SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Review
Article
Giant
cell
tumor
locally
advanced
around
the
knee:
treatment
and
literature
review
夽
Ana
Valeria
Rigollino
a,b,∗,
Thiago
Santos
Fernando
a,
Marcos
Hajime
Tanaka
b,
Marcello
Martins
Souza
baHospitaldoServidorPúblicoEstadualdeSãoPaulo,Servic¸odeOrtopediaeTraumatologia,SaoPaulo,SP,Brazil
bHospitaldoServidorPúblicoEstadualdeSãoPaulo,GrupodeOncologiaOrtopédica,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received4June2016 Accepted8July2016 Availableonline27June2017
Keywords: Giantcelltumors Boneneoplasms Kneejoint
a
b
s
t
r
a
c
t
Giantcelltumor(GCT)isabenignbonetumorwithaggressivecharacteristics.Theyare moreprevalentinthethirddecadeoflifeanddemonstrateapreferenceforlocatinginthe epiphysealregionoflongbones.Theyhaveahighlocalrecurrencerate,whichdependson thetypeoftreatmentandinitialtumorpresentation.Theriskoflungmetastasesisaround 3%.
BetweenOctober2010andAugust2014,ninepatientsdiagnosedwithlocallyadvanced GCTorwithpathologicalfracturetothekneelevelunderwentsurgicaltreatment.Theaim ofthisstudywastoevaluatetheresultsofthetreatment,particularlywithregardtorelapse, andtoconductaliteraturereview.
Therewasapredominanceofmales(77.7%).Themostcommonlocationwasthedistal femur.Fourpatients(44%)developedlocalrecurrenceinthefirstyearaftersurgery,three indistalfemurandoneinproximaltibia.Ofthetwopatientswithpathologicfractureat diagnosis,oneofthempresentedrecurrenceafterfivemonths.
ThetreatmentofGCTisstillachallenge.Theauthorsbelievethatthebesttreatment methodiswideresectionandreconstructionofbonedefectswithnon-conventional endo-prostheses.Patientsshouldbeawareandwellinformedaboutthepossiblecomplications andfunctionallossesthatmayoccurasaresultofthesurgicaltreatmentchosenandthe needforfurthersurgeryinthemediumandlongterm.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheHospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.V.Rigollino).
http://dx.doi.org/10.1016/j.rboe.2017.06.009
fêmurdistal.Quatropacientes(44%)apresentaramrecidivalocalnoprimeiroanode pós-operatório,trêsdofêmurdistaleumnatíbiaproximal.Dostrêspacientesqueapresentaram fraturapatológicanomomentododiagnóstico,umdelesapresentourecidivacincomeses apósacirurgia.Otratamentoaindaéumgrandedesafio.Acreditamosqueomelhormétodo de tratamentoéa ressecc¸ãoamplacomreconstruc¸ãoda falhaósseacomendoprótese nãoconvencional.Ospacientesdevemestarcientesebemorientadosquantoàspossíveis complicac¸ões eprejuízosfuncionaisquepodemocorreremdecorrênciadotratamento escolhidoequantoànecessidadedenovasintervenc¸õescirúrgicasemmédioelongoprazo. ©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Giantcelltumor(GCT)isabenignbonetumorwith aggres-sivecharacteristics.Itrepresentsapproximately5%ofprimary bonetumorsandabout15%ofbenignbonetumors.1
Itconsistsofgiantosteoclast-likecellsinterspersedwith a hypercellular and vascularized stroma, which differenti-atesitfromothertumororpseudotumorallesions,suchas chondroblastoma,browntumorofhyperparathyroidism,and aneurysmalbonecyst.2
Itismoreprevalentwithinthethirdandfourthdecadesof life,andismostcommonlylocatedintheepiphysealregionof thelongbones.Themostaffectedareasarethedistalfemur, proximaltibia,anddistalradius.
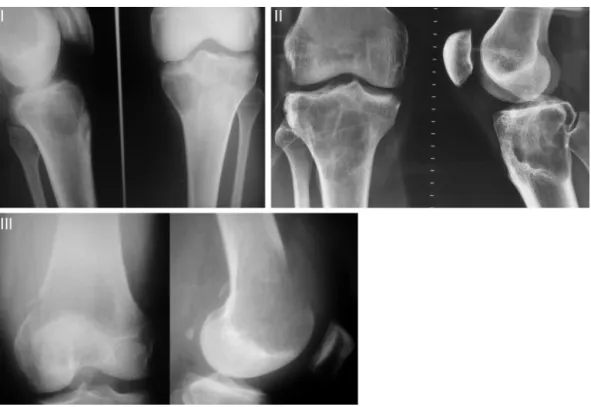
Campanaccietal.3classifiedGCTsintothreetypes accord-ingtotheirbiologicalbehavior,radiographicappearance,and degreeofbonedestruction(Fig.1).TypeIareconsideredlatent andarerepresentedbysmall,intraosseouslesions.TypeIIare
activeandradiographicallylarger,butwithintactperiosteum. TypeIIIareaggressive,extendingthroughouttheperiosteum
andsurroundingtissues.3–5
Surgicaltreatmentisusuallynecessary.Surgeryaimsfor completetumorresection,preservingbonearchitectureand jointfunction,correctionofthedefectcreatedwithtechniques suchasautograft,homograft,arthrodesis,non-conventional endoprostheses,andfillingwithbonecement.6
Intralesionalresectionisusuallythetreatmentofchoicefor CampanacciIandIItumors.1Thisshouldbeaccompaniedby oneormorelocaladjuvantmethods(electrocautery,phenol, liquidnitrogen,argonplasmacoagulation,etc.)inanattempt
todecreasethechanceofrecurrence.2CampanacciIIItumors,
due totheirsizeand localaggressiveness, are usuallybest addressedthroughwideresectionwithdefectcorrection.1,6
Theypresenthighratesoflocalrecurrence,whichdepends on the type of treatment and initial presentation of the tumor.Theriskofsystemicdissemination(lungmetastasis) isapproximately3%.1
Thisstudyassessedninepatientsdiagnosedwithlocally advancedGCTatthekneelevelandtheoutcomeoneyearafter surgery.ThetumorsclassifiedasCampanacciIIIwereincluded
inthisstudy,aswellascasesofpathologicalfracture. Thisstudyaimedtoevaluatetheresultsofthetreatmentof thesepatients,especiallyinrelationtorelapse,andtoreview theliteratureonthetreatmentoflocallyadvancedGCTatthe knee.
Methods
BetweenOctober2010and August2014,ninepatients diag-nosedwithlocallyadvancedGCTattheknee(distalfemurand proximaltibia)underwentsurgicaltreatment.Thediagnosis ofthelesionswithoutfracturewasconfirmedbypercutaneous biopsy using aJamshidi needle.In caseswith pathological fracture, after localstagingand surgery, the diagnosis was confirmedbyhistologicstudy.
Theinclusioncriteriawere:patientsdiagnosedwith Cam-panacci III GCTattheknee or who presentedpathological
Fig.1–Campanacciclassification.
I,quiescent,intraosseouslesions;II,active,withintactperiosteum;III,aggressive,withinvasionofsofttissues.
Table1–Dataofthepatientsselectedforthestudy.
Sex Age Location Fracture Treatment
Patient1 Male 36 Distalfemur No Curettage+cement
Patient2 Male 39 Distalfemur No Curettage+cement
Patient3 Male 29 Distalfemur Yes Curettage+cement
Patient4 Male 32 Distalfemur Yes Curettage+cement
Patient5 Male 35 Distalfemur No Resection+endoprosthesis
Patient6 Male 26 Proximaltibia No Curettage+cement
Patient7 Female 41 Distalfemur No Curettage+cement
Patient8 Male 34 Distalfemur No Curettage+cement
Patient9 Female 32 Proximaltibia Yes Resection+endoprosthesis
Patientswere dividedaccordingtosex,age, tumor loca-tion,presenceofpathologicalfracture,andtypeoftreatment (Table1).
Themostcommonlyusedtreatmentmethodwas curet-tage of the lesion, followed by an adjuvant method with electrocauterization and bone cement, in seven patients. Twopatients underwenten blocresectionofthe lesionand joint replacement using non-conventional endoprosthesis. Forthesepatients, significantbonedestruction withtumor extensiontotheneighboringsofttissueswasobserved,which made any other more conservative method unfeasible. In casesofpathologicalfractureofthedistalfemur,theauthors choseto approach the tumor, performing curettage ofthe lesionwithelectrocauterizationofthetumorcore,reduction ofthedeviatedfragmentswithanatomicalreductionofthe articularsurface, fixation withaspecial plate withlocking screws,andlesioncementation.Forpatientswith patholog-icalfracture ofthe proximal tibia, extensive resectionwas performedwithendoprosthesisreplacement.
Evaluation ofbonedestructionthroughradiographs and magneticresonanceimagingorcomputed tomographywas paramounttodefinesurgicalstrategy.Inpatientswhoselesion didnotallowanatomicalbonereconstruction,resectionand replacementwithendoprosthesiswerechosen,regardlessof thepresenceofapathologicalfracture.
Patientswereevaluatedevery15daysinthefirstmonth, withmonthlyfollow-upappointmentsuptothethirdmonth, and follow-up appointments every threemonths untilone yearofsurgery.Patientswhodidnotpresentrelapseinthe firsttwoyearsaftersurgerywereconsideredcured.However, follow-upisannualforanindefiniteperiod.
Results
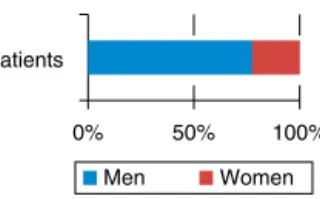
Apredominanceofmaleswasobserved.Outofninepatients evaluated, sevenweremale (77.7%)andtwofemale (22.2%;
Fig.3–Percentageofrecurrencesfoundinthestudyafter oneyear.
0
Distal fêmur Proximal tibia 5
10 7
3
2 1
Total number of patients Recurrence
Fig.4–Locationofthetumorandnumberofrecurrences.
Four patients (44%) developed local recurrence (Fig. 3) withinfirstpostoperativeyear,threeinthedistalfemurand oneinthe proximal tibia(Fig. 4). Ofthe twopatients who presentedapathologicalfracture ofthedistalfemuratthe timeofdiagnosis,onepresentedrecurrencefivemonthsafter surgery.Fig.5showspatient1,whounderwentcurettageof lesionassociatedwithbonecementinthedistalfemur, com-binedwithplatefixation.After11months,patientpresented abonedefectintheposteriorcortexduetotumorgrowth.
Incasesofrecurrence,patients’maincomplaintwas reap-pearance of pain. A new staging with imaging tests was performedtoconfirmrelapse.Inoneofthepatients(patient3), anewcurettageandcementationwereperformed,withgood outcome.Fortheother threepatients,en blocresectionand replacementwithendoprothesiswasperformed(Table2).
Discussion
GCTisconsideredtobeabenignlesion,despiteitspotentialfor localaggression,recurrence,andoccasionallungmetastases.7 Thefrequencyoftheseisapproximately1%–3%,whichcanbe higherincaseswithlocalrecurrence,especiallywhenlocated inthesofttissue.8
Thistumordoesnotremainlatent.Asmalllesiontendsto evolveandleadtotheprogressivedestructionoftheaffected bone.9Therefore,surgicaltreatmentshouldbeindicatedand performedasearlyaspossible.
Curettageassociatedwithanadjuvantmethodhasbeen definedasthepreferredtreatmentformostcasesofGCT.1,10,11 Thisoptionpresentsabetterfunctionaloutcome,butis asso-ciatedwithahigherchanceofrelapse,asevidencedinsome
erenceformoreconservativereconstructionmethodsinthe treatmentoftheselesions,inthehopethatprimaryprocedure willbedefinitive.Theuseofbonecementisawell-established methodthatpresentsgoodlong-termoncologicaland func-tionalresults.Regardingthepossibilityofarthrosissecondary totheuseofbonecement,Baptistaetal.4publisheda retro-spectivestudyof46casesofGCTundergoingcurettageand cementation, concludingthat the distancefrom cementto subchondralbonehasaprognosticrelationshiptothe devel-opmentofosteoarthritis,butnottofinalfunctionaloutcome ofthepatient.
TheincidenceofGCTrecurrencevariesintheliterature. Dahlinetal.14publishedastudywith60%oflocalrecurrence inGCTpatientswhounderwentcurettageandgrafting,and recommendedamoreaggressiveresectionforlocalcontrol. Theuseofmethylmethacrylateassociatedwithcauterization ofthecavityaslocaladjuvantsinthetreatmentofGCT signifi-cantlydecreasedtherateofrecurrence.5Inaliteraturereview, Zhen etal.15 showedvaryingrecurrencerates, from12%to 54%withinsevenyearsoffollow-up(Table3).Klenkeetal.13 observedrecurrenceratesrangingfrom0%to65%,depending onsurgicalmethod.Inthepresentstudy,44%ofrecurrences occurredinthefirstpostoperativeyear,aperiodinwhichthe frequencyofrelapseisgreater.However,unlikeotherstudies, onlylocallyaggressiveCampanacciIIItumorswereincluded
inthepresentstudy.
Baptista11indicatedthatinthepresenceoffractureswith significantdeviation,markeddeformity,orsignificant impair-mentofthreecorticalareas,thesafestprocedureissegment resection,fromboththeoncologicalstandpointandtoreduce morbidity.Thatauthorconcludedthattheapproximate vol-umeoftumor,presenceofcorticalinvolvement,percentageof theepiphysiswidthaffected,anddistancebetweenthelesion borderandthearticularsurfacewerestatisticallysignificant radiographicparametersfortheindicationand/orprognosisof thetreatmentwithcurettageassociatedwith electrocauteri-zationofthelesionwallandfillingwithbonegraft,atechnique assessedinhisstudy.Tumorprognosisisdirectlyrelatedto qualityofthetechniqueofcurettageand/orresectionused, andnotonlytothemethodofreconstructionorfilling.5,6,9
Fig.5–Patient1intheimmediatepost-operativeperiodandintherelapseat11months.
Table2–Dataofpatientswhopresentedrecurrence.
Location Age Sex Monthsuntilrelapse Treatment
Patient1 Distalfemur 36 Male 11 Endoprosthesis
Patient2 Distalfemur 39 Male 9 Endoprosthesis
Patient3 Distalfemur 29 Male 6 Newcurettage
Patient4 Proximaltibia 26 Male 8 Endoprosthesis
Table3–Percentageofrecurrenceinthestudies analyzedbyZehn.
Author Numberof
patients
Recurrence(%)
Dahlin, Crupps,and Johnson
37 41
Goldenberg, Campbell, andBonfiglio
136 54
Larsson, Lorentzon, andBoquist
30 47
Marcoveetal. 52 23
Sungetal. 34 41
McDonald etal.
85 34
Jacobsand Clemency
12 17
Campanacci etal.
151 27
Waldramand Sneath
19 37
O’Donnell etal.
60 25
Blackleyetal. 59 12
reportedthatthree(50%)outofsixpatientswithpathologic fractures evolvedwith recurrence ofthe tumor. They con-cluded that there is a correlation between the occurrence ofpathologicalfracturesandtumorrecurrence.Jesus-Garcia etal.6indicatedthatpathologicalfracturemaybean impor-tant factor in the association with recurrence, sincein its presence,the difficulty inperforming effectivecurettage is
greater. Intheirstudy,oftheeightpatients whopresented recurrence,50%hadapathologicalfracture.
In the present study,conclusionwhether the chanceof tumor recurrence was directly related to the presence of pathologicalfracturewasnotpossible.However,theauthors believethatcontaminationofthesofttissuebythetumor,as isthecaseinCampanacciIIIandpathologicfracture,isarisk
factorfortumorrecurrence.6
Theuseofdenosumabhasshowngoodresultsforthe treat-mentofGCT.ThisdruginhibitstheactionoftheRANKligand, thereforedecreasingtheosteoclasticactivityofthetumor.17 Studies indicate aclinicaland radiological improvementof thetumoraftertreatmentwithsubcutaneousdenosumabat adoseof120mgmonthly,withadditionaldosesonthe8th and15thdayoftreatment,17,18 thusopeninganewhorizon inthetreatmentofthistumor.Thepossibilityofcontrolling thediseaseaftertheuseofthismedicationwouldallowmore conservativesurgeries,withlesschancesofrecurrence.
Limitationsofthepresentstudyincludethesmallnumber ofpatients.GCTisararecondition;accountingforanaverage of5%ofallprimarybenigntumorsofthebone.15Thestudy onlyincluded patientswithCampanacci III GCTand those
with pathological fracture diagnosis, whichfurther limited theselectionofcases.However,fewmulticentricstudieswith large numbers ofpatients were retrieved in the literature. Treatmentmethodsandstatisticalanalysesaredifferentand thereisalackofrandomizedprospectivestudies.
Final
considerations
GCTtreatment(especiallycasesofCampanacciIII)isstillvery
r
e
f
e
r
e
n
c
e
s
1. KlenkeFM,WengerDE,InwardsCY,RosePS,SimFH.Giant celltumorofbone:riskfactorsforrecurrence.ClinOrthop RelatRes.2011;469(2):591–9.
2. MelloGP,SoneharaHA,NetoMA.Endoprótesenãocimentada notratamentodetumordecélulasgigantesdetíbia,18anos deevoluc¸ão.RevBrasOrtop.2010;45(6):612–7.
3. CampanacciM,GiuntiA,OlmiR.Giant-celltumoursofbone: astudyof209caseswithlongtermfollowupin130.ItalJ OrthopTraumatol.1975;1:249–77.
4. BaptistaAM,CamargoAFF,CaieroMT,RebolledoDCS,Correia LFM,CamargoOP.TCG:oqueaconteceuapós10anosde curetagemecimentac¸ão?Estudorestrospectivode46casos. ActaOrtopBras.2014;22(6):308–11.
5. CamargoOPO.Estadodaartenodiagnósticoetratamentodo tumordecélulasgigantes.RevBrasOrtop.2002;37(10):424–9.
6. Jesus-GarciaR,WajchenbergM,JustinoMAF,KorukianM, YshiharaHI,daPonteFM.Tumordecélulasgigantes,análise
12.O’DonnellRJ,SpringfieldDS,MotwaniHK,ReadyJE,Gebhardt MC,MankinHJ.Recurrenceofgiant-celltumorsofthelong bonesaftercurettageandpackingwithcement.JBoneJoint SurgAm.1994;76(12):1827–33.
13.KlenkeFM,WengerDE,InwardsCY,RosePS,SimFH. Recurrentgiantcelltumoroflongbones:analysisofsurgical management.ClinOrthopRelatRes.2011;469(4):1181–7.
14.DahlinDC,CuppsRE,JohnsonEWJr.Giant-celltumor:astudy of195cases.Cancer.1970;25(5):1061–70.
15.ZhenW,YaotianH,SongjianL,GeL,QingliangW.Giant-cell tumourofbone.Thelong-termresultsoftreatmentby curettageandbonegraft.JBoneJointSurgBr.2004;86(2):212–6.
16.McDonaldDJ,SimFH,McLeodRA,DahlinDC.Giant-cell tumorofbone.JBoneJointSurgAm.1986;68(2):235–42.
17.ThomasD,HenshawR,SkubitzK,ChawlaS,StaddonA,Blay JY,etal.Denosumabinpatientswithgiant-celltumourof bone:anopen-label,phase2study.LancetOncol. 2010;11(3):275–80.