SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Posterior
three-column
osteotomies
for
the
treatment
of
rigid
thoracic
kyphosis
–
a
case
series
夽
Marcelo
Simoni
Simões,
Ernani
Vianna
de
Abreu,
Bruno
Costamilan
Winkler
∗HospitalErnestoDornelles,PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16December2015 Accepted31May2016
Availableonline24January2017
Keywords:
Osteotomy Kyphosis Spinalcurvatures Spinaldiseases
a
b
s
t
r
a
c
t
Objective:Toevaluatetheresultsandcomplicationsofaseriesofpatientswhounderwent three-columnosteotomyusingtheposteriorapproachforcorrectionofcomplexcasesof rigiddorsalkyphoticdeformity.
Methods:Reviewofclinicalrecordsandimagesof15consecutivecasesofpedicle subtrac-tionosteotomies,bone-disk-boneosteotomies,orvertebralcolumnresection,recordingthe etiology,typeandlevelofosteotomy,extensionoffixation,complications,andpre-and post-surgicalmeasurementsofthesagittalcurvesandpelvicparameters.
Results:Sixpediclesubtractionosteotomieswereperformed,oneofwhichintwoadjacent vertebrae,aswellastwobone-disk-boneosteotomiesandsevenvertebralcolumnresection, twoofwhichwereperformedintwoadjacentvertebrae.Themeancorrectionwas39.3◦for
theangularkyphosisand33.9◦fordorsalkyphosis.Thecorrectionsweresimilarregardless
ofthekindofosteotomy,theoperatedspinalsegment,ortheapproachinoneortwolevels, butthismaybeasampleeffect.
Eightcomplicationswereobservedinsixpatients(40%ofcases):twomedical complica-tions,fiveearlyandonelatesurgicalcomplication(over90daysaftersurgery).Therewere threereoperationswithinlessthanoneyearfromtheinitialsurgeryandonecaseof per-sistentparaparesis.Clinicalcomplicationswereresolvedwithoutsequelae.Therewasno significantlossofcorrectionduringthesegment,exceptintwocasesofmajormechanical failureduetoajunctionalsegmentfracture.
Conclusion: Despitebeingcomplexandaggressiveprocedures,pronetovarious complica-tions,osteotomieswithresectionofthethreecolumnsarehighlyeffectiveinthecorrection ofrigidkyphoticdeformitiesandsafeenoughtojustifyitsuseinselectedcases.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalErnestoDornelles,PortoAlegre,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](B.C.Winkler).
http://dx.doi.org/10.1016/j.rboe.2017.01.004
190
rev bras ortop.2017;52(2):189–196Osteotomias
posteriores
de
três
colunas
para
tratamento
de
cifose
dorsal
rígida
–
Série
de
casos
Palavras-chave:
Osteotomia Cifose
Curvaturasdacolunavertebral Doenc¸asdacolunavertebral
r
e
s
u
m
o
Objetivo: Avaliarosresultadoseascomplicac¸õesdeumasériedepacientessubmetidosa osteotomiasdastrêscolunasporabordagemposteriorparacorrec¸ãodecasoscomplexos dedeformidadecifóticadorsalrígida.
Métodos: Revisãodosprontuáriosedasimagensde15casosconsecutivosdeosteotomias desubtrac¸ãopedicular,osteotomiasosso-disco-ossoouvertebrectomiasposteriorestotais, comregistrodasetiologias,tipoeníveldeosteotomia,extensãodafixac¸ão,complicac¸õese medidaspré-epós-cirúrgicasdascurvassagitaisedosparâmetrospélvicos.
Resultados: Foramfeitasseisosteotomiasdesubtrac¸ãopedicular,umaemduasvértebras adjacenteseduasosso-disco-ossoesetevertebrectomiasposteriorestotais,duasemduas vértebrasadjacentes.Asmédiasdecorrec¸ãoforamde39,3◦paraacifoseangulare33,9◦
paraacifosedorsaltotal.Ascorrec¸õesforamsemelhantes,independentementedotipode osteotomiausado,dosegmentoespinhaloperadooudaabordagememumoudoisníveis, masissopodeserefeitodaamostra.
Ocorreramoitocomplicac¸õesemseispacientes(40%doscasos),duasclínicas,cinco cirúgi-casprecoceseumacirúrgicatardia(maisde90diasapósacirurgia).Houvetrêsreoperac¸ões commenosdeumanodacirurgiainicialeumcasodeparaparesiamantida.Ascomplicac¸ões clínicasforamresolvidassemsequelasmaiores.Nãohouveperdadecorrec¸ãosignificativa duranteosegmento,excetoemdoiscasosdefalhamecânicamaiorporfraturadesegmento juncional.
Conclusão:Emborasejamprocedimentoscomplexos,agressivosesujeitosacomplicac¸ões,as osteotomiascomressecc¸ãodastrêscolunassãoaltamenteeficazesnacorrec¸ãodas deformi-dadescifóticasrígidasesegurasobastanteparajustificarseuusoemcasosselecionados.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Thedevelopmentofspinalsurgeryhasledsurgeonstoface increasinglycomplexcases,aimingnotonlyatspinal decom-pressionandstabilization,butalsoatdeformitiescorrection andthespinebiomechanicalbalancerestoration.1
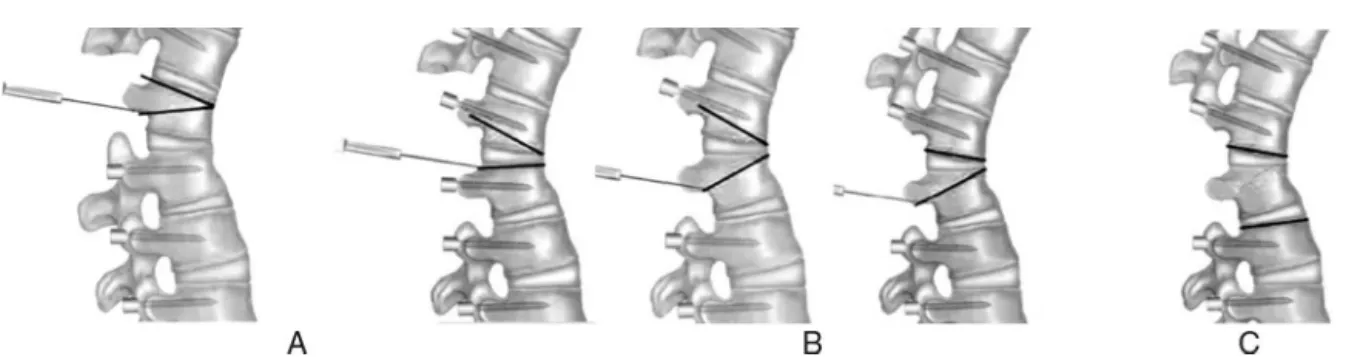
Inthelastdecade,subtractionosteotomieshavebecome popularinthemanagementofspinaldeformities2,3andhave beguntobeusedinawiderangeofsituations.Thefocuses ofthisstudyarepedicularsubtractionosteotomy(PSO), bone-disk-boneosteotomy(BDB),andvertebral columnresection (VCR),allofwhichareposterior,middle,andanteriorresection techniquesthroughasingleposterioraccessthatcanbeused invery rigiddeformities,withthree-column arthrodesisor ankylosis,providingsignificantangularcorrectionsinasingle levelwithoutelongationoftheanteriorcolumnofthespine (Fig.1).
Material
and
methods
Thiswasaretrospectivestudyof15casesofpatientswithrigid dorsalkyphoticorkyphoscolioticdeformitiesofseveral etiolo-gies,surgicallytreated,whosepostoperativefollow-upranged from6to60months(meanof36months).Datafromcharts and measurements of spine curves were collected by the
four-lineCobb method. Lumbar lordosisand dorsal kypho-sis were measured betweenthe points of inversionof the curve,regardlessofthelevel(Fig.2).Incaseswheremorethan onesurgerywasperformed,resultsconsideredmeasurements takenafterthelastapproach.
Surgicaltechnique
Fig.1–Typesofthree-columnosteotomy.(A)Pedicularsubtractionosteotomy(PSO);resectionofavertebralbodywedge.
(B)Bone-disk-boneosteotomies(BDB);resectionofawedgewiththeapexonthedisk.(C)Vertebralcolumnresection(VCR);
resectionoftheentirevertebralbodywiththedisksaboveandbelow.
Results
Sampledata
Five men and ten women, agedbetween 13 and 66 years (mean:38,SD=±18.8),wereoperated.Therewerefourcases ofpost-traumatickyphosis(26.6%),fourcasesof kyphoscolio-sisduetohemivertebrae(26.6%),twocasesofPott’sdisease (13.3%), twocases ofjunctionalkyphosis (13.3%), one case of deformity after pathological fracture due to multiple
myeloma,onecaseofkyphoscoliosisdueto neurofibromato-sis,andonecaseofrigidScheuermann’skyphosisinanadult patient. Onlythe twopatientswithjunctionalkyphosis, in whomalongfixationofthelumbosacralspinewasobserved, presentedsignificantsagittalimbalance.Forallothercases, eveninthepresenceofsignificantkyphosis,overallsagittal balancewasmaintainedattheexpenseofcompensatory lum-barhyperlordosisandpelvicanteversion.
Nineofthe15casespresentedverysignificantspinalcord compression, but there were onlytwo cases of neurologi-cal compressive deficits (case 1, Pott’s disease and case 8,
Fig.2–Methodoftakingmeasurementsofangularkyphosis(AK),sacralslope(SS),pelvicincidence(PI),dorsalkyphosis
192
rev bras ortop.2017;52(2):189–196post-neoplastic).Incase5,paraplegia wascausedbyacute trauma,notbylatedeformity.
Thefollowingprocedureswereperformed:sixPSOs(40%), oneofwhichoccurredintwoadjacentvertebrae(case6);two BDBs (13.3%); and seven VCRs (46.7%), two of which were conducted in two adjacent vertebrae (cases 1 and 2). One osteotomywasperformedintheproximalthoracicsegment (T2–T4),seven(46.7%)inthemiddlethoracicsegment(T5–T9), andseven(46.7%)inthelowerthoracicsegment(T10–T12).
DataaresummarizedinTable1.
Surgicalresults
Themeanangularkyphosiscorrectionwas39.3◦(SD=±14.6◦)
andtotalkyphosis33.9◦ (SD=±17.7◦).Consideringthe
oper-ated segment, angular kyphosis correction and full dorsal kyphosiswere,respectively,33◦and22◦inupperdorsallesions
(T2–T4),41.1◦(SD=
±13◦)and35◦(SD=
±21.3◦)inmedialdorsal
lesions(T5–T9),and38.3◦(SD=±17.7◦)and34.4◦(SD=±15.9◦)
in lower dorsal lesions (T10–T12). Considering the type of osteotomyused,thecorrectionofangularkyphosisachieved byBDBwas28◦(26◦and30◦);byPSO,41.5◦(29–53◦,SD=
±9.4◦);
andbyPTV,42◦ (10–63◦,SD=
±19.5◦).Completeneurological
recoverywasobservedinthetwocasesthatpresented para-paresisduetodeformity.
Complications
Eight complications occurred in six patients, as shown in
Table2.Theclinicalcomplicationswereapulmonary throm-boembolism and a thyroid storm in ayoung woman with hypothyroidismwhodiscontinuedthemedicationonherown. Bothcaseswereresolvedwithoutmajorsequelae.
In the case of neurofibromatosis, there was a partial medullarylesionduringvertebrectomy,whichwasperformed viathetransduralaccess,sincethemeningocelesembraced theentirecontourofthevertebra.Patientpresentedleft dor-salparesisinthepostoperativeperiod,compatiblewithgait, andwithprogressiveimprovement.However,sevenmonths aftersurgery,patientreturnedwithseverespastic parapare-sis.Investigationshowedsignificantspinalcordcompression byanarachnoidcystabovetheoperatedarea,probablydueto arachnoidadhesionsafterthetransduralapproach. Further surgerywasperformed,butpatientremainedparapareticand spastic(case9,Fig.3).Therewerethreeearlymechanical com-plications,oneinstrumentationfailure(case8,Fig.4),andtwo junctionalfracturesatthemostcaudalinstrumentedlevel, withasmalllossofcorrectioninoneandimportantlossin another,whichledtothedecompensationofthesagittal bal-ance(case11,Fig.5).Asignificantlossofcorrectionwasnot observedinanyoftheothercasesduringfollow-up.
Discussion
Three-columnosteotomiesare aggressivesurgeries,usually indicatedinsituationsinwhichothertechniqueswithlower potentialmorbidityarenotapplicable,eitherduetolackof flexibilityofthespineorthepresenceofseverefocalangular deformity.2Itsprimaryadvantageistoallowthecorrectionof
rigiddeformitieswithouttheneedforanteriorrelease.PSOis thebestknowntechnique;somepublicationshavedescribed againof30to40degreesoflordosisperleveladdressed.4–6 Inthedorsalspine,itsusehasbeenmuchmorelimitedand thepotentialforcorrectionisnotsoclear.7In1994,Lehmer etal.8reportedfourcasesoperatedinthelowerdorsalspine, with amean correction of29.5 degrees. Bridwell2 reported gainsofapproximately25degrees.WiththeuseoftheVCR inthe dorsalspine,Rajasekaranet al.9 reportedameanof 36degreesofcorrectionincasesoftuberculosis,while Shi-modeetal.5reportedameancorrectionof56degreesinsevere kyphoscoliosis. In the present series, the corrections were ofapproximately 40 degrees,with nosignificant difference betweentechniques.
Thoracicosteotomiesdiffergreatlyfromthoseofthe lum-bar.First,toallowaneffectiveclosureoftheosteotomy,the ribsthatarticulatewiththesuperiorandinferiordisksmustbe released;second,becausethesurgeryisdoneatlevelswhere thereisbonemarrow,thereisalimittothebone mobiliza-tionthatcanbeachievedwithacceptablerisk.O’Shaughnessy et al.7 reportedthat20–25mmofposteriorlaminar closure canbetoleratedwithoutneurologicalproblems,butthisvalue hasnotbeenvalidatedexperimentally.Tomitahasshownthat spinalcordshorteningassociatedwiththeremovalofa ver-tebralbody isnotaproblem, andneitheristhe ligationof segmental vessels in up tothree levels.10,11 Gertzbein and Harris12postulatedthatdistortionofthecordandclamping oftheduralsacarepotentialrisksassociatedwithspinalcord shortening; theseauthors recommend avoidingcorrections ofmorethan40◦.Inthepresent series,resectionsofupto
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
7;
5
2(2)
:189–196
193
Case G-A Etiology PS Deficitpre AKpre PI SVApre DKpre LLpre SSpre LOP LFIX TOS AKpost SVApost DKpost LLpost SSpost CorK
1 M-28 PostTBC 0 Paraparesis 60 60 4 52 48 36 T8+T9 T5–T12 VPC 21 2 33 40 31 39
2 M-48 PostTBC 0 105 59 6 82 46 40 T5+T6 T2–T10 VPC 42 4 44 40 38 63
3 F-54 PTD+Infection 5 33 55 6.5 51 47 30 T12 T8–L3 VPC 4 5.5 43 50 30 29
4 M-16 Congenital 0 78 66 −3 73 90 49 T11 T7–L2 VPC 20 2 43 70 45 58
5a F-27 PostPTD 0 Paraplegia 33 50 0 68 40 0 T11-T12 T9–L3 BDB 3 −3 42 52 15 30
6 F-62 PostPTD 0 54 42 4.5 75 58 33 T8+T9 T5–T12 PSO 15 1 62 62 35 39
7 M-13 Congenital 0 63 42 3 90 90 40 T11 T8–L2 VPC 28 1 33 38 23 35
8 F-63 PostNeo 0 Paraparesis 70 60 5 72 50 30 T3 C2–T7 PSO 37 0 50 66 40 33
9 F-20 Dysplastic 0 90 50 1 126 78 38 T11 T8-L4 VPC 30 0 70 70 42 60
10 F-22 Congenital 0 42 68 −4.5 70 90 45 T7-T8 T2–L1 BDB 16 −2 44 70 50 26
11 F-66 Junctional 2 45 54 8.5 75 49 27 T9 T2–L3 PSO 16 6 44 49 30 31
12 F-37 Scheuermann 0 60 53 1.5 73 78 35 T11 T4–L3 PSO 14 0 40 60 35 46
13 M-17 CEH 0 30 64 −1 73 90 45 T10 T8–L3 VPC 20 0.5 52 70 39 10
14 F-48 PostPTD 1 63 60 0 108 89 36 T8+T9 T2–L2 PSO 14 −6 34 60 42 74
15 F-50 Junctional 1 75 66 36 106 50 47 T7 T2–IL PSO 22 8 66 74 45 53
AKpre,preoperativeangularkyphosis(degrees);AKpost,postoperativeangularkyphosis(degrees);DKpre,totalpreoperativedorsalkyphosis(degrees);DKpost,postoperativedorsalkyphosis (degrees);CorAK,correctionofangularkyphosis(degrees);PS,numberofprevioussurgeries;SVApre,preoperativesagittalverticalaxis(centimeters);SVApost,postoperativesagittalverticalaxis (centimeters);IL,sacralandiliacfixation;PI,pelvicincidence;SSpre,preoperativesacralslope(degrees);SSpost,postoperativesacralslope(degrees);LLpre,preoperativelumbarlordosis(degrees); LLpost,post-operativelumbarlordosis(degrees);NEO,deformityafterboneneoplasia;LFIX,fixatedlevels;LOP,levelatwhichtheosteotomywasperformed;G-A,gender-age;TOS,osteotomytype; PTD,posttraumaticdeformity.
194
rev bras ortop.2017;52(2):189–196Table2–Complications.
Case Earlyclinical Earlysurgical Surgicalprocedures Reoperations Sequelae
03 Deepinfection Surgicaldressing
06 T12fracture Lossofcorrection
08 Cervicalpullout Revisionofthefixation
09 Spinalcordinjury Arachnoidcyst Cystresection Spasticparaparesis
10 Thyroidcrisis
11 TEP L4fracture Lossofcorrection
cases.The recommended approachis tomaintaina mean arterialpressureofatleast75mHg,loosenthecorrectionand, if thepotentials donotrestore, then removethe rodsand undothecorrection,attemptingagainwithanotherstrategy aftersignalsarerestored.15Neurologicaldeficitinthepresent serieswasnotrelatedtothecorrectionofthedeformity,but ratheroccurredduringboneresectionperformedvia transdu-ralaccessinthecaseofneurofibromatosis,whilethepatient was being monitored. Mechanical complications are more commonthanneurologicalones,sincekyphoticdeformities haveanaturaltendencytoprogressionandinstrumentation overloadisnotuncommon,especiallywhensagittalbalance isnot corrected. In some cases, the patient appearsto be used tothe anterior position ofthe trunkand the projec-tionofthehead,andassumesthistypeofpostureevenafter correctionofthedeformity,whichsuggeststheexistenceof someneurologicalorproprioceptivemechanism that influ-encestheindividualabilitytomaintainthebodybalance.6The mostdescribedmechanical complicationsare pseudarthro-sis, failure of instrumentation, and loss ofcorrection over time.Intheliterature,theincidenceofpseudarthrosisranges from0to5%5,18,19 andinstrumentationfailuresoccurinup to8%ofthe cases, generallyrelated toinsufficient correc-tion,osteoporosis,orlackofanteriorsupportinVCR.7,9,19In thepresentseries,therewerenocasesofpseudarthrosis,and
onlyonepatientwasfollowed-upforlessthanayear.Three earlymechanicalcomplicationswere observed:onecasein whichscrewspulledout(case8,Fig.4)andtwofracturesof theinstrumentedlowervertebra,bothrelatedto osteoporo-sis.ThefirstcasewasafixationfromT5toT12,andfracture occurred due toinsufficiency in T12.As loss ofcorrection wassmallandclinicaloutcomewassatisfactory,theauthors decidednottoperformasecondsurgicalapproach.Afterthis case,thegroup’sconductwasmodifiedandthedefinitionof distalfixationlevelswasmadeincludingthefirstlevelin lor-dosis,asrecommendedinthetreatmentofScheuermann’s kyphosis.20Inthesecondcase,therewasanL4fracturewith significantimpactonsagittalbalanceandfunctionaloutcome, butpatientwasnotreoperatedduetoclinical contraindica-tion(case11,Fig.5).Withtheexceptionofthesetwocasesof fracture,nosignificantlossofcorrectionwasobservedduring follow-up. Thismaintenanceofthe correctionovertimein uncomplicatedcaseswasobservedinmostseries.8,10,11,17,21 Astherearenoabsolutevaluesfordefiningnormal kypho-sis,theimportantparametersintheevaluationofcorrections arereducedangularkyphosisandtherestorationofsagittal balance.22Inthisseries,onlytwocasesofjunctionalkyphosis, whichhadpreviousfixationsofT10tothesacrum,had sig-nificantsagittaldecompensation.Thisisduetotwofactors: first, the mostpowerful spinopelvic sagittal compensation
Fig.3–Kyphoscoliosisduetodysplasticneurofibromatosis,with90-degreerotationofT11onT12,withspinal
compression.Patientpresentedonlylowerlimbhyperreflexia,butwasbedriddenduetopain.(A)Panoramicradiograph.
(B)Magneticresonanceimagingandradiograph,focusedshowingtheangulardeformitywith90◦ofT10–T12kyphosisand
spinalcompression.(C)Magneticresonanceimagingshowingtheextentofthemeningocelesaroundtheangulardeformity
thatledtothetransduralapproach.(D)Postoperativeradiographshowinggoodcorrectionofthedeformity.(E)Magnetic
resonanceimagingsevenmonthsaftertheinitialsurgeryshowinganarachnoidcystattheupperendofthe
instrumentation,twolevelsabovetheVCR,withimportantcompressionanddisplacementofthespinalcord.Thepatient
Fig.4–AngularkyphosisduetopathologicalfractureofT3aftermultiplemyelomatreatment.Parapareticpatientwith
strengthgradeIII.(A)Initialappearanceonmagneticresonanceimagingwith70◦ofT2–T4kyphosisandspinalcord
compression.(B)Postoperativetomographyshowinggoodcorrectionofthedeformity.(C)Radiographandtomographymade
afterdischargeduetosuddenincreaseincervicalpain.Theexamsshowpullingofthescrewsinthelateralcervical
masses,withlittlelossofcorrection.(D)Finalaspectafteranewapproach,inwhichthedorsalscrewsweremaintainedand
thecervicalimplantsreplaced,withextensionofthefixationuptoC2.TheorthostaticradiographshowstheC7plumbline
exactlyontheposterioraspectofthesacralplateau(case8).
mechanism is the adjustment oflumbar lordosis,23,24 and injuries that do not compromise the lumbar mobility are moreeasilybalanced;second,asamatteroftrigonometry,the higherthelevelofangularkyphosis,theloweritsimpacton
theoverallsagittalbalance,becauseitisfurtherawayfromthe base.25Inbothcases,animprovementonthesagittalvertical axis(SVA)withoutcompletenormalizationwasobserved.In casesoflumbarosteotomiesforsagittalimbalancecorrection,
Fig.5–L3–S1arthrodesisforovertenyears,whichevolvedwithL2–L3stenosisandextensionofthefixationuptoT10for
threeyears,developingprogressivejunctionalkyphosis.(A)Radiographshowingtheconsolidationoftheoldarthrodesis.
(B)ExtensionofthefixationuptoT10,withdevelopmentofjunctionalkyphosis.(C)Postoperativeradiographshowing
fixationextensionuptoT2andT9PSO,withgoodkyphosiscorrection.Asthelumbarsegmentwasfirmlyconsolidatedand
therewere12anchoragepointsdistaltotheosteotomy,itwasdecidedtofixateonlyuptoL4.(D)Radiograph60daysafter
surgeryshowinglossoflumbarlordosisandsagittalimbalance.Thepatientprojectedhertrunkwhenrisingfromalow
chairandfeltacrackinherlowerback.(E)DetailoftheradiographshowingwedgingofL4andlumbarrectification.Asthe
patienthadpulmonarythromboembolismpostoperativelyandwasanticoagulated,inadditiontootherclinicalproblems,it
196
rev bras ortop.2017;52(2):189–196Roseetal.26concludedthatthecombinationofPI+CD-LL≤45◦
hasapredictivevalueof91%formaintainingsagittalbalance uptotwoyearsaftersurgery.Inthedorsalspine,this princi-pledoesnotappeartobevalid,sincethelossofbalancethat occursovertimeismainlyduetotheprogressionofdorsal kyphosis;itismorenoticeableincasesinwhichthesuperior instrumentedlevelisbelowT5.26Inthepresentseries,only 50%ofpatientsmetthiscriterionandyettherewasnolossof correction.
Final
considerations
Although these procedures are complex, aggressive, and subject to complications, osteotomies with three-column resectionhaveproved tobequite effectiveand sufficiently safeforthecorrectionofrigidsagittaldeformities.Duetothe severityofthistypeofdeformity,theauthorsbelievethatthe useofosteotomiesinthetreatmentofthisconditionishighly justified.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GokceA,OzturkmenY,MutluS,Caniklio ˘gluM.Spinal osteotomy:correctingsagittalbalanceintuberculous spondylitis.JSpinalDisordTech.2008;21(7):484–8.
2. BridwellKH.Decisionmakingregardingsmith-petersenvs. pediclesubtractionosteotomyvs.vertebralcolumnresection forspinaldeformity.Spine(PhilaPa1976).2006;31(19):S171–8.
3. CostaRJF,CarelliLE,BarcellosALL,AraújoJuniorAEP, SchetinoLCV.Correc¸ãodasdeformidadessagitaisfixaspela técnicadeosteotomiadesubtrac¸ãopedicular(PSO). Coluna/Columna.2011;10(2):139–43.
4. LiF,SagiHC,LiuB,YuanHA.Comparativeevaluationof single-levelclosing-wedgevertebralosteotomiesforthe correctionoffixedkyphoticdeformityofthelumbarspine.A cadavericstudy.Spine(PhilaPa1976).2001;26(21):2385–91.
5. ShimodeM,KojimaT,SowaK.Spinalwedgeosteotomybya singleposteriorapproachforcorrectionofsevereandrigid kyphosisorkyphoscoliosis.Spine(PhilaPa1976).
2002;27(20):2260–7.
6. ChangKW,ChengCW,ChenHC,ChangKI,ChenTC. Closing-openingwedgeosteotomyforthetreatmentof sagittalimbalance.Spine(PhilaPa1976).2008;33(13):1470–7.
7. O’ShaughnessyBA,KukloTR,HsiehPC,YangBP,KoskiTR, OndraSL.Thoracicpediclesubtractionosteotomyforfixed sagittalspinaldeformity.Spine(PhilaPa1976).
2009;34(26):2893–9.
8. LehmerSM,KepplerL,BiscupRS,EnkerP,MillerSD,Steffee AD.Posteriortransvertebralosteotomyforadult
thoracolumbarkyphosis.Spine(PhilaPa1976). 1994;19(18):2060–7.
9. RajasekaranS,VijayK,ShettyAP.Single-stage
closing-openingwedgeosteotomyofspinetocorrectsevere post-tubercularkyphoticdeformitiesofthespine:a3-year follow-upof17patients.EurSpineJ.2010;19(4):583–92.
10.KawaharaN,TomitaK,BabaH,KobayashiT,FujitaT, MurakamiH.Closing-openingwedgeosteotomytocorrect angularkyphoticdeformitybyasingleposteriorapproach. Spine(PhilaPa1976).2001;26(4):391–402.
11.TomitaK,KawaharaN,BabaH,TsuchiyaH,FujitaT, ToribatakeY.Totalemblocspondylectomy.Anewsurgical techniqueforprimarymalignantvertebraltumors.Spine (PhilaPa1976).1997;22(3):324–33.
12.GertzbeinSD,HarrisMB.Wedgeosteotomyforthecorrection ofpost-traumatickyphosis.Anewtechniqueandareportof threecases.Spine(PhilaPa1976).1992;17(3):374–9.
13.BuchowskiJM,BridwellKH,LenkeLG,KuhnsCA,LehmanRA Jr,KimYJ,etal.Neurologiccomplicationsoflumbarpedicle subtractionosteotomy:a10-yearassessment.Spine(PhilaPa 1976).2007;32(20):2245–52.
14.ChunguangZ,LiminL,RigaoC,YuemingS,HaoL,Qingquan K,etal.Surgicaltreatmentofkyphosisinchildreninhealed stagesofspinaltuberculosis.JPediatrOrthop.
2010;30(3):271–6.
15.ChehG,LenkeLG,PadbergAM,KimYJ,DaubsMD,KuhnsC, etal.Lossofspinalcordmonitoringsignalsinchildrenduring thoracickyphosiscorrectionwithspinalosteotomy:whydoes itoccurandwhatshouldyoudo?Spine(PhilaPa1976). 2008;33(10):1093–9.
16.BakaloudisG,LolliF,DiSilvestreM,GreggiT,AstolfiS, MartikosK,etal.Thoracicpediclesubtractionosteotomyin thetreatmentofseverepediatricdeformities.EurSpineJ. 2011;20Suppl.1:S95–104.
17.LenkeLG,SidesBA,KoesterLA,HensleyM,BlankeKM. Vertebralcolumnresectionforthetreatmentofseverespinal deformity.ClinOrthopRelatRes.2010;468(3):687–99.
18.SmithJA.Adultdeformity–managementofsagittalplane deformityinrevisionadultspinesurgery.ContempSpine Surg.2002;3(2):9–18.
19.SukSI,KimJH,LeeSM,ChungER,LeeJH.Anterior-posterior surgeryversusposteriorclosingwedgeosteotomyin posttraumatickyphosiswithneurologiccompromised osteoporoticfracture.Spine(PhilaPa1976).
2003;28(18):2170–5.
20.HerreroCFPS,PortoMA,BarbosaMHN,DefinoHLA.
Osteotomiassegmentaresmúltiplasparaacorrec¸ãodacifose. RevBrasOrtop.2009;44(6):513–8.
21.SukSI,KimJH,KimWJ,LeeSM,ChungER,NahKH.Posterior vertebralcolumnresectionforseverespinaldeformities. Spine(PhilaPa1976).2002;27(21):2374–82.
22.WinterRB,LonsteinJE,DenisF.Sagittalspinalalignment:the truemeasurement,norms,anddescriptionofcorrectionfor thoracickyphosis.JSpinalDisordTech.2009;22(5):311–4.
23.LafageV,SchwabF,SkalliW,HawkinsonN,GageyPM,Ondra S,etal.Standingbalanceandsagittalplanespinaldeformity: analysisofspinopelvicandgravitylineparameters.Spine (PhilaPa1976).2008;33(14):1572–8.
24.SchwabF,LafageV,BoyceR,SkalliW,FarcyJP.Gravityline analysisinadultvolunteers:age-relatedcorrelationwith spinalparameters,pelvicparameters,andfootposition. Spine(PhilaPa1976).2006;31(25):E959–67.
25.OndraSL,MarzoukS,KoskiT,SilvaF,SalehiS.Mathematical calculationofpediclesubtractionosteotomysizetoallow precisioncorrectionoffixedsagittaldeformity.Spine(Phila Pa1976).2006;31(25):E973–9.