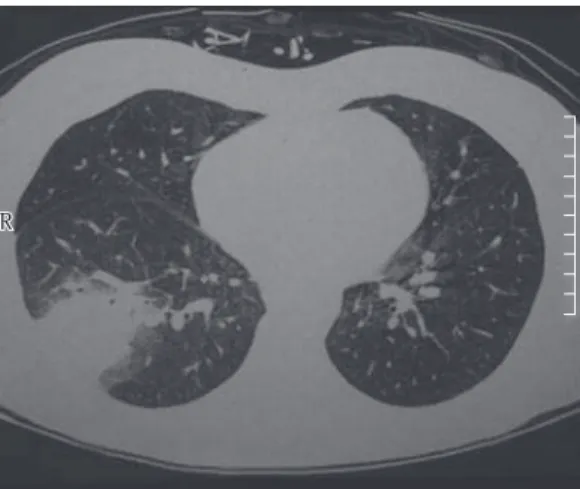
Pulmonary complications are the most common cause of morbidity and mortality in immunocompromised patients, who lack of the basic mechanisms of cellular defense.. Regardless of
Ousasse apontar algumas hipóteses para a solução desse problema público a partir do exposto dos autores usados como base para fundamentação teórica, da análise dos dados
