w w w . r b o . o r g . b r
Original
article
Surgical
treatment
of
avulsion
fractures
at
the
tibial
insertion
of
the
posterior
cruciate
ligament:
functional
result
夽
Marcos
Alexandre
Barros,
Gabriel
Lopes
de
Faria
Cervone
∗,
André
Luis
Serigatti
Costa
HospitalUniversitáriodeTaubaté,Taubaté,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24September2014 Accepted14November2014 Availableonline23October2015
Keywords:
Bonefractures
Posteriorcruciateligament Knee
a
b
s
t
r
a
c
t
Objective:Toobjectivelyandsubjectivelyevaluatethefunctionalresultfrombeforetoafter
surgeryamongpatientswithadiagnosisofanisolatedavulsionfractureoftheposterior cruciateligamentwhoweretreatedsurgically.
Method:Fivepatientswereevaluatedbymeansofreviewingthemedicalfiles,applyingthe
Lysholmquestionnaire,physicalexaminationandradiologicalexamination.Forthe statis-ticalanalysis,asignificancelevelof0.10and95%confidenceintervalwereused.
Results:AccordingtotheLysholmcriteria,allthepatientswereclassifiedaspoor(<64points)
beforetheoperationandevolvedtoameanof96pointssixmonthsaftertheoperation.We observedthat100%oftheposteriordrawercasesbecamenegative,takingvalueslessthan 5mmtobenegative.
Conclusion: Surgicalmethodswithstablefixationfortreatingavulsionfracturesatthetibial
insertionoftheposteriorcruciateligamentproduceacceptablefunctionalresultsfromthe surgicalandradiologicalpointsofview,withasignificancelevelof0.042.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Tratamento
cirúrgico
da
fratura
avulsão
na
inserc¸ão
tibial
do
ligamento
cruzado
posterior:
resultado
funcional
Palavras-chave:
Fraturasósseas
Ligamentocruzadoposterior Joelho
r
e
s
u
m
o
Objetivo:Avaliaroresultadofuncionalpréepós-cirúrgico,deformaobjetivaesubjetiva,dos
pacientescomdiagnósticodefraturaavulsãoisoladadoligamentocruzadoposteriorque foramtratadoscirurgicamente.
Método:Foramavaliadoscincopacientespormeioderevisãodeprontuários,aplicac¸ãodo
questionáriodeLysholm,examefísicoeexameradiológico.Paraaestatísticafoiusadonível designificânciade0,10eintervalodeconfianc¸ade95%.
夽
WorkperformedintheDepartmentofOrthopedicsandTraumatology,HospitalUniversitáriodeTaubaté,Taubaté,SP,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](G.L.F.Cervone).
http://dx.doi.org/10.1016/j.rboe.2015.09.005
Resultados: SegundooscritériosdeLysholm,todosospacientesforamclassificadoscomo ruins(<64pontos)nopré-operatório,evoluíramparamédiade96pontosemseismeses depós-operatório.Observamosanegativac¸ãode100%dagavetaposterior,umavezque consideramosnegativoovalormenordoque5mm.
Conclusão: A fraturaavulsãodoligamentocruzado posteriornainserc¸ãotibialquando
tratadacommétodoscirúrgicosefixac¸ãoestávelproduzresultadosfuncionaisaceitáveis dopontodevistaclínicoeradiológicoparaumasignificânciade0,042.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Kneeligamentinjuriesarefrequenttopicsofhealth-related research and publications. For some years,studies on the posterior cruciate ligament (PCL) have shared researchers’ attention.Avulsion fractures,which are thesubject ofthis study,areamongtheinjuriestothecruciateligament.
Avulsionfracturesoftheappendicularskeletonare com-monly seen within orthopedicemergency scenarios. Their prevalence is continuing to rise as the population pro-gressively becomes involved in athletic activities1 and car
accidents.2
Avulsionfracturesconsistofdetachmentofabone frag-mentconsequent totractionofaligament,tendonorjoint capsulefromitspointofboneinsertion.1Althoughthistype
ofinjuryisincreasing,it isstillrare,accordingtothe liter-ature, especiallyinjuries to the PCL, whichare sometimes underdiagnosed.3–5AvulsionofthePCLmaybeasmuchas10
timeslessfrequentthanthatoftheanteriorcruciateligament (ACL),eveninchildren.6,7
ThePCLhasanimportantroleinthebiomechanicsofthe kneeandisfundamentaltothestabilityofthisjointbecauseit istheprimaryrestrictorofposteriortranslationofthetibiain relationtothefemur.2,8–11Thecharacteristicsofthefracture,
suchasthesizeanddisplacementofthebonefragment,the regionofthetibiaaffectedandthepatient’sage,areimportant informationinchoosingthetreatmentandmayinfluencethe functionalresult.
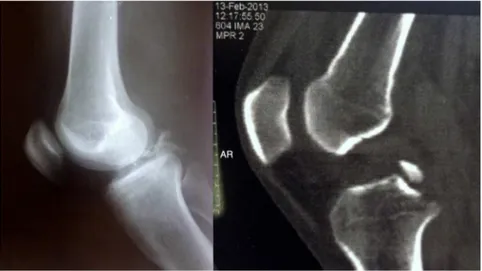
Fig.1–Simpleradiographyandcomputedtomographybeforetheoperation.
Inviewoftheimportanceofthistopic,themainobjective ofthepresent studywas toevaluatethefunctional quality ofkneeswithavulsionfracturesofthePCLbeforeandafter surgicaltreatment,incomparisonwiththeliterature.
Materials
and
methods
Thiswasaretrospectiveobservationalstudyonfivepatients whowereevaluatedinourdepartmentbetweenJanuary2013 andJuly2014.Thisstudyhadpreviouslyundergoneanalysis byourinstitution’sethicscommittee(whichisregisteredwith andapprovedbytheBrazilPlatform)andwasauthorizedby it.
Patientswere onlyincludediftheyhadafinaldiagnosis ofaclosedavulsionfractureofthePCLinisolationthathad been diagnosedbymeans ofsimpleradiography and com-puted tomography (Fig. 1), and if they underwent surgical treatment.Therewerenosexoragerestrictions.Patientswere excludediftheyweretreatedconservatively,presentedlesions withmorethan 30daysofevolution, showed pseudarthro-sis,orhadadiagnosisofintrasubstantialligamentlesionsof thePCLoravulsionfractureoftheanteriorcruciateligament (ACL).
Fig.2–Techniqueusedforradiographyunderstressat80◦ofkneeflexion,using49NontheATTandradiologicalimage.
thesumofthepointsobtainedattheendofthequestionnaire, incomparingthesituationsbeforeandaftertheoperation.6
Theposteriordrawertestwasconsideredtobepositiveor negativeincomparisonwiththeclinicalstateofthe contralat-eralknee,inthepresenceorabsenceofastop,respectively.
Fortheradiographyunderstress,inlateralview,weused patientsinhorizontaldorsaldecubitus,withthelimbat80◦,
supportedonly in the heel region, and a force of 49N(N) appliedtotheregionoftheanteriortibialtuberosity (ATT). Followingthis,theposteriortranslationofthetibiainrelation tothefemurwasquantifiedusingaruler:itwasconsidered tobenegativeorzerowhenthedisplacementwaslessthan 4mmandwasgradedasonecross(+)if5–9mmandastwo crosses(++)ifgreaterthanorequalto10mm,incomparison witheachindividual’scontralaterallimb(Fig.2).8–10,12
Thefollowing informationinherentto the surgical pro-cedurewasgatheredfromthemedicalfiles:durationofthe operation,osteosynthesisandthesurgicalaccessrouteused. The following complementary information was also gath-ered:timeelapsedbetweeninjuryandtreatment,associated lesions, trauma mechanism, age and sex of the patients (Table1).
Allthepatientswerepositionedinhorizontalventral decu-bitus,spinalanesthesiawasapplied,apneumatictourniquet was usedattherootofthe thighthatwas tobeoperated, andaposteriorapproachtotheknee wasusedatthelevel ofthepoplitealfossa.Trickey’sroute13(inSshape)wasused
onthreepatientsand,fortheothertwo,itwasdecidedtouse areducedincision asdescribedbyBurksandSchaffer14(in
aninvertedLshape),asillustratedinFigs.3and4.Afterthe incisionhadbeenmade,dissectionwasperformedinlayers andthevascular-nervebundlebetweenthemedialandlateral gastrocnemiusmuscleswasidentifiedandcarefullypushed away.Centralandposteriorarthrotomywereperformed,with identificationofthebonefragmentavulsedfromitstibialbed. Noneofthebonefragmentsweresmallenoughtoimpede fixationwithrigidmaterial,whichwouldhaverequired tran-sosseoussuturingorbinding.Inthesefivecases,theprinciples ofabsolutestability,anatomicalreductionandcompression ofthefracturefocuswithrigidsynthesis(oneormorescrews withwashers)wereused,ascanbeseeninFig.5.Werespected thegrowthplateevenincasesofsmallfragments.
During the postoperative period, a plaster-cast splint extendingfromthethightothemalleoluswasused,without
Table1–Datarelatingtothedescriptionofthecases:sex,age,injurymechanism,presenceofinjuryontheanterior face,durationofthesurgery,timeelapsedsinceinjury,preandpostoperativerangeofmotion,sideinjured,Lysholm result,radiographunderstress,incisionandcomplications.
Patient 01 02 03 04 05
Sex M M M M M
Age(years) 21 15 46 31 48
Injurymechanism Motorcycle Bicycle Motorcycle Motorcycle Motorcycle
Injuryonanteriorface (lowerlegorknee)
Yes No Yes Yes No
Durationofoperation (inminutes)
40 35 55 40 30
Timeelapsedbetween injuryandsurgery(in days)
22 06 07 21 16
Postoperativerangeof motion–flexion (right/left)
125◦/145◦ 130◦/120◦ 140◦/140◦ 135◦/135◦ 145◦/135◦
Preoperativerangeof motion–flexion (right/left)
Lockedat 40◦/preservedat 145◦
Preservedat 130◦/lockedat 10◦
Lockedat 20◦/preservedat 140◦
Preservedat 135◦/lockedat 15◦
Preservedat 145◦/lockedat 20◦
Kneeinjured Right Left Right Left Left
Lysholmquestionnaire (before/after) Poor(0)/Excellent (95) Poor (25)/Excellent(99) Poor (27)/Excellent(97) Poor (25)/Excellent(95)
Poor(2)/Good(94)
Relativedistances tibia–femuron radiographunder stress(right/left),in millimeters
3/0 0/1 2/0 0/2 0/1
Skinincision Trickey Trickey Trickey Burks Burks
Postoperative complications
None None Dehiscenceof
suture
None None
weight-bearing.Thepatientsreturnedtotheoutpatientclinic inthesecondweekforthestitchestoberemovedandforthe plastercasttobeexchangedforabrace,soastoallowthe startofpassivemobilizationandcryotherapy.Afteronemonth hadbeencompleted,aradiographiccontrolwasperformedin ordertoprogressivelyreleasethepatientsforweight-bearing anddefinitiveremovaloftheimmobilization.Fromthe
sec-ondmonthonwards,thepatientswereauthorizedtobegin
theworkofmusclestrengthening.Inthethirdmonth,they
40%
60%
Burks
Distribution of skin incisions
Trickey
Fig.4–Illustrationofthedistributionoftheincisioninthe skin.
returnedtoworkandinthesixthmonth,afteraclinicaland radiologicalreevaluation,theyweregivenamedicaldischarge.
ThestatisticalmethodologycomprisedtheWilcoxontest
withasignificancelevelof0.10and95%confidenceinterval.
Results
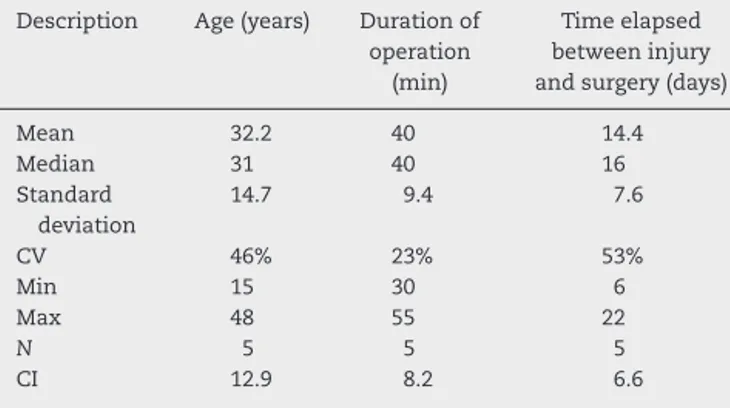
Westartedtheresultsbydoingacompletedescriptiveanalysis accordingtoage,durationofthesurgicalprocedureandthe timeelapsedbetweeninjuryandsurgery(Table2).Itshould benotedthat100%ofthepatientsweremale.
Table2–Completedescriptionforage,durationof operationandtimeelapsedfrominjurytosurgery. Description Age(years) Durationof
operation (min)
Timeelapsed betweeninjury andsurgery(days)
Mean 32.2 40 14.4
Median 31 40 16
Standard deviation
14.7 9.4 7.6
CV 46% 23% 53%
Min 15 30 6
Max 48 55 22
N 5 5 5
CI 12.9 8.2 6.6
Fig.5–Radiographyofsynthesisinanadolescent,parallel tothegrowthplate,thuspreservingit.
TheWilcoxon methodallowedustoconsiderthat there wasastatisticallysignificant difference (p=0.042)from the Lysholmresultbeforethesurgery,of15.8points(poor),toan averageof96points(excellent).Therewasasinglecaseofa goodresult(94points)afterthesurgery,inwhichthepatient lost one point (out of fivepoints) in relation tosquatting, becauseofslightasymmetrywhenflexedforsquatting(10◦),
incomparisonwiththecontralaterallimb(Fig.6andTable3). Acomparisonwasmadewiththemeanposterior transla-tionofthetibiainrelationtothefemuronradiographsunder stress,withthreereferencevaluesinmillimeters(zero,one
Comparison between times for applying lysholm
120
100
80
60
40
20
Mean
Before After
15.8
96
0
Fig.6–IllustrationcomparingtimesforapplyingLysholm.
Table3–ComparisonbetweentimeswhenLysholmwas applied.
Lysholm Before After
Mean 15.8 96
Median 25 95
Standarddeviation 13.6 2
Min 0 94
Max 27 99
N 5 5
CI 11.9 1.8
pvalue 0.042
CV,coefficientofvariation;Min,minimumvalue;Max,maximum value;N,samplesize;CI,confidenceinterval.
Table4–Comparisonbetweenradiographunderstress andreferencevalues.
Radiographunderstress
Mean 1.80
Median 2
Standarddeviation 0.84
Min 1
Max 3
N 5
CI 0.73
pvalue(0) 0.009
pvalue(2.5) 0.621
pvalue(5) 0.001
CV,coefficientofvariation;Min,minimumvalue;Max,maximum value;N,samplesize;CI,confidenceinterval.
Table5–Distributionoftheinjurymechanism.
Injurymechanism N % pvalue
Motorcycle 4 80% 0.058
Bicycle 1 20%
andfive),giventhatallcaseswereatthelimitforzerocrosses ornegative(Table4).
Wefoundthatthemeanforradiographsunderstresswas 1.80mmandthatthismeanwasstatisticallydifferencefrom zeroandfromfive,butwasconsideredtobeequaltothevalue of2.50andlessthan5mm,whichisthevalueforonecross (+)ofposteriortranslationofthetibiainrelationtothefemur, whichwouldindicatesomedegreeofinstabilityofthejoint (Table4).
We also concludedthat there were significant different with regard to the distribution of postoperative complica-tions,injurymechanism(Table5)and posteriordrawertest (Table6).Regardingpostoperativecomplications,80%didnot presentany,while20%presentedcomplications,andthiswas asignificantdifference(p=0.058).Thecomplicationobserved
Table6–Distributionofthedrawertest.
Drawertest N % pvalue
Negative 5 100% 0.002
wasdehiscenceoftheskin,whichevolvedwellandwithout anyinfectionbeforehealing.Neithersidewasmore predom-inantlyaffected(0.527;non-significant).
Whenasked,100%ofthepatientsstatedthattheywere satisfiedwith thefunctional resultfor theirknee afterthe treatment. None of them had sequelae or symptoms that causedanylimitationsorincapacityinrelationtotheir phys-ical, professional and daily activities. Even in one of the cases,inwhichthepatientwasaprofessionalwithin athlet-icsandaphysicaleducationteacher,therewasnoresidual incapacitatinglimitation.Thispatientisnowparticipatingin competitionsatprofessionallevel.
Discussion
Posteriorcruciateligamentinjuriesareuncommonand,when they occur, they are generally combined with other knee ligamentinjuries.InjuriestothePCLaloneaccountfor approx-imately3%ofacutekneeinjuries.9
Someauthors have reporteda mean incidenceof three casesofavulsionfracturesoftheACLper 100,000andthat casesofavulsionofthePCLareevenrarer,possiblyasmuch astentimeslessfrequent,eveninchildren.6,7
ThePCListhestrongestofthecruciateligamentsandisthe primaryrestrictorofposteriortranslationofthetibiaduring kneeflexion.Whenitisinjured,posteriorsubluxationoccurs andthiscauseschangestothepressureinthefemoropatellar joint,withconsequentchronicpainanddegenerationofthe jointcartilage.8,15
Previousstudies8,9observedthattheposteriortranslation
ofthetibiaisgreaterwithincreasingdegreesofkneeflexionon radiographsunderstress,at10◦,20◦,60◦and80◦.Stäubliand
Jakob8agreedthatthenormalposteriordeviationin
millime-terswasonaverage3.7±2.1ontheintactsideand10.4±2.4 wheninjured (significance ofp<0.001).8,9 This information
ensuresgreatercredibilityforourobjectiveevaluationof func-tionusingradiographsunderstressat80◦.
Althoughthereisstillnoconsensusregardingtheprimary repairinPCLinjuries,itisnowclearthatthebestresultsin casesofavulsionfracturesareobtainedafterstablefixation. Serial studies have consistently demonstrated satisfactory resultsthroughfixation,anduniformlypoorresultsfrom non-surgicalmethods.6,8,13,16,17
The commonest injury mechanism is motorcycle
acci-dents,followedbyinjuryagainstthepanelandbeingrunover, amongothers.3,17 Weobservedthattherewasonecaseofa
bicycleaccident,whilealltheothersinvolvedmotorcyclists (Table5).Inaround90◦ofthecases,theinjuryiscausedbyan
impactontheanteriorfaceoftheflexedknee.Insomecases, injurytotheanteriorregionoftheknee ispresent,suchas lacerationsorcutting-bruisingskinwounds(observedin60% ofthecasesinthisstudy),asillustratedinFigs.7and8.Other injuriesmaybeassociatedwiththese,suchasfracturesofthe patella,ipsilateralfemur,carpalbonesorribarches.3
Independentoftheroute,techniqueormaterialused, avul-sion fractures of the PCL should be treated surgically, as suggestedbyVeselkoandSaciri16andbyothers.2,3,17Thebest
techniquetoapply isstillamatterunderdiscussion, butit shouldbetheonewithwhichthespecialistsurgeonismost
40%
60%
No
Distribution of lesions on anterior face
Yes
Fig.7–Illustrationofthelesiondistributionontheanterior face.
Fig.8–Imageofextensivecutting-bruisingwoundand suturingintheanteriorregionofthelowerleg.
familiarorforwhichtheconditionsandstructurefor apply-ingitarethebest,6,8,12,13,16,17giventhatthearthroscopicand
opentechniquesareequallyreliable.18
Conclusion
andobjectivelysatisfactoryresults,withcompletefunctional restoration.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WhiteEA,PatelDB,MatcukGR,ForresterDM,LundquistRB, HatchGF3rd,etal.Cruciateligamentavulsionfractures: anatomy,biomechanics,injurypatterns,andapproachto management.EmergRadiol.2013;20(5):429–40.
2. SinglaR,Devgan,GognaP,BatraA.Fixationofdelayedunion ornon-unionposteriorcruciateligamentavulsionfractures.J OrthopSci.2014;22(1):70–4.
3. TorisuT.Avulsionfracturestothetibialattachmentofthe posteriorcruciateligament:indicationsandresultsof delayedrepair.ClinOrthopRelatRes.1979;143:107–14.
4. Al-AhaidebA.Posteriorcruciateligamentavulsionfracturein children:acasereportwithlong-termfollow-upand comprehensiveliteraturereview.EurJOrthopSurg Traumatol.2013;23Suppl.2:S257–60.
5. PiedadeSR,MischanMM.Tratamentocirúrgicoda fratura-avulsãodainserc¸ãotibialdoLCPdojoelho: experiênciade21casos.ActaOrtopBras.2007;15(5):272–5.
6. PeccinMS,CiconelliR,CohenM.Questionárioespecíficopara sintomasdojoelhoLysholmKneeScoringScale:traduc¸ãoe validac¸ãoparaalínguaportuguesa.ActaOrtopBras. 2006;14(5):268–72.
7. DhillonMS,SinghHP,NagiON.Posteriorcruciateligament avulsionfromthetibia:fixationbyaposteromedialapproach. ActaOrthopBelg.2003;69(2):162–7.
8.StäubliHU,JakobRP.Posteriorinstabilityofthekneenear extension.Aclinicalandstressradiographicanalysisofacute injuriesoftheposteriorcruciateligament.JBoneJointSurg Br.1990;72(2):225–30.
9.GroodES,StowersSF,NoyesFR.Limitsofmovementinthe humanknee.Effectofsectioningtheposteriorcruciate ligamentandposterolateralstructures.JBoneJointSurgAm. 1988;70(1):88–97.
10.LeãoMGS,SantoroES,AvelinoRL,GranjeiroRC,Orlando JuniorN.Fraturaavulsãosimultâneadasinserc¸õestibiaisdos ligamentoscruzadosanterioreposterioremadulto.RevBras Ortop.2013;48(6):581–5.
11.CanaleST,BeattyJH,editors.Campbell’soperative orthopaedics.11thed.Philadelphia:MosbyElsevier;2007.
12.ScottMD,NormanW.Surgeryoftheknee.5thed. Philadelphia:Mosby/Elsevier;2012.
13.TrickeyEL.Injuriesoftheposteriorcruciateligament: diagnosisandtreatmentofearlyinjuriesandreconstruction oflateinstability.ClinOrthopRelatRes.1980;147:
76–81.
14.BurksRT,SchafferJJ.Asimplifiedapproachtothetibial attachmentoftheposteriorcruciateligament.ClinOrthop RelatRes.1990;254:216–9.
15.JohnsonD.Posteriorcruciateligamentinjuries:myapproach. OperTechSportsMed.2009;17:167–74.
16.VeselkoM,SaciriV.Posteriorapproachforarthroscopic reductionandantegradefixationofavulsionfractureofthe posteriorcruciateligamentfromthetibiawithcannulated screwandwasher.Arthroscopy.2003;19(8):916–21.
17.SchulteKR,HarnerCD.Managementofisolatedposterior cruciateligamentinjuries.OperTechOrthop.1995;5(3): 270–5.
18.SasakiSU,daMotaeAlbuquerqueRF,AmatuzziMM,Pereira CA.Openscrewfixationversusarthroscopicsuturefixationof tibialposteriorcruciateligamentavulsioninjuries:a