www.jped.com.br
ORIGINAL
ARTICLE
The
association
between
healthy
lifestyle
behaviors
and
health-related
quality
of
life
among
adolescents
夽
José
J.
Muros
a,∗,
Federico
Salvador
Pérez
b,
Félix
Zurita
Ortega
c,
Vanesa
M.
Gámez
Sánchez
b,
Emily
Knox
daUniversidaddeGranada(UGR),FacultaddeFarmacia,DepartamentodeNutriciónyBromatología,Granada,Spain bUniversidaddeGranada(UGR),FacultaddeEducación,DepartamentodeDidácticayOrganizaciónEscolar,Granada,Spain cUniversidaddeGranada(UGR),FacultaddeCienciasdelaEducación,DepartamentodeDidácticadelaExpresiónMusical,
CorporalyPlástica,Granada,Spain
dSchoolofHealthSciences.UniversityofNottingham,Nottingham,UnitedKingdom
Received18July2016;accepted13October2016 Availableonline25January2017
KEYWORDS
Qualityoflife; Physicalactivity; Mediterraneandiet; Bodymassindex
Abstract
Objective: Theaimofthisresearchwastoexaminetheassociationbetweenbodymassindex,
physicalactivity,adherencetotheMediterraneandiet,andhealth-relatedqualityoflifeina
sampleofSpanishadolescents.
Method: Thestudyinvolved456adolescentsagedbetween11and14years.Theycompleted
questionnairesontheMediterraneandiet(KIDMED),physicalactivity(PhysicalActivity
Ques-tionnaireforOlderChildren[PAQ-C]),andqualityoflife(KIDSCREEN-27).Bodymassindexwas
calculated.Hierarchical linearregressionanalyses were usedtodetermine whether
health-related quality of life could be predicted by the measured variables. The variables were
analyzedinastepwisemanner,withMediterraneandietenteredinthefirststep,bodymass
indexinthesecond,andphysicalactivityinthethird.
Results: Mediterraneandietaccountedfor4.6%ofthevarianceinadolescent’shealth-related
qualityoflife,withhigheradherencetotheMediterraneandietpredictinghigherhealth-related
qualityoflife-scores.Bodymassindexaccountedforafurther4.1%ofthevariance,withahigher
bodymassindexpredictinglowerhealth-relatedqualityoflifescores.Finally,physicalactivity
explainedanadditional11.3% ofthevariance,withahigherlevelofphysicalactivitybeing
associatedwithhigherhealth-relatedqualityoflifescores.Together,thesevariablesexplained
20%ofthevarianceintheadolescents’health-relatedqualityoflife.
夽
Pleasecitethisarticleas:MurosJJ,PérezFS,OrtegaFZ,SánchezVM,KnoxE.Theassociationbetweenhealthylifestylebehaviorsand health-relatedqualityoflifeamongadolescents.JPediatr(RioJ).2017;93:406---12.
∗Correspondingauthor.
E-mail:[email protected](J.J.Muros).
http://dx.doi.org/10.1016/j.jped.2016.10.005
Healthpromotioninapediatricpopulation 407
Conclusions: Physicalactivity,bodymassindex,andadherencetotheMediterraneandietare
importantcomponentstoconsiderwhentargetingimprovementsinthehealth-relatedquality
oflife ofadolescents, withphysical activityrepresentingthe componentwith thegreatest
influence.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
PALAVRAS-CHAVE
Qualidadedevida; Atividadefísica; Dietamediterrânea; Índicedemassa corporal
Associac¸ãoentrecomportamentosdeestilodevidasaudáveleaqualidadedevida relacionadaàsaúdeentreadolescentes
Resumo
Objetivo: Oobjetivodestapesquisafoiexaminaraassociac¸ãoentreoíndicedemassacorporal,
aatividadefísica,aadesãoàdietamediterrâneaeaqualidadedevidarelacionadaàsaúdeem
umamostradeadolescentesespanhóis.
Método: Oestudoenvolveu456adolescentescomidadesentre11eanos.Elespreencheram
questionáriossobreadietamediterrânea(KIDMED),atividadefísica(QuestionáriodeAtividade
FísicaparaCrianc¸asmaisvelhas,PAQ-C)equalidadedevida(KIDSCREEN-27).Foicalculadoo
índicedemassacorporal.Análisesderegressãolinearhierárquicaforamutilizadaspara
deter-minarseaqualidadedevidarelacionadaàsaúdepodeserprevistapelasvariáveismedidas.
Asvariáveisforamintroduzidasdeformagradualcomadietamediterrâneanaprimeiraetapa,
índicedemassacorporalnasegundaetapaeatividadefísicanaterceira.
Resultados: Adieta mediterrânearepresentou4,6%davariâncianaqualidadede vida
rela-cionadaàsaúdedosadolescentes,eumamaioradesãoàdietamediterrâneafoipreditivade
maioresescoresdequalidadedevidarelacionadaàsaúde.Oíndicedemassacorporal
repre-sentouumadicionalde4,1%devariância,eummaioríndicedemassacorporalfoipreditivode
menoresescoresdequalidadedevidarelacionadaàsaúde.Porfim,aatividadefísica
repre-sentouumadicionalde11,3%davariância,eummaiorníveldeatividadefísicafoiassociadoa
maioresescoresdequalidadedevidarelacionadaàsaúde.Juntas,essasvariáveisrepresentam
20%davariâncianaqualidadedevidarelacionadaàsaúdedosadolescentes.
Conclusões: Aatividadefísica,oíndicedemassacorporaleaadesãoàdietamediterrâneasão
importantescomponentesparaconsideraraovisarmelhoriasnaqualidadedevidarelacionada
àsaúdedosadolescentes,sendoaatividadefísicaocomponentecommaiorinfluência.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo
OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Duringadolescence,cognitive,physical,psychological,and emotional changes take place that can affect health and well-being.1 Health-related quality of life (HRQoL) is a
multi-dimensional construct that describes well-being in
physical,psychological,andsocialterms.2
TheWorldHealthOrganizationestimatesthat35million
childrenindevelopingcountriesareoverweightorobese.3
Comparedtohealthyweightchildrenandadolescents,those
whoareobeseare morelikelytodevelop severalchronic
diseases, such as an unhealthy lipid profile, insulin
resis-tance, and metabolic syndrome.4 Also, evidence suggests
that adolescents with excess weight report poor overall
HRQoLrelativetohealthyweightadolescents.5
Levels of physical activity (PA) have been shown to
declineduringadolescence,makingthisanimportant
life-stageduringwhichtofocusresearch.6Someofthebenefits
ofPAincludereductionsinbloodcholesterol,hypertension,
metabolic syndrome, obesity,and reduced risk of
prema-ture deathin adolescents.Participation inPA can alsobe
importantfor ensuringgoodmentalhealth.7 Moreintense
andfrequent PAis associatedwithlower depression,
ten-sion,andfatigueinchildrenandadolescents.8Althoughfew
studieshaveinvestigatedtherelationshipbetweenPAand
HRQoLinadolescents,someevidenceexistsrelatinghighPA
withhighHRQoL.9
Establishinghealthynutritionalbehaviorsis also
impor-tant during adolescence, since the healthy nutrition
practices established in this period often persist into
adulthood.10 FollowingaMediterranean diet(MD),
charac-terizedbyhighconsumptionofoliveoil,fruits,vegetables,
wholegrains,moderate tohigh consumptionof fish,
mod-erate consumption of milk and dairy products, and low
consumptionofmeatandmeatproducts hasbeenrelated
with weight loss, reduced abdominal obesity and insulin
resistance, and lower risk of diabetes mellitus and
car-diovasculardiseases.Onlyafew studieshave investigated
the association between MD and HRQoL in adults11 or
adolescents,12findingMDtobepositivelyassociated.
TogainabetterunderstandingofHRQoLduring
aimofthisstudywastoexaminethe associationbetween
bodymassindex(BMI),PA,adherencetotheMD,andHRQoL
inasampleofSpanishadolescents.Thisstudymayprovide
evidenceandatheoreticalbasisonwhichtodevelop
strate-giestoimprovetheHRQoLofSpanishadolescents.
Methods
Subjects
Participantswererecruitedfromtheirschoolstoparticipate in this cross-sectional research. Between 2014 and 2015, therewere 20,929 adolescents enrolled in schools across Granada.Thestudyinvolved456adolescentsagedbetween 11and14years,ofwhom235weregirlsand221,boys.Data werecollectedbetweenMarchandMayin2014.Power anal-ysissuggestedthatthestudyrequiredaminimumsampleof 378adolescenttoachievesufficientpowerwitha95% confi-denceinterval(˛:0.05;ˇ:0.2).Fiveofthe55publicschools inthecitycenterofGranada(Spain)wererandomlyselected toparticipateinthisresearch.Allparticipatingschoolswere inamedium-highsocioeconomicareabasedoninformation containedintheEducationalProjectofthecenterorschool. Alladolescentsfromthefiveschoolsagedbetween11and 14 years(n=511) were invitedto take part in this study. Ofthese,480 agreed toparticipateand written informed consentwasreceivedfromtheirparentorguardian. Twenty-fouradolescentswereexcludedforfailingtocompletesome elementoftesting, orbecausetheyfailedtoattendclass ontheirtestingday.Boththeadolescentsandtheirparents or guardians were informed of the objectives and meth-ods of the study and told that they could withdraw at anytime.Participantswereinstructedonhowtocomplete thequestionnairesandhowtoconduct thetests.Alltests wereconductedduringtheparticipants’physicaleducation lessonsduringschooltime.Noincentiveswereprovidedto adolescentsorparents.Aresearchassistantwasalsoonhand to provide guidance on the completion of questionnaires andconductphysicaltesting.Ethicalapprovalwasgranted bytheEthicsCommitteeoftheUniversityofGranada.The ethicalprinciplesoftheDeclarationofHelsinkiformedical researchwereadheredto.
HRQoL
ToassessHRQoL,theKIDSCREEN-27questionnairewasused. Thisinternationallyvalidatedinstrument13isapplicablefor
healthy and chronically ill children and adolescents aged
from8to18 years.The KIDSREEN-27 consistsof 27items
acrossfivecomponents(physical well-being,psychological
well-being,autonomyandparent’srelation,socialsupport
and peers,and schoolenvironment). Internal consistency
of the subscales was between 0.81 and 0.84, and
test-retestreliabilityrangedfrom0.61to0.74.14Theresponses
werescoredandanalyzedaccordingtostandardalgorithms.
The recommended syntax steps were performed,
includ-ing transforming Rasch person parameter estimates into
z-values,yieldingscalescoresasT-valueswithmean(±SD)
scores of 50±10 define normality for children and
adolescentsaged8---18 yearsacross Europe.Higherscores
indicatehigherHRQoL.
Anthropometricmeasurement
Height andweightweremeasured following theprotocols established by the International Society for the Advance-ment of Kinanthropometry15 using a stadiometer (GPM,
Seritex, Inc., NJ, USA) with ±1mm accuracy) and an
electronic scale model 707 (Seca®, MD, USA) with ±50g
accuracy; BMI wascalculatedasweightdivided by height
squared (kg/m2). Overweight and obesity were defined
accordingtointernationalcriteria.16
PA,maximaloxygenuptake,andscreentime
PAlevelswereevaluatedusingthePhysicalActivity Ques-tionnaire for Older Children (PAQ-C). The questionnaire providesa generalmeasure ofPA for 8---20 year-olds.The PAQ-Cisaself-administeredquestionnaireconsistingofnine items ratedona five-pointscale. The finalPAQ-C activity summary scorewascalculatedfromthemeanof thenine items.Fivewasthereforethehighestpossiblescoreandone thelowest,withascoreoffiveindicatinghigh PAandone indicatinglowPA.Respondentsareaskedtorecallthe fre-quencyandtypeofPAtheyhaveengagedinoneachofthe sevendayspriortocompletingthequestionnaire.Validation studieshavefoundthePAQ-Ctobehighlyreliable.17 Based
onthesescores, thesample wasclassified intoPAtertiles
(low,medium,andhigh).
Maximal oxygen uptake (VO2max) was estimated using
a20mincremental-maximumeffortshuttle runfieldtest.
The test involves running to and fro between two lines
placed 20m apart.Participants start atan initial velocity
of8.5km/handincreasetheirspeedby0.5km/h/minuntil
theycannolongerreachthelineontwoconsecutive
occa-sions or when the participantcan nolonger maintain the
physical effort required to continue. VO2max relative to
bodymass(mL/kg/min)wascalculatedusingtheestablished
formula.18
Todetermine sedentaryscreen time,participantswere
asked to report the number of hours per day they
spentwatchingTV/DVDs,computerscreens,smartphones,
tablets,orotherdevices.
AdherencetotheMD
AdherencetotheMDwasassessedusingtheEvaluationof theMediterraneanDietQualityIndex(KIDMED),19whichwas
created toestimate adherence tothe MDin children and
youngadults.Thetestiscomprisedof16dichotomousitems
(yes/no),ofwhichtwelveitemsdescribebehaviors
consis-tent with the MD,e.g., ‘‘do you use olive oil at home?’’
andfouritemsdescribebehaviorsinconsistentwiththeMD,
e.g.,‘‘doyouconsumesweetsandcandyseveraltimesevery
day?’’ Affirmative answers to MD-consistent and
inconsis-tentbehaviorswerescored+1and−1,respectively,giving
amaximum possiblescoreof12.AccordingtotheKIDMED
Healthpromotioninapediatricpopulation 409
in need of improvement (4---7 points), or low quality(≤3
points).
Statisticalanalysis
Means and standard deviations are reported for all variables. Normality of the data was tested using the Kolmogorov---SmirnovtestwiththeLillieforscorrectionand homoscedasticitywasassessedusingtheLevenetest.After verifyingthatthevariableswerenotnormallydistributed, thedatawereanalyzedusingtheMann---WhitneyU-testfor two-groupcomparisonandtheKruskal---Wallistestfor three-groupcomparisons. Hierarchicallinearregressionanalyses wereusedtodetermine whetherHRQoL inchildren could bepredictedbythemeasuredvariables.MDwasenteredin astepwisemannerinthefirststep,BMIinthesecondstep, andPAinthethirdstep.TheSPSSStatisticsforWindows(IBM SPSSStatisticsforWindows,version22.0.NY,USA)wasused toanalyzethedatawith˛setat0.05.
Results
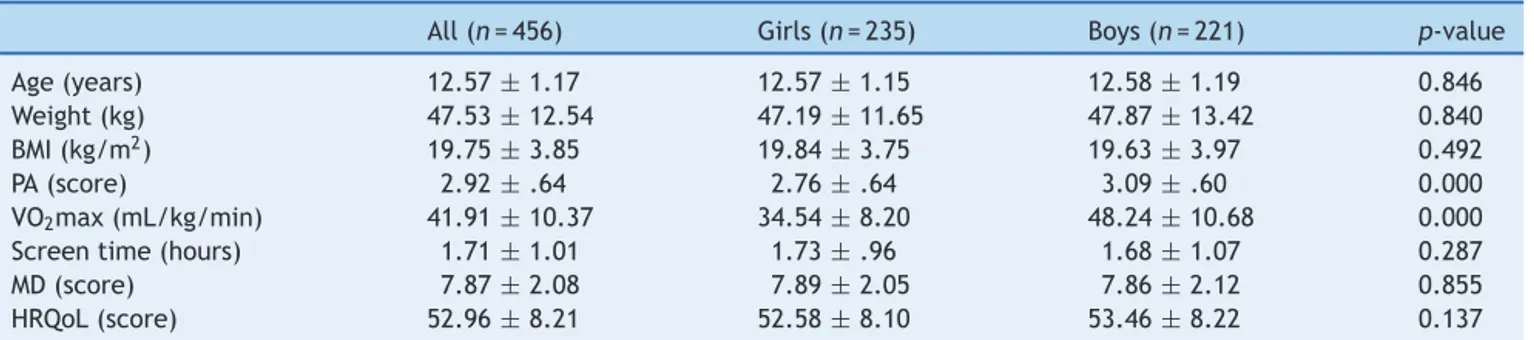
Descriptivecharacteristicsfor thestudy sampleareshown inTable1.TheMann---WhitneyU-testshowedthatreported
scoresforPAQ-CandVO2maxweresignificantlyloweringirls
thaninboys.Nosignificantdifferenceswerefoundforthe
othervariables.
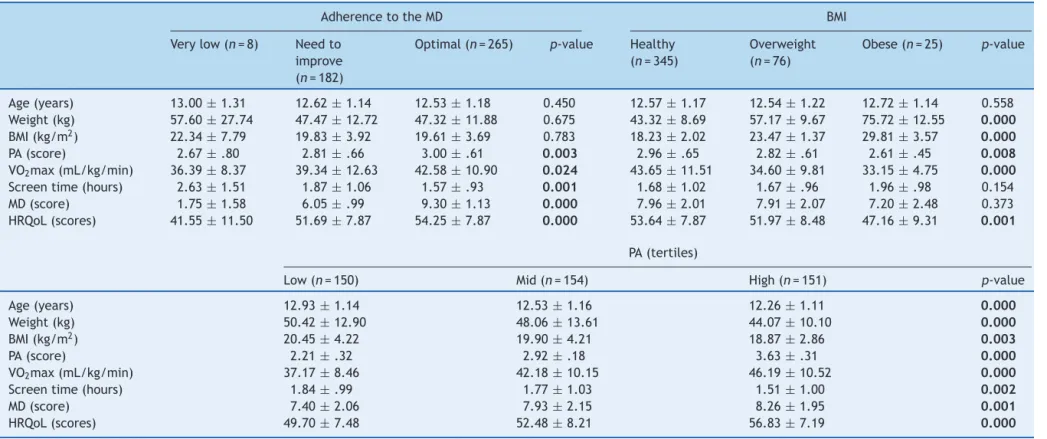
Table2showsthedescriptivecharacteristicsofthe
sam-pleaccordingtoadherencetotheMD,BMI,andPA.Analysis
accordingtoadherencetotheMDrevealedsignificant
differ-encesforPA,VO2max,andHRQoL,withhigherMDadherence
showingapositiverelationshipinallcases.Adolescentswith
higheradherencetotheMDalsoreportedlowerscreentime.
AnalysisaccordingtoBMIshowedsignificantlyhighervalues
ofPA,VO2max,andHRQoLinhealthyweightadolescentsin
comparisonwithoverweightorobeseadolescents.Interms
ofPA,adolescentswhoengagedinmorePApresented
sig-nificantlyhigherVO2max,adherencetotheMD,andHRQoL,
aswellassignificantlylowerweight,BMI,andscreentime.
Table 3 presents results from the hierarchical
regres-sion.MDaccountedfor4.6%ofthevarianceinadolescent’s
HRQoL. Higher adherence tothe MD was associated with
higherHRQoLscores.BMIaccountedforafurther4.1%ofthe
variance,withahigherBMIpredictinglowerHRQoLamong
adolescents.Finally,PAexplainedanadditional11.3%ofthe
variancein adolescent’sHRQoL,with ahigher levelof PA
beingassociatedwithhigherHRQoLscores.Together,these
variablesexplained20%ofthevarianceintheadolescents’
HRQoL.
Discussion
Totheauthors’knowledge,thisisthefirststudytoanalyze theassociationbetweenacombinationofadherencetoMD, BMI,andPAonHRQoLduringthefirststageofadolescence. Themainfindingofthepresentstudyisthathealthylifestyle behaviorsarereasonablygoodpredictors ofHRQoLduring adolescence(togetheraccountingfor20%ofthevariance). Inaddition,thestrongestmeasuredpredictorofHRQoLwas PA,whichexplained11.3%ofthevariance,morethan adher-encetoMDandBMIcombined.
Fewstudieshavestudiedtheassociationbetween adher-encetotheMDandHRQoL.Previousstudiesinadultshave found self-perceived mental and physical function to be directlyassociatedwithadherencetotheMD.11 Duringthe
period of adolescence, only one recent study conducted
in Greece has revealed a significant positive association
betweenadherencetotheMDandHRQoL(Beta=0.210).12
Consuming a MD has been inversely associated with
vari-ous chronic diseases.20 Furthermore, adolescents who do
nottypicallyconsumeaMDtendtohavealower
socioeco-nomicstatus.19 As aresult, theytend tohave less access
to some of the healthy components of the MD, such as
fruits,vegetables, fish,or olive oil. Lowersocioeconomic
statushasbeenassociatedwithpoorerphysicalandgeneral
health.21Consideringthatthemajorityofthepresent
sam-plelivedinmedium-highsocioeconomicareas,thesefactors
areunlikelyhaveexertedalargeinfluenceonthefindings.
IndividualsfollowingaMDarealsomorelikelytoengagein
otheraspectsoftheMediterraneanlifestyle,suchasusing
lunchtimeforsocialcommunicationwithfamilyandfriends.
Thismayatleastpartiallyexplaintherelationshipsbetween
adherencetotheMDandsocialaspectsoftheHRQoL.
Theresults regardingBMIandHRQoLarecontroversial.
This study found a higher BMI to be related with lower
HRQoL.PreviousstudiescomparingpediatricHRQoLacross
different BMI weight categories of adolescents have not
foundsignificantdifferencesaccordingtoweightcategory.22
Incontrast,otherstudieshavefoundthatobeseadolescents
Table1 Baselinecharacteristicsofadolescents.
All(n=456) Girls(n=235) Boys(n=221) p-value
Age(years) 12.57±1.17 12.57±1.15 12.58±1.19 0.846
Weight(kg) 47.53±12.54 47.19±11.65 47.87±13.42 0.840
BMI(kg/m2) 19.75±3.85 19.84±3.75 19.63±3.97 0.492
PA(score) 2.92±.64 2.76±.64 3.09±.60 0.000
VO2max(mL/kg/min) 41.91±10.37 34.54±8.20 48.24±10.68 0.000
Screentime(hours) 1.71±1.01 1.73±.96 1.68±1.07 0.287
MD(score) 7.87±2.08 7.89±2.05 7.86±2.12 0.855
HRQoL(score) 52.96±8.21 52.58±8.10 53.46±8.22 0.137
Datashownasmean±SD.
BMI,bodymassindex;PA,physicalactivity;VO2max,maximaloxygenuptake;MD,Mediterraneandiet;HRQoL,health-relatedquality
Muros
JJ
et
al.
Table2 CharacteristicoftheadolescentsbyadherencetotheMediterraneandiet,bodymassindex,andphysicalactivity.
AdherencetotheMD BMI
Verylow(n=8) Needto
improve
(n=182)
Optimal(n=265) p-value Healthy
(n=345)
Overweight
(n=76)
Obese(n=25) p-value
Age(years) 13.00±1.31 12.62±1.14 12.53±1.18 0.450 12.57±1.17 12.54±1.22 12.72±1.14 0.558
Weight(kg) 57.60±27.74 47.47±12.72 47.32±11.88 0.675 43.32±8.69 57.17±9.67 75.72±12.55 0.000
BMI(kg/m2) 22.34±7.79 19.83±3.92 19.61±3.69 0.783 18.23±2.02 23.47±1.37 29.81±3.57 0.000
PA(score) 2.67±.80 2.81±.66 3.00±.61 0.003 2.96±.65 2.82±.61 2.61±.45 0.008
VO2max(mL/kg/min) 36.39±8.37 39.34±12.63 42.58±10.90 0.024 43.65±11.51 34.60±9.81 33.15±4.75 0.000
Screentime(hours) 2.63±1.51 1.87±1.06 1.57±.93 0.001 1.68±1.02 1.67±.96 1.96±.98 0.154
MD(score) 1.75±1.58 6.05±.99 9.30±1.13 0.000 7.96±2.01 7.91±2.07 7.20±2.48 0.373
HRQoL(scores) 41.55±11.50 51.69±7.87 54.25±7.87 0.000 53.64±7.87 51.97±8.48 47.16±9.31 0.001
PA(tertiles)
Low(n=150) Mid(n=154) High(n=151) p-value
Age(years) 12.93±1.14 12.53±1.16 12.26±1.11 0.000
Weight(kg) 50.42±12.90 48.06±13.61 44.07±10.10 0.000
BMI(kg/m2) 20.45±4.22 19.90±4.21 18.87±2.86 0.003
PA(score) 2.21±.32 2.92±.18 3.63±.31 0.000
VO2max(mL/kg/min) 37.17±8.46 42.18±10.15 46.19±10.52 0.000
Screentime(hours) 1.84±.99 1.77±1.03 1.51±1.00 0.002
MD(score) 7.40±2.06 7.93±2.15 8.26±1.95 0.001
HRQoL(scores) 49.70±7.48 52.48±8.21 56.83±7.19 0.000
Datashownasmean±SD.
Healthpromotioninapediatricpopulation 411
Table3 Factorsassociatedwithhealth-relatedqualityoflife(totalscore)inchildren---multiplehierarchicalregressionanalysis
(n=456).
Predictorvariable StandardizedBeta R R2 R2 F F
Step1 0.215 0.046 0.046 21.323a
MD 0.215a
Step2 0.295 0.087 0.041 20.868a 16.516a
MD 0.202a
BMI −0.202a
Step3 0.447 0.200 0.113 36.432a 61.782a
MD 0.142b
BMI −0.140b
PA 0.348a
BMI,bodymassindex;PA,physicalactivity;MD,Mediterraneandiet.
a p<0.001. b p<0.01.
havelowerHRQoLthanhealthyweightadolescents.23Many
overweight adolescents may experience weight-related
stigmaandsocialdiscriminationasaresultofcarryingexcess
weight,whichcoulddiminishtheirHRQoL.24
The present study also identified high levels of PA to
berelated tohigh HRQoL,in congruence withother
pub-lishedresearch.25Onepreviousprospectivestudyshoweda
bidirectionalassociation betweenPAandHRQoLin
adoles-centsinwhichtotalPAengagementstronglypredictedhigh
HRQoL,andpositive HRQoLpredicted engagementin
rec-ommendedPAlevels.26Thismaybearesultofthepositive
influenceofPAonpsychologicalandsocialfunctioning,and
protectionfromdepression.27
PAhadastrongerinfluencethanadherencetotheMDand
BMIandshouldbeconsideredasthemainfocusof
interven-tiontargetingHRQoLinadolescents.Arecentintervention
study involving overweight andobese adolescents
investi-gated correlationsbetween changes in HRQoL andBMI or
PA aftera 24-month weight-lossprogram. Results showed
that long-term changes in PA explained 30% of the
varia-tioninoverallHRQoL(p=.01),whereaschangesinBMIwere
notassociatedwithachangeinHRQoL.Thisindicatesthat
PAmayhaveapositiveinfluenceonHRQoLevenwithouta
substantialchangeinbodycomposition.28
One limitation of the present research is its
cross-sectionaldesign,whichinhibits theinvestigationofcausal
relationships.Furthermore,theuseofself-reporttoassessa
numberofthevariablesincreasesthepossibilityof
measure-menterror. However,asboththe PAQ-CandKIDMEDhave
previouslydemonstratedhighvalidityandreliabilityinthis
population,thisshouldhavelittleimpactontheconclusions
made. Also,itwasnot possible toevaluatethe
socioeco-nomic status (SES) of individuals in the study.All schools
weresituatedinamedium-highsocioeconomicareabased
oninformationcontainedintheEducationalProjectofthe
center or school. As a result, the schools should at least
becomparable;however,futurestudiesshouldmeasureSES
wherepossible.
Despite these limitations, to the best of the authors’
knowledge, this is the first study to analyze associations
between MDadherence, PA,and BMIonHRQoLin
adoles-cents.
Thisstudy suggeststhatPA,BMI,andadherencetothe
MDareimportantcomponents toconsiderwhentargeting
improvementsintheHRQoLofadolescents,withPA
repre-sentingthecomponentwiththegreatestinfluence.Policies
thatpromote theMD andrecommend PAareexpected to
improve HRQoL in adolescents. Longitudinal studies are
needed tofurther explore the association between these
componentswithregardstoHRQoL.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Patton GC, Viner R. Pubertal transitions in health. Lancet. 2007;369:1130---9.
2.TestaMA,SimonsonDC.Assessmentofquality-oflifeoutcomes. NEnglJMed.1996;334:835---40.
3.WorldHealthOrganization.Population-basedprevention strate-giesforchildhoodobesity.Geneva:WHOPress;2010.
4.CatenacciVA, HillJO, WyattHR. Theobesity epidemic. Clin ChestMed.2009;30:415---44.
5.Ul-HaqZ,MackayDF,FenwickE,PellJP.Meta-analysisofthe associationbetweenbodymassindexandhealth-related qual-ityoflifeamongchildrenandadolescents,assessedusingthe pediatricqualityoflifeinventoryindex. JPediatr. 2013;162, 280---286.e.1.
6.Dumith SC, GiganteDP,Domingues MR,KohlHW III. Physical activitychangeduringadolescence:asystematicreviewanda pooledanalysis.IntJEpidemiol.2011;40:685---98.
7.JanssenI,LeBlancAG.Systematicreviewofthehealth bene-fitsofphysicalactivityandfitnessinschool-agedchildrenand youth.IntJBehavNutrPhysAct.2010;7:40.
8.Cheung SY, MakJY, Chan J. Children’s physical activity par-ticipation and psychological well being. Res Q Exerc Sport. 2008;79:A30.
9.ChenG,RatcliffeJ,OldsT,MagareyA,JonesM,LeslieE.BMI, healthbehaviors,andqualityoflifeinchildrenandadolescents: aschool-basedstudy.Pediatrics.2014;133:e868---74.
11.Henríquez Sánchez P, Ruano C, de Irala J, Ruiz-Canela M, Martínez-González MA,Sánchez-Villegas A. Adherencetothe MediterraneandietandqualityoflifeintheSUNProject.EurJ ClinNutr.2012;66:360---8.
12.CostarelliV,KoretsiE,GeorgitsogianniE.Health-relatedquality oflifeofGreekadolescents:theroleoftheMediterraneandiet. QualLifeRes.2013;22:951---6.
13.Ravens-Sieberer U, Gosch A, Rajmil L, Erhart M, Bruil J, DuerW,et al.KIDSCREEN-52quality-of-lifemeasurefor chil-dren andadolescents.Exp RevPharmacoecon OutcomesRes. 2005;5:353---64.
14.The KIDSCREEN Group Europe. The KIDSCREEN Question-naires --- Quality of life questionnaires for children and adolescents. Handbook. Lengerich:PabstScience Publishers; 2006.
15.StewartA,Marfell-JonesM,OldsT,HansdeRidderJ. Interna-tionalstandardsforanthropometricassessment.NewZealand: ISAK,LowerHut;2011.
16.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standarddefinitionforchildoverweightandobesityworldwide. IntSurvBMJ.2000;320:1240---3.
17.Saint-Maurice P,Welk GJ, BeylerNK, Bartee RT, Heelan KA. Calibrationofself-reporttoolsfor physicalactivityresearch: thePhysicalActivityQuestionnaire(PAQ).BMCPublicHealth. 2014;14:461.
18.Léger LA, MercierD, GadouryC,LambertJ. The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci. 1988;6:93---101.
19.Serra-MajemL, Ribas L,Ngo J,Ortega RM,GarcíaA, Pérez-Rodrigo C, et al. Food, youth and the Mediterranean diet in Spain, Development of KIDMED, Mediterranean diet qual-ity index in children and adolescents. Public Health Nutr. 2004;7:931---5.
20.DomínguezLJ,Bes-RastrolloM,delaFuente-ArrillagaC,Toledo E,Beunza JJ,Barbagallo M,et al.Similarpredictionoftotal mortality, diabetes incidence or cardiovascular events using relative- and absolute-component Mediterranean diet score: TheSUNcohort.NutrMetabCardiovascDis.2013;23:451---8. 21.KunstA,BosV,LahelmaE,BartleyM,LissauI,RegidorE,etal.
Trendsinsocio-economicinequalitiesinself-assessedhealthin 10Europeancountries.IntJEpidemiol.2005;34:316---26. 22.Gandhi PK, Revicki DA, Huang IC. Adolescent body weight
and health-related quality of life rated by adolescents and parents:theissue ofmeasurement bias.BMC PublicHealth. 2015;15:1192.
23.WilliamsJ, Wake M,Hesketh K, Maher E,Waters E. Health-relatedqualityoflifeofoverweightandobesechildren.JAm MedAssoc.2005;293:70---6.
24.Puhl RM, Brownell KB. Confronting and coping with weight stigma:aninvestigationofoverweightandobeseadults. Obe-sity.2006;14:1802---15.
25.SpenglerS,WollA.Themorephysicallyactive,thehealthier? Therelationshipbetweenphysicalactivityandhealth-related qualityoflifeinadolescents:theMoMostudy.JPhysActHealth. 2013;10:708---15.
26.Omorou AY,Langlois J, Lecomte E, Brianc¸on S, VuilleminA. Cumulative and bidirectional association of physical activity andsedentarybehaviourwithhealth-relatedqualityoflifein adolescents.QualLifeRes.2016;25:1169---78.
27.HallgrenM,HerringMP,OwenN, DunstanD,EkblomÖ, Hel-gadottir B, et al. Exercise,physical activity, and sedentary behaviorinthetreatmentofdepression:broadeningthe scien-tificperspectivesand clinicalopportunities.FrontPsychiatry. 2016;7:36.