Pleasecitethisarticleinpressas:VieiraC,etal.Ischemicruptureoftheanterolateralpapillarymuscle.RevPortCardiol. 2013.http://dx.doi.org/10.1016/j.repc.2012.06.014
ARTICLE IN PRESS
+Model
REPC-231; No.ofPages4
RevPortCardiol.2013;xxx(xx):xxx---xxx
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
www.revportcardiol.org
CASE
REPORT
Ischemic
rupture
of
the
anterolateral
papillary
muscle
Catarina
Vieira
a,∗,
António
Gaspar
a,
Miguel
Álvares
Pereira
a,
Nuno
Salomé
a,
Jorge
Almeida
b,
Mário
Jorge
Amorim
baDepartmentofCardiology,HospitaldeBraga,Braga,Portugal
bDepartmentofCardiothoracicSurgery,HospitaldeSãoJoão,Oporto,Portugal
Received25May2012;accepted4June2012
KEYWORDS
Papillarymuscle; Rupture;
Surgical reimplantation; Echocardiography
Abstract We describe the case of a59-year-old man who presented with chest pain and ST-segmentelevationintheinferiorleads,R>SinV1andSTdepressionintheanteriorleadsdue toproximalocclusionofthefirstobtusemarginal.Primarycoronaryangioplastyandstentingof thisarterywereperformed.Twelvehourslaterthepatientbecamehemodynamicallyunstable andseveremitralregurgitationduetoruptureofoneoftheheadsoftheanterolateralpapillary musclewasdiagnosed.Emergencysurgerywasperformed(papillarymusclehead reimplanta-tion,mitralannuloplastywitharigidring,tricuspidannuloplastyandcoronaryarterybypass grafting).Onsurgicalinspection,itwasobservedthatthedetachedmuscleheadhadbecome trappedintheleftventriclebyasecondarycordattachedtotheotherhead.
This case isunusual in presentingtwo uncommon features ofischemic papillarymuscle: ruptureoftheanterolateralmuscleinmyocardialinfarctioninvolvingtheinferoposteriorwalls, andthefactthattherupturedmuscleheaddidnotprolapsebecauseithadbecometrappedin theleftventriclebysecondarycordattachment.
© 2012 SociedadePortuguesa de Cardiologia. Published by Elsevier España, S.L. All rights reserved.
PALAVRAS-CHAVE
Músculopapilar; Rutura;
Reimplantac¸ão cirúrgica; Ecocardiograma
Ruturaisquémicadomúsculopapilarântero-lateral
Resumo Apresentamosumcasodeumhomem,de59anosdeidade,admitidonoServic¸ode Urgênciapordortorácicaeelevac¸ãoSTnasderivac¸õesinferiores,r>semV1edepressãoSTnas derivac¸õesprecordiais,devidoaoclusãodaprimeiraobtusamarginal.Foirealizadaangioplastia primáriadessalesãocomimplantac¸ãodestentrevestido.Dozehorasdepois,odoente desen-volveinstabilidadehemodinâmica,tendosidodiagnosticadaumainsuficiênciamitralgravepor ruturadeumadascabec¸asdomúsculopapilarântero-lateral.Odoentefoisubmetidoa cirur-giaemergente(reimplantac¸ãodomúsculopapilarântero-lateral,anuloplastiamitralcomanel rígido,anuloplastiatricúspideerevascularizac¸ãomiocárdica).Ainspec¸ãocirúrgicarevelouque acabec¸amuscularrompidasemantinhapresaaoventrículoesquerdoporumacordasecundária quealigavaàoutracabec¸adomúsculopapilarântero-lateral.
∗Correspondingauthor.
E-mailaddress:cfvieira1982@hotmail.com(C.Vieira).
Pleasecitethisarticleinpressas:VieiraC,etal.Ischemicruptureoftheanterolateralpapillarymuscle.RevPortCardiol. 2013.http://dx.doi.org/10.1016/j.repc.2012.06.014
ARTICLE IN PRESS
+Model
REPC-231; No.ofPages4
2 C.Vieiraetal.
Estecasotemaparticularidadedeapresentar2característicasincomunsdaisquemiado mús-culopapilar: rutura domúsculo ântero-lateral num enfarte póstero-inferiore ofacto dea cabec¸ademúsculonãoprolapsarparaaaurículaesquerda,porseencontrarpresaaoventrículo esquerdoporumacordasecundária.
© 2012 SociedadePortuguesa de Cardiologia. Publicado por Elsevier España, S.L.Todos os direitosreservados.
Introduction
Papillary muscle rupture is an infrequent but often
catastrophicmechanical complicationofacutemyocardial infarction (MI) accounting for approximately 5% of early deaths.1The conditionmayresultinacutemitral regurgi-tation,acutepulmonaryedema,and/orcardiogenicshock.2 Despitehighoperativemortality,surgeryisindicatedas sur-vivalofmedicallytreatedpatientsisverylow.3
Wereportanuncommonpresentationofananterolateral papillarymuscle rupture successfully repaired by surgical reimplantationofoneofthepapillarymuscleheads.
Case
report
A 59-year-old man wasadmitted tothe emergency room withacutechestpain.The12-leadECG(Figure1)showedST elevationintheinferiorleads,R>SinV1andSTdepression intheanteriorleads.Thepatientwashemodynamically sta-bleandcardiacandpulmonaryauscultationswerenormal.
Coronary angiography showed obstruction of the prox-imal segment of the first obtuse marginal and significant stenosis (80%) of the proximal segment of the anterior descendingartery.Primarycoronaryangioplastyofthefirst obtuse marginal and implantation of a drug-elutingstent wereperformed. Twelve hourslater the patientsuddenly became hypotensive and tachycardic. Physical examina-tionrevealed a new3/6 holosystolic murmur at the apex and significant bilateral rales. Transthoracic echocardiog-raphyshowedseveremitralregurgitationduetoposterior mitral leaflet prolapse and an image of a mass in the left ventricle, which did not prolapse totally into the left atrium during systole, suggestive of an anterolateral papillary muscle head. Left ventricular size and function wererelativelynormalbuttheposteriorandinferiorwalls were hypokinetic. Moderate tricuspid regurgitation was noticed and pulmonary artery systolic pressure was esti-matedat60mmHg.
Thepatientbecameoliguric,withdeteriorationofrenal function,andsoanintra-aorticballoonwasplacedandhe wastransferred toacardiothoracicdepartment for emer-gencysurgery.
Intraoperative2D/3Dtransesophagealechocardiography confirmedruptureofoneoftheheadsoftheanterolateral papillarymuscle, leading toextensive prolapse of the P1 and P2 segments and causing severe mitral regurgitation
(Figures 2 and 3A and B; videos 1, 2 and 3). On surgical
inspection,itwasobservedthatthedetachedmusclehead
(Figure 4) had become trapped in the left ventricle by a
secondarycordattachedtotheotherhead.Papillarymuscle headreimplantation,mitralannuloplastywitharigidring, tricuspidannuloplastywithaSoveringringanddouble coro-naryarterybypassgrafting(CABG)(leftinternalmammary artery tofirstobtuse marginal and right internal thoracic arterytoanteriordescendingartery)wereperformed.
The postoperative period was complicated by noso-comial pneumonia but the patient recovered fully and was discharged home on the 18th day. Transthoracic echocardiographyperformed15daysaftersurgeryshowed preserved global leftventricular functionand mild mitral regurgitation.
Discussion
The posteromedialpapillarymuscleissupplied withblood fromtheposteriordescendingartery,while the anterolat-eral papillary muscle has a dual blood supply, from the leftanteriordescendingandleftcircumflexarteries.4---6This differenceinbloodsupplyexplainswhyruptureofthe pos-teromedial papillarymuscle is 6---12 timesmore common. On the other hand, rupture of the anterolateral papillary muscle is usually associated withanterolateral MI, rarely occurringinthecontextofinferiorMI,ashappenedinthe casepresented.7
Transthoracicechocardiographyisusefulinthediagnosis ofpapillarymusclerupture,withasensitivityof65---85%.8 A flail segment of the mitral valve and a severed papil-larymuscleorchordacanfrequentlybeseenmovingfreely withintheleftventricularcavity.However,insomecases, transthoracicechocardiographyisnotinformativeand trans-esophageal echocardiography is required to establish the diagnosis;thisismostlikelytooccurwhentherupturedhead does notprolapse intotheleftatrium,aswasobservedin ourpatient,afeaturereportedinupto35%ofcases.9
Emergencysurgical interventionremainsthetreatment ofchoiceforpapillarymusclerupture.Surgeryinvolves sig-nificant operative mortality (18%), but there are recent trendsforloweroperativerisk,particularlywithassociated CABG(8.7%).10Long-termoutcomeaftersurgeryisthesame as that of similar MI without papillary muscle rupture.10 Theseencouragingobservationsemphasizetheimportance ofpromptdiagnosisandanaggressivetherapeuticapproach forpatientssufferingpapillarymuscleruptureafterMI.
Pleasecitethisarticleinpressas:VieiraC,etal.Ischemicruptureoftheanterolateralpapillarymuscle.RevPortCardiol. 2013.http://dx.doi.org/10.1016/j.repc.2012.06.014
ARTICLE IN PRESS
+Model
REPC-231; No.ofPages4
Ischemicruptureoftheanterolateralpapillarymuscle 3
Figure 1 Electrocardiogram on admission demonstrating slight ST-segment elevation in the inferior leads, R>S in V1 and
ST-segmentdepressionintheanteriorleads.
Figure2 Two-dimensionaltransesophagealechocardiogramshowingseveremitralregurgitationcausedbyposteriorleaflet
pro-lapse.LA:leftatrium;LV:leftventricle.
LA
A
B
LV
LAA Ao
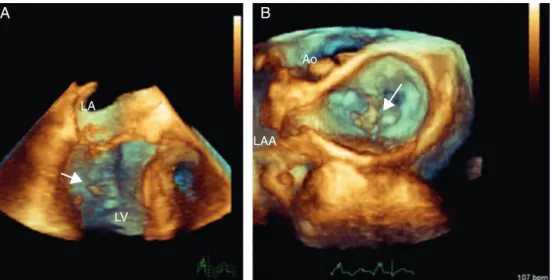
Figure3 Three-dimensionaltransesophagealechocardiography.(A)Fullvolumecroppedimageshowingthedetachedheadofthe
anteriorpapillarymuscleinside theLV(arrow)causingsevereprolapse oftheposterior leaflet;(B)3DZoomofthemitralvalve
Pleasecitethisarticleinpressas:VieiraC,etal.Ischemicruptureoftheanterolateralpapillarymuscle.RevPortCardiol. 2013.http://dx.doi.org/10.1016/j.repc.2012.06.014
ARTICLE IN PRESS
+Model
REPC-231; No.ofPages4
4 C.Vieiraetal.
Figure 4 Intraoperative view showing the forceps holding
thedetachedmusclehead.Thetwoprimarycordsconnecting
themuscleheadtotheedgeoftheposteriorleafletareclearly
seen.
hadbecometrappedintheleftventriclebyacord attach-ment.
Ethical
disclosures
Protection of human and animal subjects.The authors
declarethatnoexperimentswereperformedonhumansor animalsforthisstudy.
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdataandthatallthepatientsincludedinthe studyreceivedsufficientinformationandgavetheirwritten informedconsenttoparticipateinthestudy.
Righttoprivacyandinformedconsent.Theauthorshave
obtained the written informedconsent of thepatients or subjectsmentionedinthearticle.Thecorrespondingauthor isinpossessionofthisdocument.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Appendix
A.
Supplementary
data
Supplementary data associated with this article can be found, in the online version, at doi:10.1016/j.repc.
2012.06.014.
References
1.NishimuraRA,SchaffHV,ShubC,GershBJ,EdwardsWD,Tajik AJ. Papillary muscle rupture complicating acute myocardial infarction:analysisof17patients.AmJCardiol.1983;51:373---7. 2.SandersRJ,NeubuergerKT,RavinA.Ruptureofpapillary mus-cles:occurrenceofruptureoftheposteriormuscleinposterior myocardialinfarction.DisChest.1957;31:316---23.
3.KishonY,OhJK,SchaffHV,MullanyCJ,TajikAJ,GershBJ.Mitral valveoperationinpostinfarctionruptureofapapillarymuscle: immediateresultsandlong-termfollow-upof22patients.Mayo ClinProc.1992;67:1023.
4. Reeder GS. Identification and treatment ofcomplications of myocardialinfarction.MayoClinProc.1995;70:880.
5.LavieCJ,GershBJ.Mechanicalandelectricalcomplicationsof acutemyocardialinfarction.MayoClinProc.1990;65:709. 6.JamesTN.Anatomyofthecoronaryarteriesinhealthand
dis-ease.Circulation.1965;32:1020.
7.Voci P,Bilotta F,Caretta Q, Mercanti C,Marino B.Papillary muscleperfusionpattern. Ahypothesisfor ischemicpapillary muscledysfunction.Circulation.1995;91:1714---8.
8.Czarnecki A, Thakrar A, Fang T, et al. Acute severe mitral regurgitation:considerationofpapillarymusclearchitecture. CardiovascUltrasound.2008;6:5.
9.MoursiMH,BhatnagarSK,Vilacosta I,SanRomanJA,Espinal MA,NandaNC.Transesophagealechocardiographicassessment ofpapillarymusclerupture.Circulation.1996;94:1003. 10.RussoA,SuriRM,GrigioniF,etal.Clinicaloutcomeafter