r e v b r a s r e u m a t o l . 2016;56(2):178–180
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Association
between
rheumatic
fever
and
Takayasu’s
arteritis
–
Case
report
Natali
W.S.
Gormezano,
Maria
Carolina
dos
Santos
∗,
Eunice
Mitiko
Okuda,
Liane
Hulle
Catani,
Silvana
B.
Sacchetti
RheumatologyandCardiologyServices,DepartmentofPediatrics,IrmandadedaSantaCasadeMisericórdiadeSãoPaulo, SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11February2014 Accepted5September2014 Availableonline20February2015
Keywords: Rheumaticfever Takayasu’sarteritis Cardiacmanifestations
a
b
s
t
r
a
c
t
Takayasu’sarteritis(TA)andrheumaticfeverarediseasesthatcanstartwithcardiac fea-tures,makingthediagnosisdifficult.TherearereportsofassociationofRFwithTakayasu’s arteritisbeginningwithcardiacinvolvementinpediatricpatients.Theaimofthisstudyis toreportthepossibleassociationofRFandTAinpatientswithcardiacabnormalities.We describethecaseofanadolescentinitiallydiagnosedwithRFwhoprogressedwithchanges thatallowedmakingthediagnosisofTA.TAandRF aretwoimportantcausesofvalve involvementthatmayhavesystemicmanifestations.
©2014ElsevierEditoraLtda.Allrightsreserved.
Associac¸ão
entre
febre
reumática
e
arterite
de
Takayasu
–
Relato
de
caso
Palavras-chave: Febrereumática ArteritedeTakayasu Manifestac¸õescardíacas
r
e
s
u
m
o
AarteritedeTakayasu(AT)eafebrereumática(FR)sãodoenc¸asquepodemteriníciocom manifestac¸ãocardíaca,oquedificultaodiagnóstico.Hárelatosdeassociac¸ãodeFRcom ATqueseiniciacomcomprometimentocardíaconafaixaetáriapediátrica.Oobjetivodeste estudoérelatarapossibilidadedaassociac¸ãodeFReATempacientecomalterac¸ãocardíaca. DescrevemosocasodeumaadolescentediagnosticadainicialmentecomoFRque apresen-tounaevoluc¸ãoalterac¸õesquepermitiramodiagnósticodeAT.AATeaFRsãoduascausas importantesdeenvolvimentovalvularquepodemapresentarmanifestac¸õessistêmicas.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
∗ Correspondingauthor.
E-mail:[email protected](M.C.Santos).
http://dx.doi.org/10.1016/j.rbre.2014.09.003
rev bras reumatol.2016;56(2):178–180
179
Introduction
Takayasu’sarteritis (TA)isachronicgranulomatous inflam-matory disease that canaffect the aorta, its branches and pulmonaryartery.1,2
Inchildren,itaffectswomenataratioof2:1,similarlyto thatfoundinaBrazilianmulticentricstudyof71childrenand adolescents(2.6:1).3Meanageofonsetis11.4years,with20%
before19yearsand2%before10yearsofage.4
The initial manifestations may be insidious and non-specific, such as asthenia, headache, fever, night sweats, arthralgia,musclepainandweightloss,startingatvariable timesbeforevasculardisease,ormaybeacutewithhighblood pressure,seizuresandcongestiveheartfailure.5
Cardiac impairment occurs inabout 50% of patients in thecourseofthedisease,andanycardiacstructurecanbe affected.Whenpresentedwithvalveregurgitation,thepatient mayinitiallybediagnosedwithrheumaticfever.
WereportedacaseofTAinanadolescentwithcardiacvalve impairmentwithearlydiagnosisofrheumaticfever.
Case
report
A15-year-oldadolescent,female,white,wasadmittedwith ahistoryofpalpitationsassociatedwithadynamiaand7-kg weight loss, 10 monthsago. On physicalexamination, the patientwaspale,tachycardic,andafebrilewithbloodpressure (BP)of130×70mmHg(90-percentile).Oncardiacauscultation,
loudP2andsystolicmurmurinmitralarearadiatingtothe backpresentsymmetricalpulses.
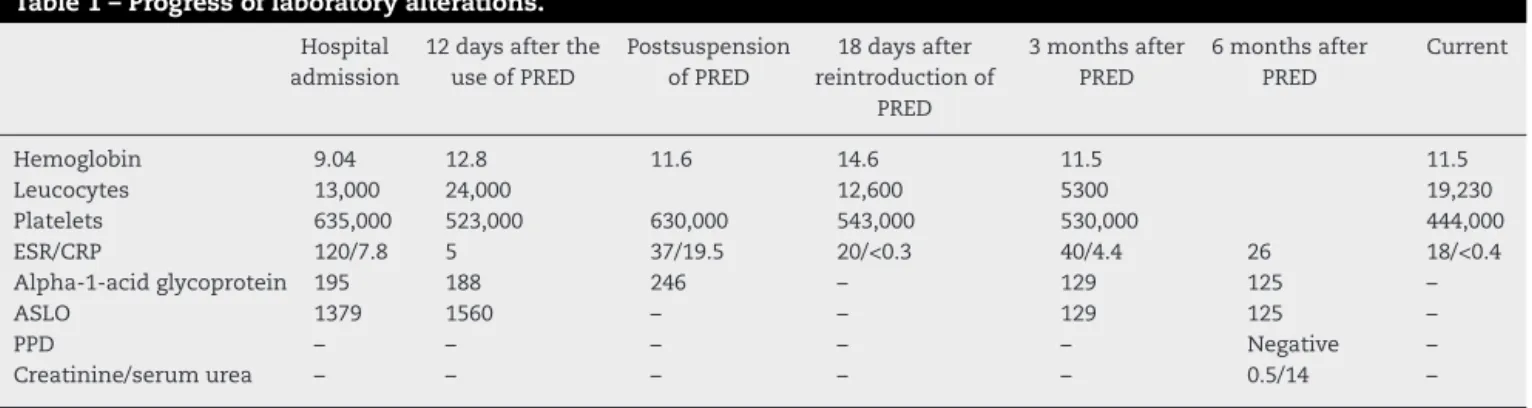
Laboratorytestsshowedanemia, withmildleukocytosis andthrombocytosis,elevatedinflammatoryactivityand titra-tionofanti-streptolysinOantibody(ASLO)(Table1).
Chestradiographyshowedcardiacareaattheupperlimit, theechocardiogramshowedmoderateleftventricular dilata-tionwiththickeningofthemitralvalveandmitral(mild)and aortic(mildtomoderate)regurgitation,withanejection frac-tionof51%,andinflammationonmyocardiumscintigraphy. With these data, shewas diagnosedwith rheumatic fever (RF).Treatmentwithprednisone,digoxin,and hydrochloroth-iazide was initiated, with prophylaxis with benzathine penicillin,withnormalizationofinflammatoryactivity.In out-patientfollow-up,corticosteroidsweregraduallyreducedand
Table1–Progressoflaboratoryalterations.
Hospital admission
12daysafterthe
useofPRED
Postsuspension
ofPRED
18daysafter
reintroductionof
PRED
3monthsafter
PRED
6monthsafter
PRED
Current
Hemoglobin 9.04 12.8 11.6 14.6 11.5 11.5
Leucocytes 13,000 24,000 12,600 5300 19,230
Platelets 635,000 523,000 630,000 543,000 530,000 444,000
ESR/CRP 120/7.8 5 37/19.5 20/<0.3 40/4.4 26 18/<0.4
Alpha-1-acidglycoprotein 195 188 246 – 129 125 –
ASLO 1379 1560 – – 129 125 –
PPD – – – – – Negative –
Creatinine/serumurea – – – – – 0.5/14 –
discontinuedafterthreemonthsofitsinitiation,maintaining adequatesecondaryprophylaxis.
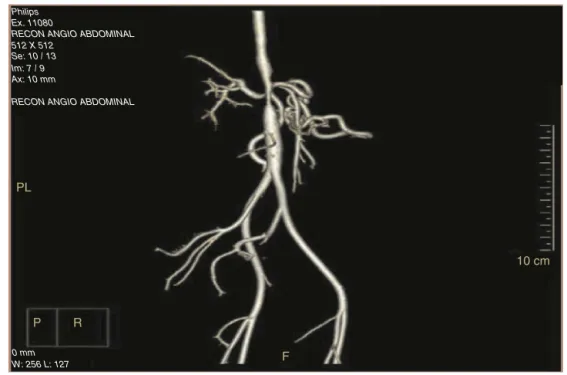
Afterdiscontinuationofcorticosteroids,sheshowed exer-tionaldyspnea,tachycardia,lowerlimbedema,auscultation ofepigastricmurmursandincreasedbloodpressure.On labo-ratoryinvestigation,inflammatoryactivitytestswerehighand PPDwasnegative.Echocardiographyrevealednormalmitral valveandmildaorticregurgitationandanejectionfraction of63%.Chesttomographydetectedparietalthickeningofthe aortaand itsbranches,and presenceofdilation (2.6cm)in thethoracoabdominaltransitionthatissuggestiveof arteri-tis. The hypothesis of TA was confirmed by the changes evidenced inarteriography. (Fig.1)Methotrexate and pred-nisonewereassociatedwithclinicalandlaboratorycontrolof inflammation.
Currently,thepatientisbeingfollowedondiagnosisofTA and RF, withprednisone, methotrexate, folic acid, digoxin, anti-hypertensives and prophylaxis with benzathine peni-cillin.
Discussion
TA is uncommon, especially in the pediatric population, althoughitisamajorcauseofrenovascularhypertension.
Genetic factors and infectious and immunological pro-cessesaredescribedinetiopathogenesis.
Inthecasedescribed,asJonescriteriaweremet,itallowed thediagnosisofRF,butthenonspecificmanifestationsthat precededFR symptomssuggest thepresenceofasystemic inflammatoryvasculitisofinsidiousonset.6Inthecourseof
thedisease,thepresenceofepigastricmurmur,hypertension andabnormalangiographyallowedthediagnosisofTAbased ontherevisedcriteriaEULAR/PReS.7TheassociationofRFand
TAisuncommon.8Tejadaetal.9reported2casesofrheumatic
heartdiseaseinaseriesof125patientswithTA.Atourservice, within11 casesofTA, onlythispatient hadheart changes consistentwithRF.
Cardiacinvolvementoccursinupto50%ofpatientswith TA,andmayimpairanyheartstructure.10,11Coronary
arteri-tis,heartvalvelesion,andventricularaneurysmarethemain manifestationsreportedinchildrenwithTA.
180
rev bras reumatol.2016;56(2):178–180Philips Ex. 11080
RECON ANGIO ABDOMINAL
RECON ANGIO ABDOMINAL
PL
P R
F
10 cm 512 X 512
Se: 10 / 13 Im: 7 / 9 Ax: 10 mm
0 mm W: 256 L: 127
Fig.1–Arteriographicalterations.
tricuspidvalvesinapproximately 20%ofTApatients, often withregurgitation,withnoevidenceofvalvethickening.11In
autopsystudies,therearereportsofaorticvalvethickening secondarytoarteritisoftheaortaextendingtovalveandmural endocardium.12
Thepresenceofmitralvalvethickening,associatedwith streptococcus,withresolutionaftertreatmentwith cortico-steroidsdoesnotallowrulingoutTA-associatedRF.According toValeetal.13,thecombinationofRFandTAraisesthe
possi-bilityofacommonimmunologicbasisinthepathogenesisof bothdisorders.
TAandRFaretwomajorcausesofvalveinvolvement,the presenceofsystemicmanifestations,echocardiographicand arteriographicfindingsarehelpfulinthediagnosisofcardiac involvement.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BrunnerJ,FeldmanBM,TyrrellPN,Kuemmerle-DeschnerJB, ZimmerhacklLB,GassnerI,etal.Takayasu’arteritisin childrenandadolescents.Rheumatology.2010;49:1806–14.
2. MesquitaZBM,SacchettiSB,AndradeOVB,MastrocinqueTH, OkudaEM,BastosW,etal.ArteritedeTakayasunainfância. RevisãodeLiteratura.Apropósitode6casos.JBrasNefrol. 1998;20:263–75.
3. ClementeG,HilarioMO,LedermanH,SilvaCA,SallumAM, CamposLM,etal.TakaysuarteritisinaBrazilianmulticenter
study:childrenwithalongerdiagnosisdelaythan
adolescents.ClinExpRheumatol.2014;322Suppl.82:5128–31.
4.MendiolaRamírezK,PortilloRiveraAC,GaliciaReyesA,García MontesJA,MaldonadoVelázquezMdelR,FaugierFuentesE. TypeIIITakayasu’sarteritisinapediatricpatientcasereport andreviewoftheliterature.ReumatolClin.2012;8:216–9.
5.AyparE,Celebi-TayfurA,KeserM,OdabasD,ÖzaltinF,Paksoy Y,etal.Takayasu’arteritisina4-year-oldgirl:casereportand briefoverviewofthepediatricliterature.TurkJPediatr. 2012;54:536–9.
6.WeissPF,CoraoDA,PollockAN,FinkelTH,SmithSE. Takayasu’arteritispresentingascerebralaneurysmsinan18 monthold:acasereport.PediatrRheum.2008;6:4.
7.OzenS,RupertoN,DillonMJ,BaggaA,BarronK,DavinJC, etal.Eular/PReSendorsedconsensuscriteriaforthe classificationofchildhoodvasculitides.AnnRheumDis. 2006;65:936–41.
8.RoghiA,PedrottiP,MilazzoA,VignatiG,MartinelliL,PainoR. Acutemyocardialinfarctionandcardiacarrestinatypical Takayasu’aortitisinayounggirl.Unusualdiagnosticroleof cardiacmagneticresonanceimaginginemergencysetting. Circulation.2010;121:e370–5.
9.TejadaO,TorresS,AlfaroK.CardiacdamageinTakayasu’s arteritisstudyin125patients.ArchInstCardiolMex. 1983;53:441–7.
10.RavelliA,PedroniE,PerroneS,TramarinR,MartiniA,Burgio GR.Aorticvalveregurgitationasthepresentingsignoof Takayasu’arteritis.EurJPediatr.1999;158:281–3.
11.MiloslavskyE,UnizonyS.Theheartinvasculitis.RheumDis ClinNam.2011;40:11–26.
12.ChhetriMK,PalNC,ChandrikaN,ChowdhuryND,Basu MullickKC.EndocardiallesioninacaseofTakayasu’s arteriopathy.BrHeartJ.1970;32:859–62.