w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Recto-sigmoid
lipoma:
a
case
report
and
review
of
the
literature
Gholamreza
Bagherzade
a,
Omid
Etemad
b,∗aShahidBeheshtiUniversityofMedicalSciences,ColorectalSurgeryWard,Tehran,Iran
bShahidBeheshtiUniversityofMedicalSciences,Tehran,Iran
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25May2016 Accepted8June2016 Availableonline9July2016
Keywords:
Lipoma Recto-sigmoid Colorectal
a
b
s
t
r
a
c
t
Lipomasareagrowthoffatcellsinafibrouscapsule.Theyaremostcommonin noncancer-oustissues.Lipomaofrectumisuncommonandthemostcommonsitofitsoriginisthe perinanalregion.Rarelytheycouldcauserectalbleeding.Inthisstudy,wehavereported a53-yrsold manwhohadbeenreferredtothe hospitalwithsymptomsofabdominal pain,rectalbleedingandthe probleminbowel movement.Rectalprolapsed with soli-taryrectalwereobservedduringtheclinicalobservation.Colonoscopy,CT-ScanandMRI wereperformedforthepatientandtheresultsshowedamasssuggestivetolipomawhich waslocatedinrecto/sigmoidregion.Heunderwentthesurgery.Intraoperativefindings showedseveralsoftmassesinrectumandalargemasswithdimensionof10cm×10cm
insigmoid.Lowanteriorresectionwasperformedforhimandpathologydiagnosiswas lipoma.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Lipoma
retossigmoide:
relato
de
caso
e
revisão
da
literatura
Palavras-chave:
Lipoma Retossigmoide Colorretal
r
e
s
u
m
o
Lipomassãoumcrescimentodeadipócitosemumacápsulafibrosa.Essasformac¸õessão maiscomunsemtecidosnãocancerosos.Olipomadoretoéderaraocorrência,eolocal maiscomumparasua origemé a regiãoperianal.Raramente essas formac¸õespodem causarsangramentoretal.Nesseestudo,descrevemosumpaciente,homem,53anos,que foiencaminhadoaohospitalcomsintomasdedorabdominal,sangramentoretale prob-lemasnosmovimentos intestinais. Aoexame clínico,foram observados prolapsoretal comsolitáriadorecto.FoirealizadaumacolonoscopiaeobtidosestudosdeTCeIRM;os
∗ Correspondingauthor.
E-mails:[email protected],[email protected](O.Etemad).
http://dx.doi.org/10.1016/j.jcol.2016.06.003
resultadosdemonstraramumamassasugestivadelipoma,localizadanaregião retossig-moide.Opacientefoiencaminhadoàcirurgia.Osachadosintraoperatóriosdemonstraram váriasmassasmaciasnoretoeumagrandemassaquemedia10cm×10cmnosigmoide.
Foirealizadaaressecc¸ãoanterioreodiagnósticodapatologiafoilipoma.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Lipomasofrectum and colon are rare and the more com-monsitesoftheirorigin arethe perianal region.1,2 Colonic
lipoma was first described by Bauer in 1757.3 Lipomas
often occur as solitary lesions in contrast to colonic lipo-maswhichtendtooccur asmultiplelesions.Patientsmay beasymptomatic or may present with tenesmus when its location isinthe distalrectum. Alarge lipomamay cause symptoms of obstruction because of its size. A peduncu-lated lesion may prolapse through the anal canal.4 The
tumorissoftandwell circumscribedonpalpation,withits yellowish color visible through the overlaying mucosa on visualization using a proctoscope or endoscope. The over-layingmucosacanbepinchedup,andthelesionisusually compressible.5
Fortreatmentthelargelesionsofcoloniclipomas,thereare severalsurgicalmethodsincludinghemicolectomy,segmental resectionofinvolvedcolonorlocalexcision.6
In case of rectal lipomas, treatment can be done by transanalincisionorendoscopicallyifitispedunculated.7A
largerectallipomamayrequireatransabdominalapproach forcompleteremoval.
Inthiscasereport,wereportedarecto-sigmoidlipomawith dimensionsof116mm×680mm.
Fig.1–Spiralabdomino-pelvicCT-Scan.
Case
report
A 53-yrs-old manwas referred tothe hospitalwith symp-tomsofabdominalpain,rectalbleedingandprobleminbowel movement.Duringclinicalexaminations,rectalprolapsewith solitary rectal ulcer were observed. Colonoscopy was per-formedforhim.
Colonoscopyreportedoneinfiltrated ulcerativelesionin 3cmfromthe analvergetill8cm fromanaland oneother largeulcerativefungatingmassneartotalobstructivemass from25cmtill31cmfromanalverge.Non-diagnosticbiopsy wasperformedforhimandtherewasnoevidenceofdysplasia ormalignancy.
AswecanfindinFig.1,spiralabdomino-pelvicCT-Scan wasdoneforhimand weobservedthicknessofrectalwall withpre-rectalfatstandinganda64mm×112mmfat-density
masswithintherecto-sigmoidlumenthatwasdisplaced for-wardtheurinarybladder.
Abdomino-PelvicMRIshowedafatcontainingwell-defined large (110mm×68mm) mass atrectum and recto-sigmoid
junction.Thefindingsweresuggestiveofrectallipoma.Fig.2
showstheMRIforthispatient.
Fig.2–Abdomino-pelvicMRI.
Rectoscopy was performed that was suggestive to rec-talprolapse,nodularityandsolitaryrectalulcer.Biopsywas doneandtherewasnomalignancy.Duringthesurgery,the intra-operativefindingsshowedasoftintramuralmasswith dimensionsof10cm×10cminrecto-sigmoidregion.
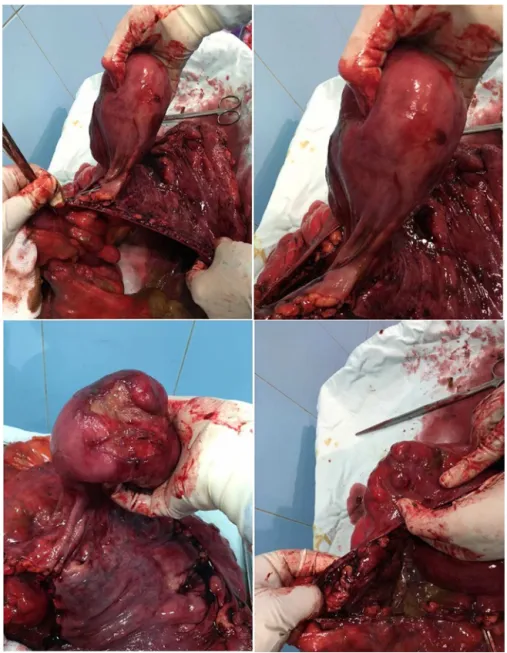
Low anterior resection was performed and one other lipomamasswithfewerdiameterswasremovedfromthe rec-tum.Theoperationwasendedafterrectopexy.Fig.3showsthe removedsectionsofsigmoidandupperrectum.
Pathologyfindingsareasfollows:
- Multiplelipomainrecto-sigmoidwithdiametersof1–15cm - Fociulceratedmucosa
- 12reactivelymphnodes - Negativeformalignancy
Discussion
Lipomas are composed of mature adipose tissue and are surrounded byafibrotic capsule.They usuallyarise inthe submucosallayerofthecaecumorthesigmoidcolon. Occur-renceoflipomaincolonisuncommon.Until2011,total227 patientswithcolorectallipomawerereported.Ofthis num-bers,9patientsexperiencedrectallipoma.Therearealsosome casesthatwerereportedduetothe rectallipomaand pre-sentedwithprolapse.8–11
65%oflipomasinthegastrointestinalsystemwerelocated inthecolonand20–25%oftheminthesmallintestine.12,13
Lipomas are mostly common at the ascending colon and transversecolon andrarely atthe descendingand sigmoid colonandrectum.14,15
Inan18-yrsanalysiswhichwasdoneon17patientswith large-bowel lipoma, onlythree patients experienced rectal lipoma.16Inanother10-yrsanalysisdoneinMayoClinic,of
91patientswithlarge-bowellipoma,nopatientwasreported withrectallipoma.17
Someauthorsreportedthatmostofaffectedpatientswere betweenagesof50-till70-yrs.18
Lipomasare well differentiated arisingfrom deposits of adiposeconnectivetissueinbowelwall(90%submucosal,10% subserosal).19Mostlipomasarediagnosedwithcolonoscopy
assoftyellowishtumorsorpolypsidentifiedbypressuringthe biopsyforceps.20
Aslong as the colonic lipomas are asymptomatic, they do not require treatment. However with size in excess of 2cm they give rise to some symptoms: constipation, diar-rhea,abdominalpain,rectalbleedingandintussusceptions.21
Colonoscopyresectionisatreatmentchoice.Ifnotpossiblea limitedsegmentalresectionorlipomectomycanbeadvised.22
Dependsontheconditionsofthepatient,bothtrans-anal excisionandlaparoscopicprocedurescanbedoneforthemas aplanoftreatment.23
Conclusion
Todistinguishtherectal/coloniclipomasfromtheother colo-rectal tumors, paraclinical examinations, colonoscopy and biopsy should be done. Due to the complications such as
rectal bleeding, obstruction andabdominal pain, colorectal lipomaswithdiametersofmorethan2cmshouldberemoved. Thereareseveralmethodsforthisaim.Colonoscopyremoval isadvisedforthelipomaswithdiameteroflessthan2cmin caseofexceededsize,surgicalextractionisnecessary.3,24Due
totheprobabilityofexistenceofmultiplelipomamasses,full observationishighlyrecommended.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ChowdriNA,ParrayFQ.Benignanorectaldisorders.Edited version;2016.
2.HayesHT,BurrHB,MeltonWT.Submucouslipomaofthe colon:reviewoftheliteratureandreportoffourcases.Dis ColonRectum.1960;3:145–8.
3.MasonR,BristolJB,PetersenV,LubyrnID.Gastrointestinal: lipomainducedintussusceptionoftransversecolon.J GastroenterolHepatol.2010;25:1177.
4.ZurkirchenMA,LeuteneggerA.Submucouslipomaofthe colon.SwissSurg.1998.
5.RodriquezDI,DrehnerDM,BeckDE,McCauleyCE.Colonic lipomaasasourceofmassivehemorrhage.DisColon Rectum.1990;33:977–9.
6.GhidirimG,MishinI,GutsuE,GagauzI,DanchA,RussuS. Giantsubmucosallipomaofthececum:reportofacaseand reviewofliterature.RomJGastroenterol.2005;14:393–6.
7.Nijhawan.Benignanorectaldisorders;1993.
8.BabuKVS,ChowhanAK,YootlaM,ReddyML.Submucous lipomaofsigmoidcolon:arareentity.JLabPhysicians. 2009;1:82–3.
9.KatsinelosP,ChatzimavroudisG,ZavosC,KountourasJ. Endoloop-assistedamputationofalargerectallipoma. GastrointestEndosc.2007;66:636–7.
10.NijhawanS,RaiRR,MathurA,BhargavaN.Rectallipoma treatedbyendoscopicpolypectomy.IndianJGastroenterol. 1993;12:23.
11.YadooS,DintsmanM,ChaimoffC.Lipomaoftherectum.Two casereports.AmJProctol.1971;22:120–2.
12.AminianA,NoaparastM,MirsharifiR,BodaghabadiM, MardanyO,AliFA,etal.Ilealintussusceptionsecondaryto bothlipomaandangiolipoma.CasesJ.2009;2:7099.
13.NebbiaJF,CucchiJM,NovellasS,BertrandS,ChevallierP, BrunetonJN.Lipomasoftherightcolon:reportonsixcases. ClinImaging.2007;31:390–3.
14.MarraB.Intestinalocclusionduetoacoloniclipoma:a propos2cases.MinervaChir.1993;48:1035–9.
15.ManchikalapatiP,LeveyJ.Suspectedasymptomaticlarge colonlipoma:biopsy?Acasereport.PractGastroenterol. 2008;32:35–40.
16.RogyMA,MirzaD,BerlakovichG,WinkelbauerF,RauhsR. Submucouslarge-bowellipomas–presentationand management.EurJSurg.1991;157:51–5.
17.TaylorBA,WolffBG.Coloniclipomas.Reportsoftwounusual casesandreviewoftheMayoClinicexperience,1976–1985. DisColonRectum.1987;30:888–93.
19.CormanML.Colon&rectalsurgery.NewYork: Lippincott-RavenPublishers;1998.
p.884–958.
20.RodriguezDI,DrehnerDM,BeckDE,McCauleyCE.Colonic lipomaasasourceofmassivehemorrhage:reportofacase. DisColonRectum.1990;33:977–9.
21.ZurkirchenMA,LeuteneggerA.Submucouslipomaofthe colon–reportoftwocases.SwissSurg.1998;4:
156–7.
22.HolzheimerRZ,MannickJA.Surgicaltreatment: evidence-basedandproblem-oriented.Munich: Zuckschwerdt;2001.
23.LadurnerR,MussackT,HohenbleicherF,FolwacznyC, SiebeckM,HallfeldK.Laparoscopic-assistedresectionof giantsigmoidlipomaundercolonoscopicguidance.Surg Endosc.2003;17:160.