Disciplina de Neurocirurgia, Faculdade de Ciências M édicas da Universidade de Campinas (UNICAM P), Campinas SP, Brasil: 1M édico Resident e, 2Prof essor Associado,3M édico Cont rat ado,4Prof essor Dout or.
Received 31 M arch 2004, received in f inal f orm 4 June 2004. Accept ed 21 July 2004.
Dr. João Paulo M at t os - Rua Hermant ino Coelho 758/31 - 13087-500 Campinas SP - Brasil. E-mail: jpvmat t [email protected]
INTRADURAL JUGULAR FORAM EN TUM ORS
João Paulo M at t os
1, Ricardo Ramina
2, Wilson Borges
1, Enrico Ghizoni
1,
Yvens B. Fernandes
3, Jorge R. Paschoal
4, Donizet i C. Honorat o
4, Guilherme Borges
4ABSTRACT - Eleven pat ient s w it h jugular f oramen lesions w it h or w it hout ext radural ext ension w ere oper-at ed oper-at Universit y Hospit al of Campinas (UNICAM P), in Campinas, Brazil, bet w een 1998 and 2001. Neck dis-sect ion, mast oidect omy w it hout t ransposit ion of t he f acial nerve and myof ascial f lap reconst ruct ion of t he cranial base w it h an especially developed t echnique w ere carried out in 7 pat ient s. Four pat ient s w ere oper-at ed using ret rosigmoid craniect omy. Tot al excision w as accomplished in 9 cases. All poper-at ient s did not show evidence of disease progression at least af t er 2 years f ollow -up. There w as no mort alit y. New low er cra-nial nerve deficits occurred in 5 patients. Nine maintain or improved their preoperative status based on Karnofsky and Glasgow Out come Scale. A complex anat omy of t his region demand w ide exposures f or t reat t hose t umors. For t his reason, an adequat e approach f or curat ive resect ion of most lesions and an eff icient skull base reconst ruct ion decreasing post operat ive morbidit y are essent ial.
KEY WORDS: jugular f oramen, post erior f ossa t umor, low er cranial nerves, skull base reconst ruct ion, glo-mus t umor.
Tum ores int radurais do f oram e jugular
RESUMO - Onze pacientes com lesões expansivas do forame jugular associadas ou não a componente extradural f oram submet idos a ressecção cirúrgica no Hospit al das Clínicas da Universidade Est adual de Campinas (UNI-CAM P) ent re 1998 e 2001. Foi ut ilizada cirurgia combinada com dissecção do pescoço, mast oidect omia sem t ransposição do nervo f acial e t écnica de reconst rução miof ascial da base do crânio desenvolvida por um dos aut ores. Quat ro pacient es f oram operados via craniect omia ret rosigmoidea. Ressecção t ot al f oi f eit a em 9 pacient es, subt ot al em um e parcial em out ro. Nenhum dos 11 pacient es t eve progressão da doença em 2 anos de acompanhament o. Não houve mort alidade. Cinco pacient es t iveram déf icit s adicionais de nervos cranianos baixos. Nove pacient es mant iveram ou melhoraram suas pont uações de acordo com a escala de Karnofsky. Para adequada abordagem do paciente com tumor de forame jugular, são necessários bom conheciment o anat ômico da região, exposição cirúrgica ampla, e t écnica de reconst rução ef icient e para obt er cura com baixas t axas de complicações pós-operat órias.
PALAVRAS-CHAVE: f orame jugular, t umor de f ossa post erior, nervos cranianos baixos, reconst rução de base de crânio, t umor de glomus jugular.
Jugular f oramen (JF) lesions are rare, being pa-ragagliomas and schw annomas t he most common t umors 1, 2. Complet e resect ion of t hese benign
le-sions is t he t reat ment of choice. The surgical man-agement of JF lesions remains difficult because t heir deep locat ion, locally aggressive behavior, involve-ment of vessels and nerves, inf ilt rat ion of skull ba-se bone and st ruct ures of t he high cervical region and t he complex anat omy of t he region. In t he last decades, development of new skull base approaches allow ed t ot al resect ion of large number of skull ba-se t umors. How ever, t he more aggressive t he surgical approach becomes, more complicat ions relat -ed t o it may occur. Reconst ruct ion of t he skull base
after large bone resection is very important to avoid complicat ions. For t his reason, t he surgical access and t he reconst ruct ion t echniques are decisive f ac-t ors concerning ac-t he ouac-t come.
We report 11 pat ient s w it h JF t umors operat ed at t he Skull Base Cent er of t he UNICAM P, bet w een 1998 and 2001. The clinical, radiological, surgical t echnique and t he result s are discussed.
M ETHOD
Pat ient populat ion – Eleven pat ient s w it h int
years (range 13 t o 63 years). The init ial sympt oms w ere hearing loss (6 cases), hoarseness (2 cases), headache (2 cases) and t innit us (1 pat ient ). The mean t ime bet w een init ial sympt oms and t he search f or t reat ment w as 3.3 years. At t he t ime of diagnosis all pat ient s had some de-gree of hearing loss, f ive show ed f acial nerve palsy and t hree had low er cranial nerves dysf unct ion (Table 1). The post operat ive f ollow -up period ranged f rom 2 t o 4.2 years. There w ere 6 paragangliomas, 2 schw annomas, 1 meningioma, 1 choroid plexus papiloma and 1 endolym-phat ic sac t umor.
Radiological evaluat ion – All pat ient s w ere evaluat ed
pre and post operat ively w it h comput erized t omography (CT) and magnet ic resonance imaging (M RI). The lesions w ere classif ied using “ Curit iba 1988” classif icat ion (Table 2) according t o involvement of ear, neck and int racra-nial compart ment in t ypes E, EN and ENI3. Four vessel
an-giography and preoperat ive embolizat ion w it h Ivalon part icles w ere carried out (6 cases) 48 t o 72 hours bef ore surgery when the radiological findings revealed a high vas-cular t umor as usually f ound in paragangliomas.
Surgical approaches– A multidisciplinary team
compo-sed by neurosurgeons and ot ologist s perf ormed t he sur-gical procedure. The decision concerning t he sursur-gical ap-proach w as based on radiological aspect s. Int racranial t umors t hat show ed no evidence of ear, t emporal bone or neck involvement w ere approached by ret rosigmoid
craniect omy (4 cases). In t he remained 7 cases, ret rosig-moid craniect omy associat ed t o neck dissect ion and mas-t oidecmas-t omy w as perf ormed mas-t o remove bomas-t h inmas-t radural and ext radural t umor in one surgical procedure.
The pat ient is placed supine w it h underneat h shoul-der roll and t he head t urned approximat ely 45 degrees t o t he opposit e side and f ixed in a M ayf ieldt hree pin head - holder.
A C shaped incision f rom t he t emporal f ossa, passing behind t he ear, t o t he ant erior border of st ernomast oid muscle in the high cervical region is performed for the com-bined approach (Fig 1). A linear ret ro auricular incision 4 cm behind t he ext ernal audit ory canal, 4 cm above t he helix and 4 cm under t he lobule is used f or ret romas-t oid craniecromas-t omy. The skin f lap is roromas-t aromas-t ed anromas-t eriorly ex-posing t he post erior t emporal, pariet occipit al and high cervical areas.
Miofascial flap for skull base reconstruction – The
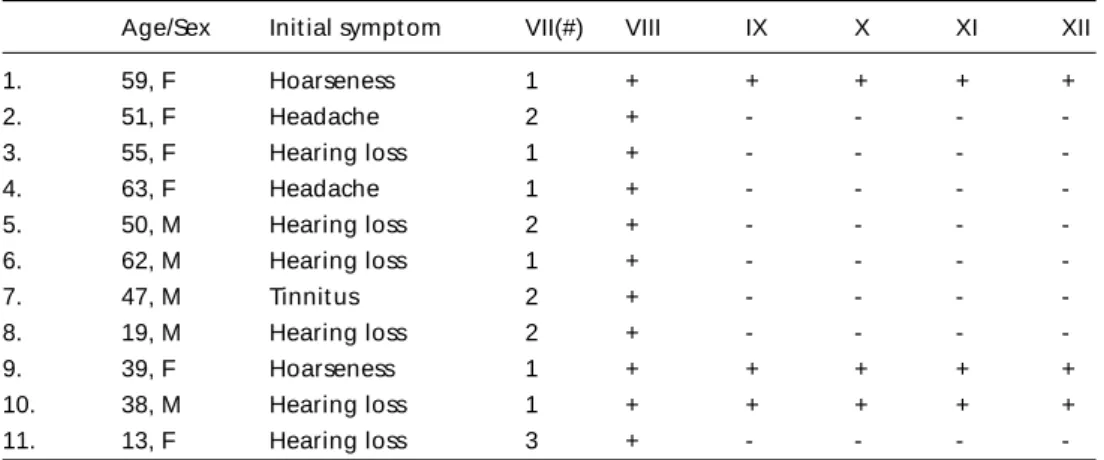
tem-poral f ascia is incised in t he middle port ion of t he t empo-Table 1. Init ial present at ion of 11 pat ient s w it h jugular f oramen t umors.
Age/Sex Init ial sympt om VII(#) VIII IX X XI XII
1. 59, F Hoarseness 1 + + + + +
2. 51, F Headache 2 + - - -
-3. 55, F Hearing loss 1 + - - -
-4. 63, F Headache 1 + - - -
-5. 50, M Hearing loss 2 + - - -
-6. 62, M Hearing loss 1 + - - -
-7. 47, M Tinnit us 2 + - - -
-8. 19, M Hearing loss 2 + - - -
-9. 39, F Hoarseness 1 + + + + +
10. 38, M Hearing loss 1 + + + + +
11. 13, F Hearing loss 3 + - - -
-# House-Brackmann grade f or f acial f unct ion; VII, VIII, IX, X, XI and XII = cranial nerves; (+) presence of nerve def icit ; (-) absence of nerve def icit
Table 2. Curit iba 1988 classif icat ion.
E Tumor locat ed in t he ear (E)
EN Tumor locat ed in t he ear (E) and neck (N) ENI Tumor in t he ear (E), neck (N) and int radural
(I) compart ment
M IXED Combinat ion among t he ant erior t ypes N Tumor rest rict ed t o t he neck (N)
I Tumor rest rict ed t o int radural (I) compart ment
ral region and dissect ed t o t he t emporal line. The cervi-cal f ascia is cut post erior t o t he ext ernal audit ory canal, mast oid t ip and over t he st ernocleidomast oid muscle (SCM ). The insert ion of SCM is removed f rom t he mas-t oid and mas-t he vascularized miof ascial f lap is mas-t urned posmas-t erior and inf eeriorly. In pat ient s w it h preoperat ive deaf -ness, t he ext ernal audit ory canal is t ransect ed and closed w it h separat e sut ures covered by a post erior auricular muscle f lap.
Neck dissect ion – Neck dissect ion w it h ident if icat ion
of t he Xt h, XIt h, and XIIt hcranial nerves, common carot id,
ext ernal carot id and int ernal carot id art eries, and t he jugular vein is perf ormed. The vert ebral art ery is alw ays ident if ied at t he craniocervical junct ion. The f acial nerve is ident if ied superiorly t o t he digast ric muscle using t he point er and t he mast oid process as paramet ers.
M ast oidect omy – A radical mast oidect omy is perf
or-med. Removal of t he semicircular canal is carried out if
t he lesion inf ilt rat es t his st ruct ure. The middle f ossa and presigmoid dura mat er are exposed. The f acial nerve re-mains in it s bone canal if t he lesion does not inf ilt rat e it . The ret rof acial mast oid cells are removed.
Ret rosigmoid craniect omy – A key-hole on ast erion
f ollow ed by a 3 cm post erior f ossa craniect omy is perf or-med exposing the transverse sinus superiorly and unroof-ing completely the sigmoid sinus. The JF is widely opened.
Ligat ure of sigmoid sinus and jugular vein – A small
dura incision is made on each side of sigmoid sinus (SS) inf erior t o t he superior pet rosal sinus. The SS is ligat ed w it h t w o sut ures. The int ernal jugular vein (IJV) is liga-t ed and culiga-t in liga-t he high cervical region.
Tumor removal – Af t er opening t he post erior w all
of SS, t he ext racranial port ion of t umor is removed f rom t he JF w it h t he IJV. The dura mat er is incised in t he me-dial w all of t he SS and t he int racranial port ion of JF and it s cont ent s are exposed. The lesion is resect ed using mi-crosurgical techniques. Infiltrated dura mater is complete-ly resect ed. Dura mat er inf ilt rat ion is more f requent complete-ly f ound in meningiomas and paragangliomas.
Skull base reconstruction (myofascial flap) – If primary
w at ert ight dural closure is not possible, a t emporal f as-cia f lap is used t o cover t he def ect . Fibrin glue is alw ays used. A second skull base reconst ruct ion layer is f ormed by t he inf erior rot at ion of post erior port ion of t empo-ral muscle (Fig 2).
The myof ascial f lap is rot at ed ant eriorly, t he t empo-ral fascia is approximated and sutured and the cervical f cia is sut ured in t he parot id f ascia and ant erior neck f as-cia. This t hree layer closure covers t he ent ire bone def ect due t o mast oidect omy and post erior f ossa craniect omy (Fig 3). The SCM muscle shape is maint ained. The scalp f lap is closed in a single layer w it h separat ed non absor-bable sut ures. No drain is used and prophylact ic. Lumbar drainage w as not necessary w it h t his t echnique.
RESULTS
Tot al t umor resect ion could be achieved in 9 pa-t ienpa-t s conf irmed by pospa-t operapa-t ive radiological eva-luat ion t hat f ailed t o show residual expansive le-sions w it h cont rast enhancement . Five pat ient s pre-sented with postoperative IXthand Xthnerve deficits,
2 show ed XIt h and XIIt h def icit s and 2 w orsening
their facial weakness. The new cranial nerve deficits w ere not associat ed w it h t umor size or hist opat ho-logic findings but with tumor infiltration of the ner-ves and dura. Incomplet e resect ion w as perf ormed in 2 cases w it h giant t umors present ing w it h involvement of t he ear, neck and int radural compart -ment s. Eight pat ient s w ho achieved complet e t u-mor resect ion maint ained or improved t heir
pre-Fig 2. Post erior t hird of t he lef t t emporalis muscle (TM ) dissec-t ed f rom idissec-t s andissec-t erior pordissec-t ion f or inf erior and posdissec-t erior rodissec-t adissec-t ion (black arrow ) covering t he mast oid bone def ect .
operat ive st at us conf irmed by Karnof sky Perf or-mance Scale of 90 or 100 and Glasgow Out come Scale (GOS) 4 or 5. One patient in the group of com-plet e resect ion w orse his clinical st at us f rom Kar-nof sky 100 t o 80. The remaining 2 pat ient s had an incomplet e resect ion. One had part ial (< 90% ) and the other subtotal (> 90%) tumoral removal accord-ingly to contrast enhanced residual lesion in the pos-t operapos-t ive M RI. One papos-t ienpos-t remains w ipos-t h his pre-operat ive Karnof sky st at us and t he ot her one decreased it f rom 80 t o 70. Bot h pat ient s show ed no evidence of progressive disease af t er f ollow up examinat ions and radiological evaluat ion 28 mon-t hs af mon-t er mon-t he surgical procedure. One pamon-t ienmon-t devel-oped cerebrospinal f luid (CSF) leak and meningi-t is meningi-t reameningi-t ed w imeningi-t h anmeningi-t ibiomeningi-t ics. There w as no mormeningi-t al-it y and no local inf ect ion (Table 3).
DISCUSSION
JF lesions are uncommon4,5. Paraganglioma w as
t he most common t umor in our series f ollow ed by schw annoma. This f inding is in accordance w it h t he lit erat ure1,2,5. Paragangliomas are rare benign
t umors t hat arise f rom paraganglionic cells along t he body. In t he skull base, t he most f requent sit e f or paragangliomas is in t he jugular and t ympan-ic paraganglia also called glomus jugulare or glo-mus tympanicum tumors, respectively5, 6. Schw
anno-mas are t he second most common t umor at t his lo-cat ion, arising f rom IXt h, Xt hor XIt h cranial nerves.
M eningiomas, met ast ases, giant cell t umors, chon-drosarcomas, plasmocyt omas, epidermoid cyst s, amyloidomas, endolymphat ic sac t umors are des-cribed in t his locat ion as primary or ext ended le-sions2,7-12.
The growth pattern of tumor seems to be
decisi-ve for clinical presentation of this group of patholo-gy. Predominant ly int racranial expansion is relat ed t o sympt oms of post erior f ossa compression and deaf ness. Tumors w it h primary bone or ext racrani-al involvement usuracrani-ally present w it h low er craniracrani-al nerve dysf unct ions13-15. Hearing loss is t he most
f requent sympt om of JF t umors13,14,16-20. In our
se-ries, all tumors had intracranial component and audi-t ory dysf uncaudi-t ion w as presenaudi-t in all cases. The jugu-lar f oramen syndrome is not alw ays present16; how
-ever, normal cranial nerve f unct ion bef ore surgery does not exclude cranial nerve t umor inf ilt rat ion21.
Glomus jugulare t umors are more common in f emale pat ient s5,14,19,21,22. M ult iple paragangliomas
are found in approximately 10% of cases5,16,21,23. The
presence of bilat eral glomus jugulare or cont ralat -eral glomus vagale t umor may result in post opera-tive bilateral lower cranial nerve palsies16. The mean
t ime bet w een t he init ial sympt oms and t he diag-nosis demonst rat e t he slow grow t h pat t ern of pa-ragangliomas5,22and schw annomas13,14, as f ound in
our series. The mean age at present at ion is around t he f if t h decade5,19,21.
Radiological investigation – Computerized
tomo-graphy is very usef ul t o show bone st ruct ures, t he jugular f oramen cont ours and it s variat ions. Bone erosion is usually f ound in paragangliomas in con-t rascon-t con-t o schw annomas con-t hacon-t f requencon-t ly presencon-t w icon-t h JF enlargement with smooth indistinct sclerotic mar-gins13,24. Angiography is usef ul t o diff erent iat e bet
-ween schwannoma and paraganglioma. Schwanno-mas are usually less vascularized t han paraganglio-mas13. Ascending pharyngeal art eries and
menin-geal branches of occipit al art ery supply most of t
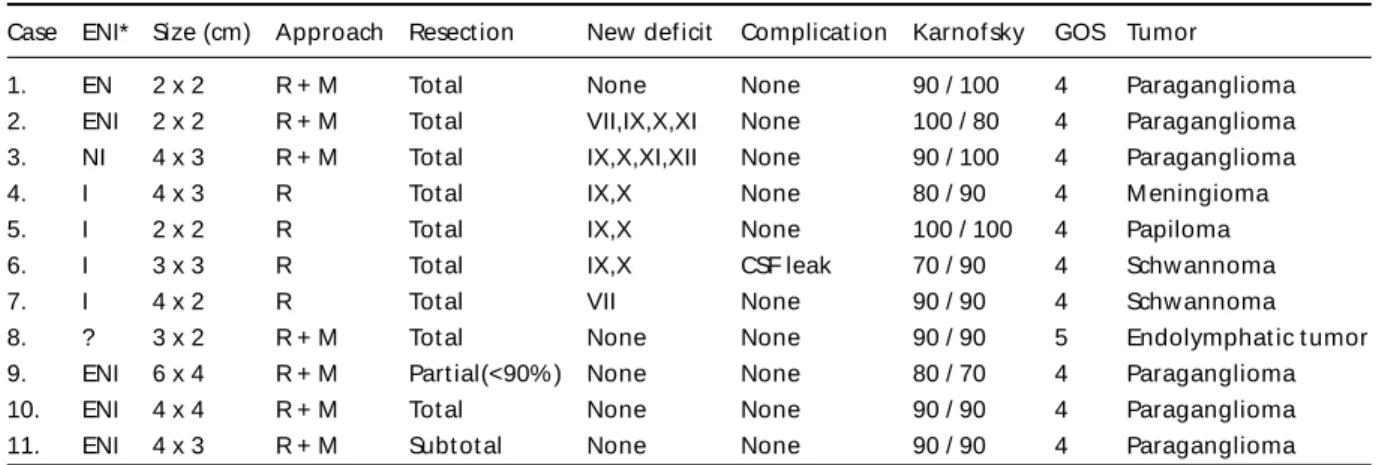
u-Table 3. Tumoral aspect s and result s.
Case ENI* Size (cm) Approach Resect ion New def icit Complicat ion Karnof sky GOS Tumor
1. EN 2 x 2 R + M Tot al None None 90 / 100 4 Paraganglioma
2. ENI 2 x 2 R + M Tot al VII,IX,X,XI None 100 / 80 4 Paraganglioma 3. NI 4 x 3 R + M Tot al IX,X,XI,XII None 90 / 100 4 Paraganglioma
4. I 4 x 3 R Tot al IX,X None 80 / 90 4 M eningioma
5. I 2 x 2 R Tot al IX,X None 100 / 100 4 Papiloma
6. I 3 x 3 R Tot al IX,X CSF leak 70 / 90 4 Schw annoma
7. I 4 x 2 R Tot al VII None 90 / 90 4 Schw annoma
8. ? 3 x 2 R + M Tot al None None 90 / 90 5 Endolymphat ic t umor
9. ENI 6 x 4 R + M Part ial(<90% ) None None 80 / 70 4 Paraganglioma
10. ENI 4 x 4 R + M Tot al None None 90 / 90 4 Paraganglioma
11. ENI 4 x 3 R + M Subt ot al None None 90 / 90 4 Paraganglioma
mors locat ed at t his region. In our series, all para-gangliomas w ere submit t ed t o embolizat ion. The ascending pharyngeal art ery supply w as f ound in every case (6 cases). It is also import ant t o deline-at e t he pdeline-at ency of jugular bulb bef ore surgery as progressive obst ruct ion is of t en seen in t umors at t his locat ion and permit s t he development of col-lat eral circucol-lat ion; how ever, dominant or non com-municat ing sigmoid sinus can lead t o int racranial hypert ension if ligat ion is achieved during surgi-cal procedure25. Af t er t he int roduct ion of t he M RI,
t he anat omic det ails, t umor margins, relat ionship of major vessels, vascular supply and even t he pa-t ency of jugular bulb can be observed14. M
enin-giomas, choroid plexus papilomas and paraganglio-mas show s high cont rast enhancement .
Jugular f oramen anat omy – The jugular f
ora-men is an apert ure in t he post erior half of t he skull base behind t he carot id canal. It s ant erolat -eral border is f ormed by pet rous t emporal bone an d t h e p o st er o m ed i al w al l b y t h e o cci p i t al bone14,24,26. The classic division of JF in t hree part s
is described. The ant erior, cont aining t he inf erior pet rosal sinus as it ent ers t he jugular vein; t he middle part , t he IXt h, Xt hand XIt hcranial nerves and
t he post erior, t he jugular bulb and meningeal branches of occipit al and ascending pharyngeal art eries24. Hovelaque divided t he JF in t w o
com-part ment s27. The larger post erolat eral also called
pars venosa cont aining jugular bulb, Xt hand XIt h
cranial nerves and a smaller compartment (pars ner-vosa) cont aining IXt hcranial nerve. The perf orat ion
can be separat ed by f ibrous sept um in 74% t o 80%26,28or by bone sept um in t he remained
cas-es. Ayeni et al. described t hat bot h t he division in pars venosa and nervosa or t hree compart ment s should not be used as t he IXt h, Xt hand XIt hcranial
nerves are ent irely ant eromedial t o jugular bulb28,29
in spit e of t he presence of anat omic separat ion of JF by f ibrous or bone bridge. The right JF is usual-ly larger t han t he lef t in 68% t o 70%26,28and equal
in 20%28. The cranial nerves (CN) lay in a
connec-t ive connec-t issue sheaconnec-t h w iconnec-t h IXt h CN being t he most ant
e-rior, complet ely separat ed f rom t he ot hers and t he XIt hCN t he most post erior20,28. The IXt hnerve
is usually individual inside t he JF, t he XIt hCN is f
re-quent ly divided in t w o part s (spinal and cranial) and t he Xt hnerve w it h mult iple f ascicles20,26,28. The
superior jugular bulb is post erolat eral t o low er cranial nerves and show s mult iple conf igurat ions concerning the inferior petrosal sinus (IPS) entrance.
The IPS can drain int o t he jugular bulb, int ernal jugular vein or bot h by single or mult iple channels an t er i o r t o IXt h n er ve an d p o st er i o r t o XIt h
nerve20,26,28.
Treat ment modalit ies – Complet e surgical
remo-val is t he t reat ment of choice f or jugular f oramen paragangliomas5,29,30. Comparative studies between
radiot herapy and surgery lack of consist ency19.
The f ollow up periods are short considering t he slow grow t h of t his t umor and it s nat ural hist ory. Some report s describe long t ime survival and even involut ion of t he t umor w it hout int ervent ional procedures19,22,30. Radiot herapy is not curat ive and
has no act ivit y in t he t umoral cells but in t he vascu-lar supply limit ing t he t umor vascuvascu-larit y leading t o f ibrosis5. This kind of t reat ment may be indicat ed
in pat ient s w it h poor surgical condit ion and residu-al or recurrent tumors5,21,22,30. The age may be a
limi-t ing f aclimi-t or bulimi-t limi-t he limi-t herapeulimi-t ic decision muslimi-t be individually considered.
Tumors at JF may arise from extradural compart-ment , int radural or bot h. Int radural involvecompart-ment means pot ent ial complicat ions such as CSF f ist ula, meningit is, brain st ruct ures adherence and t heir consequences. In our series, all pat ient s had in-t radural in-t umors. Dif f erenin-t surgical in-t echniques are used f or t hose t umors. In neurosurgical series, es-sent ially JF int radural t umors as meningiomas, schwannomas, epidermoid cysts and some metasta-t ic lesions are approached by remetasta-t rosigmoid roumetasta-t e in most cases13-15. M any t echniques are described
for large lesions with transcranial component. Trans-canal and post eroauricular approaches are not discussed because t heir use is rest rict ed t o small t umors at promont ory, middle ear and hypo t ym-panum. We use an inf ralabyrint hine or t rans-labyrint hine approach depending on t he audit o-ry f unct ion. Dif f erent skin incisions are described f or large t umors. Glasscock et al.22use modif ied
in-f rat emporal in-f ossa approach w it h C shaped incision above and just behind t he auricle but w it hout ex-t ension ex-t o ex-t emporal or posex-t erior f ossa region. Sa-mii et al.14use a ret ro auricular incision ext ending
exposures. Some aut hors t ranspose t he f acial nerve during t umor removal5,16,21,22,29, especially in t hose
t umors w it h ant erior ext ension, w it h t he object ive of increase t he surgical exposure w it h less mobi-lizat ion of low er cranial nerves. This maneuver leads t o t ransit ory f acial nerve dysf unct ion in most pat ient s and def init ive def icit in some. Some aut hors do not t ranspose t he f acial nerve14,31. In our
surgical t echnique t he f acial nerve is skelet onized and lef t int act in f allopian canal except if t here is t umoral inf ilt rat ion. In our cases, t he f acial nerve f unct ion w as maint ained in nine pat ient s w it h t his t echnique. Tw o pat ient s show ed post operat ive f acial nerve impairment . The f irst one had inf ilt ra-t ive paraganglioma. The second para-t ienra-t had an int radural t umor and t he f acial palsy w as due in-t racranial dissecin-t ion of in-t he in-t umor capsule f rom in-t he VIIt hnerve. The ext racranial port ion of t umor is f irst
removed f ollow ed by dural opening and int radur-al tumorradur-al microsurgicradur-al resection. The dura is resect-ed w hen t here is any degree of inf ilt rat ion and reconst ruct ion of t he skull base in t hree layers is done as previously described in t his t ext .
Complicat ions – The low er cranial nerve def icit s
leading t o dysphagia, breat hing diff icult y, hoarse-ness and pneumonia due t o aspirat ion are pot en-t ial dangerous problems. According en-t o lien-t eraen-t ure many prophylact ic or t herapeut ic procedures are performed such as tracheostomy, gastrostomy, vocal cord manipulat ions and cricopharyngeal myo-t omy5,14,18,21,22,31. Samii et al.14advocat e t emporary
t racheost omy if t he low er cranial nerves are sac-rif iced during t he surgical procedure and sw al-low ing f unct ion is injured in t he post operat ive period. Persist ent hoarseness is t reat ed w it h Tef lon inject ion int o paralyzed vocal cord af t er 6 mont hs f rom surgical procedure according t o George5or
earlier in post operat ive period by Fent on et al.18
result ing in a bet t er voice and cough ref lex. Gas-t rosGas-t omy is employed if persisGas-t enGas-t aspiraGas-t ion oc-curs14. In our series, t emporary dysphagia and
hoar-seness w ere common. All pat ient s are maint ained w it h ent eral f eeding unt il t he sw allow ing f unct ion permit t he oral int ake. Nasogast ric t ube w as kept in place for as long as 14 days but no permanent pro-cedure as t racheost omy or gast rost omy w as neces-sary. No pat ient had aspirat ive pneumonia. No pa-t ienpa-t underw enpa-t vocal cord augmenpa-t apa-t ion.
CSF f ist ula is anot her t ype of lif e t hreat ening complicat ion. M eningit is can occur increasing t he morbidit y and mort alit y. The use of f ibrin glue
(Beriplas®) af t er t he dura closure f ollow ed by
mio-f ascial mio-f lap rot at ion has been mio-f ound very emio-f mio-f icient in avoiding t his complicat ion.
CONCLUSION
Surgical removal of JF benign lesion may be cura-t ive. Adequacura-t e exposure and skull base reconscura-t ruc-t ion are very imporruc-t anruc-t ruc-t o achieve compleruc-t e resec-t ion and resec-t o avoid posresec-t operaresec-t ive complicaresec-t ions.
An experienced mult idisciplinary t eam, an ade-quat e individually pre and post operat ive evalua-t ion of evalua-t he paevalua-t ienevalua-t s are evalua-t he requisievalua-t es evalua-t o achieve ra-dical t umor removal w it h low morbidit y rat es and good overall f unct ional out come.
The f act t hat some pat ient s had short f ollow -up period and t hat most JF t umors has slow grow t h pat t ern must be considered. How ever, t he good out come of t he pat ient s demonst rat ed by Karno-f sky scale in t he post operat ive period added t o ab-sence of residual t umor or t umoral progression in all pat ient s show s t hat t he goal of t reat ment w as accomplished.
REFERENCES
1. George B, Lot G, Tran Ba Huy P. The justacondylar approach to the jugu-lar foramen (without bone drilling). Surg Neurol 1995;44:279-284. 2. Weber AL, McKenna MJ. Radiologic evaluation of the jugular foramen:
anatomy, vascular variants, anomalies and tumors. Neuroimaging Clin N Am 1994;4:579-598.
3. Ramina R, Maniglia JJ, Paschoal JR, Pedrozo AA, Coelho M Neto, Bor-ges G. Tumores do forame jugular. In Pereira CU, Aguiar PH, Ramina R. Tópicos em neurocirurgia. Rio de Janeiro: Revinter, 2001:65-71. 4. Seyfried DM, Rock JP. The transcondylar approach to the jugular
fora-men: a comparative anatomic study. Surg Neurol 1994;42:265-271. 5. George B. Jugular foramen paragangliomas. Acta Neurochir (Wien)
1992;118:20-26.
6. Briggs RJ, Kaye AH. Paragangliomas of the skull base and neck. In Kaye AH, Black PM (eds). Operative neurosurgery. London: Churchill Li-vingstone 2000:929-934.
7. Chao CK, Sheen TS, Lien HC, Hsu MM. Metastatic carcinoma to the jugular foramen. Otolaryngol Head Neck Surg 2000;122:922-923. 8. Rosenbloom JS, Storper IS, Aviv JE, Hacein-Bey L, Bruce JN. Giant cell
tumors of the jugular foramen. Am J Otolaryngol 1999;20:176-179. 9. Roche PH, Dufour H, Figarella-Branger D, Pellet W. Endolymphatic sac
tumors: report of three cases. Neurosurgery 1998;42:927-932. 10. Harvey SA, Wiet RJ, Kazan R. Chondrosarcoma of the jugular foramen.
Am J Otol 1994;15:257-263.
11. Matsumoto T, Tani E, Maeda Y, Natsume S. Amyloidomas in the cere-bellopontine angle and jugular foramen: case report. J Neurosurg 1985;62:592-596.
12. Lee SH, Osborn MA, Buchheit WA. Glioma of the jugular foramen. J Neurosurg 1976;44:493-495.
13. Kaye AH, Hahn JF, Kinney SE, Hardy RW, Bay JW. Jugular foramen schwannomas. J Neurosurg 1984;60:1045-1053.
14. Samii M, Babu RP, Tatagiba M, Sepehrnia A. Surgical treatment of ju-gular foramen schwannomas. J Neurosurg 1995;82:924-932. 15. Carvalho GA, Tatagiba M, Samii M. Cystic schwannomas of the jugular
foramen: clinical and surgical remarks. Neurosurgery 2000;46:560-566. 16. Jackson CJ, Glasscock ME, Nissen AJ, Schwaber MK. Glomus tumor surgery: the approach, results and problems. Otolaryngol Clin N Am 1982;15:897-916.
18. Fenton JE, Brake H, Shirazi A, Mendelsohn MS, Atlas MD, Fagan PA. The management of dysphagia in jugular foramen surgery. J Laringol Otol 1996;110:144-147.
19. Anand VK, Leonetti JP, AL-Mefty O. Neurovascular considerations in surgery of glomus tumors with intracranial extensions. Laryngoscope 1993;103:722-728.
20. Sen C, Hague K, Kacchara R, Jenkins A, Das S, Catalano P. Jugular fora-men: microscopic anatomic features and implications for neural preserva-tion with reference to glomus tumors involving the temporal bone. Neurosurgery 2001;48:838-847.
21. Green JD, Brackmann DE, Nguyen CD, Arriaga MA, Telischi FF, Cruz A. Surgical management of previously untreated glomus jugulare tu-mors. Laryngoscope 1994;104:917-921.
22. Glasscock ME, Jackson CG, Dickins JR Wiet RJ, Panel discussion: glo-mus jugulare tumors of the temporal bone. The surgical management of glomus tumors. Laryngoscope 1979;89:1640-1654.
23. Spector GJ, Sobol S, Thawley SE, Maisel RH, Ogura JH. Panel discus-sion: glomus jugulare tumors of the temporal bone. Patterns of inva-sion in the temporal bone. Laryngoscope 1979;89:1628-1639.
24. Shapiro R. Compartmentation of the jugular foramen. J Neurosurg 1972;36:340-343.
25. Sekhar LN, Tzortzidis FN, Bejjani GK, Schessel DA. Saphenous vein graft bypass of the sigmoid sinus and jugular bulb during the removal of glomus jugulare tumors. J Neurosurg 1997;86:1036-1041. 26. Rothon AL, Buza R. Microsurgical anatomy of the jugular foramen. J
Neurosurg 1975;42:541-550.
27. Hovelaque A. Osteologie, Vol 2 Paris: G Doin, 1934;2:155-156. 28. Ayeni SA, Ohata K, Tanaka K, Hakuba A. The microsurgical anatomy
of the jugular foramen. J Neurosurg 1995;83:903-909.
29. Cece JA, Lawson W, Biller HF, Eden AR, Parisier SC. Complications in the management of large glomus jugulare tumors. Laryngoscope 1987;97:152-157.
30. Glasscock ME, Harris PF, Newsome G. Glomus tumors: diagnosis and treatment. Laryngoscope 1974;84:2006-2032.