w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Assessment
of
cardiovascular
risk
in
patients
with
rheumatoid
arthritis
using
the
SCORE
risk
index
Otávio
Augusto
Martins
de
Campos
a,
Nazaré
Otília
Nazário
b,
Sônia
Cristina
de
Magalhães
Souza
Fialho
c,
Guilherme
Loureiro
Fialho
d,
Fernando
José
Savóia
de
Oliveira
a,
Gláucio
Ricardo
Werner
de
Castro
a,e,
Ivânio
Alves
Pereira
a,e,∗aDisciplineofRheumatology,UniversidadedoSuldeSantaCatarina,Florianópolis,SC,Brazil bDepartmentofEpidemiology,UniversidadedoSuldeSantaCatarina,Florianópolis,SC,Brazil
cNucleusofRheumatology,TeachingHospital,UniversidadeFederaldeSantaCatarina,Florianópolis,SC,Brazil dNucleusofCardiology,TeachingHospital,UniversidadeFederaldeSantaCatarina,Florianópolis,SC,Brazil eNucleusofRheumatology,HospitalGovernadorCelsoRamosdeFlorianópolis,Florianópolis,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13November2014 Accepted15July2015
Availableonline29October2015
Keywords:
Rheumatoidarthritis Cardiovascularevents Cardiovascularrisk Riskfactors
a
b
s
t
r
a
c
t
Introduction:Rheumatoidarthritisisanautoimmunediseasethatcausessystemic involve-mentandisassociatedwithincreasedriskofcardiovasculardisease.
Objective:Toanalyzethepredictionindexof10-yearriskofafatalcardiovasculardisease eventinfemaleRApatientsversuscontrols.
Methods:Case–controlstudywithanalysisof100femalepatientsmatchedforageand gen-derversus100patientsinthecontrolgroup.Forthepredictionof10-yearriskofafatal cardiovasculardiseaseevent,theSCOREandmodifiedSCORE(mSCORE)riskindexeswere used,assuggestedbyEULAR,inthesubgroupwithtwoormoreofthefollowing:duration ofdisease≥10years,RFand/oranti-CCPpositivity,andextra-articularmanifestations. Results:TheprevalenceofanalyzedcomorbiditieswassimilarinRApatientscomparedwith thecontrolgroup(p>0.05).ThemeansoftheSCOREriskindexinRApatientsandinthe controlgroupwere1.99(SD:1.89) and1.56(SD:1.87)(p=0.06), respectively.Themeans ofmSCOREindexinRApatientsandinthecontrolgroupwere2.84(SD=2.86)and1.56 (SD=1.87)(p=0.001),respectively.ByusingtheSCOREriskindex,11%ofRApatientswere classifiedasofhighrisk,andwiththeuseofmSCOREriskindex,36%wereathighrisk (p<0.001).
Conclusion:TheSCOREriskindexissimilarinbothgroups,butwiththeapplicationofthe mSCOREindex,werecognizedthatRApatientshaveahigher10-yearriskofafatal cardio-vasculardiseaseevent,andthisreinforcestheimportanceoffactorsinherenttothedisease notmeasuredintheSCOREriskindex,butconsideredinmSCOREriskindex.
©2015ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](I.A.Pereira). http://dx.doi.org/10.1016/j.rbre.2015.09.005
Avaliac¸ão
do
risco
cardiovascular
de
pacientes
com
artrite
reumatoide
utilizando
o
índice
SCORE
Palavras-chave: Artritereumatoide Eventosvasculares Riscocardiovascular Fatoresderisco
r
e
s
u
m
o
Introduc¸ão:ArtriteReumatóide(AR)éumadoenc¸aautoimunequedeterminamanifestac¸ões sistêmicaseestáassociadaaaumentodoriscodeeventocardiovascular.
Objetivo: Objetiva-senesteestudoanalisaroíndicedepredic¸ãodeeventocardiovascular empacientesdogênerofemininoportadoresdeARcomparadosacontrolessemadoenc¸a. Métodos:Estudodecaso-controlecomanálisede100pacientespareadasporgêneroeidade versus100pacientesdogrupocontrole.Paraapredic¸ãodoriscodeeventocardiovascular fatalem10anos,utilizamososíndicesSCOREeSCOREmodificado(mSCORE),conforme sugeridopelaEULAR,nosubgrupocom2oumaisdosseguintes:durac¸ãodadoenc¸a≥10 anos,positividadeparafatorreumatoidee/ouanti-CCP,emanifestac¸õesextra-articulares. Resultados: AprevalênciadascomorbidadesanalisadasfoisimilarnaspacientescomAR, emcomparac¸ãocomogrupocontrole(p>0,05).AsmédiasdoíndiceSCOREforam1,99(DP: 1,89)e1,56(DP:1,87)nasportadorasdeARenoscontroles(p=0,06),respectivamente.Coma utilizac¸ãodoíndicemSCORE,naspacientescomARfoiencontradaamédiade2,84(DP:2,86) versus1,56noscontroles(DP:1,87)(p=0,001).AoutilizaroíndiceSCORE,11%dosportadores deARforamclassificadoscomodealtorisco;comoíndicemSCORE,36%obtiveramessa classificac¸ão(p<0,001).
Conclusões: OíndiceSCOREésemelhantenosdoisgrupos,mascomaaplicac¸ãodoíndice mSCORE,identificamosqueospacientescomARtêmmaiorriscodeeventocardiovascular fatalem10anos,comênfasenaimportânciadosfatoresinerentesàdoenc¸anãomensurados noíndiceSCORE,masconsideradosnoíndicemSCORE.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Rheumatoidarthritis(RA)isasystemicautoimmunedisease ofunknowncause characterizedmainlybythepresenceof synovialinflammation,cartilagedamageandarticular defor-mity.Thisdiseasealsodeterminessystemicmanifestations andisassociatedwithmultiplecomorbidities.1
Studies haveshown that the prevalence ofRA isabout 0.5–1%ofthepopulation,2,3andcardiovasculardiseaseisthe
leading cause of mortality in thesepatients. In a recently publishedmeta-analysis,theauthors foundthattheriskof mortality from cardiovascular disease (ischemic heart dis-ease and stroke) is 50% higher in RA patients compared to the generalpopulation.4 However, it is clear that early
atherosclerosis observed in this group of patients cannot be explained only by traditional cardiovascular risk fac-tors.Theformationofatheroscleroticplaques byachronic inflammatorydisease process cancomedirectly (actingon the formation and destabilization of plaque) or indirectly throughaorticstiffening,whichcan leadtoleft ventricular hypertrophy.5,6
Inthegeneralpopulation,anumberofcardiovascularrisk predictive scores has been used, such as the Framingham score and the Systematic Coronary Risk Evaluation index (SCORE),inanattempttopredictriskandactingpreventively toavoidunfavorableoutcomes.InRApatients,studiesonthe useofthesescoresarescarce.Accordingtothe recommenda-tionsoftheEuropeanLeagueAgainstRheumatism(EULAR), SCOREandmodifiedSCORE(mSCORE)riskindexesshouldbe usedforriskpredictioninthisspecificpopulation.
Thisstudyaimedtoanalyzethecardiovascularrisk pre-dictionindexaccordingtoSCOREandmSCOREindexesinRA patientscomparedtocontrolswithoutthedisease.
Methods
This case–control study was conducted atthe Movimento Clinic,acenterspecializedinrheumaticdiseases,atthe Ref-erencePolyclinicofUNSUL,andatthePrimaryHealthCare Group(ABS),locatedinthecityofPalhoc¸a(SC).
Medicalrecordsoffemalepatientsagedbetween35and70 yearsold,diagnosedwithRAandwhometthe1987disease classification criteria7 were analyzed. The control subjects
program,withthefollowingparameters:95%confidence inter-val (CI 95%); power of 80%; control/case ratio 1:1; rate of exposedcontrols:20%;rateofexposedcases:40%,totaling100 casesand100controls.
Subjectsmeetingthefollowingcriteria8–10wereconsidered
ascomorbiditycarriers:
1. Highblood pressure(BP):SBP≥140mmHg;DBP≥90mm Hg,oruseofantihypertensivemedication.Subjectswithat leastthreeofthesemeasurementsontwodifferent occa-sionswereconsideredaswithhypertension(accordingto VIBrazilianGuidelinesonHypertension,2010).
2. Dyslipidemia: LDL cholesterol≥130mg/dL; Total choles-terol≥200mg/dL; Triglycerides≥150mg/dL; HDL≤
40mg/dL; or use of statins (according to the classifi-cation of the Third Report of the National Cholesterol Education Program [NCEP] Expert Panel on Detection, Evaluation,and Treatment of HighBlood Cholesterol in Adults[AdultTreatmentPanelIII]FinalReport).
3. Diabetesmellitus(DM):fastingglucose≥126mg/dLintwo samples; glycaemia≥200mg/dL in a 2-h tolerance test (75gofglucose);randombloodglucoselevels≥200mg/dL;
glycated hemoglobin≥6.5% in 2 samples; use of hypo-glycemicagentsorinsulintherapy(accordingtoStandards ofMedicalCareinDiabetes–2011).
4. Smoking.
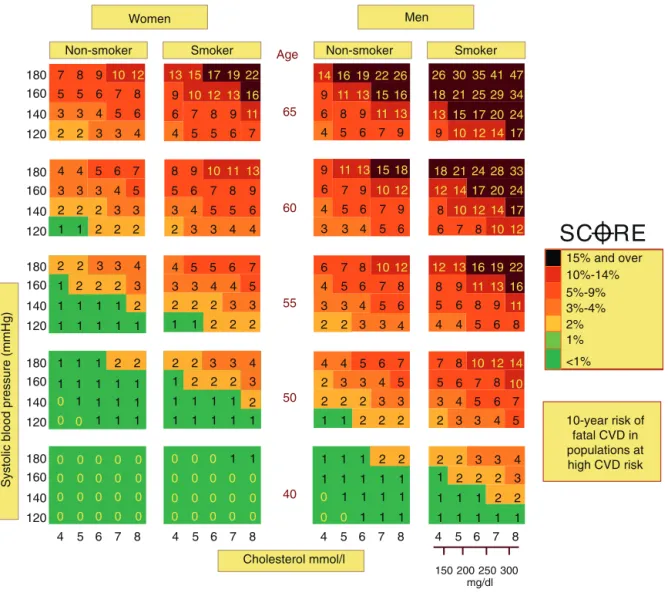
For cardiovascularriskprediction,weusedthehigh-risk SCOREindex(Fig.1)whichclassifiespatientsaccordingtoage, gender, totalcholesterollevel, systolic bloodpressure (SBP) andtobaccouse,usinglow-andhigh-riskmatrices.11
Cross-checkingofdataforeachpatientprovidesacellcontaininga numberrepresentingthenumericalvalueoftheSCORErisk index,andacolorrepresentingtherateof10-yearriskofa fatalcardiovasculardisease event,towhich eachpatientis exposed.
TocalculatethemSCOREriskindex,thevalueinitially col-lectedfromtheSCOREriskindexwasmultipliedbyafactorof 1.5forRApatientsthatmettwooutofthefollowingthree crite-ria:adiseaselastingmorethan10years,RFand/oranti-CCP positivity,andfinally,patientswithextra-articular manifesta-tions.
Based on calculations of SCORE and mSCORE indexes, patientswhowereclassifiedwithachance≥5%ofa10-year
180
Women Men
Non-smoker Smoker Non-smoker Smoker
160 140 120 180 160 140 120 180 160 140 120 180 160 140 120 180 0 0 0 0
0 0 0 0
0 0 0 0 0
0 0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 0 0 0 0
0 0 0
0 0 0
0 0 0 1 1
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1 1 1 1
2 2 2 2 2 2 2 2 2 2 2 2 2 2 2
2 2 2
2 2 2 2 2 2 2 2 2 2 2 2 4 4 4 4 4 4 4 2 3 4 4 4 3 3 3 3 4 4 4 4 3 3 3 3 3 3 3 3 3 3 2 2 2 2 2
2 2 2 2
2 2 2
2 2 2 2 3 4 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 4 4 4 4 4 4 4 4 4 4 5 5 5 5 5 5 6 6 6 7 6 7 7 7 7 5 5 5 3 3
3 4 4 5
3
4 5 5
5 5 5 5 5 6 6 6 9 6 6 6 6 6 6 6 6 6 8 8 8 8 8 8 8 8 8 9 9 9 9 9 8 9 9 9 7 7 7 7 7 7 7 7 7 2 3 5 5 6 6 5 5 5 5 5 7 6 6 9 9 9 9 9 6 8 8 8 8 8 7 6 5 7 1 1 0 0 10 12 10 11 16 19 17 15 22 13 13 11 12 10 11 16 13 11 16 19 10 22 12 17 17 47 41 35 30 26 26 17 17 14 14 14 15 13 12 20 20 22 24 24 34 33 28 24 21 29 25 21 18 18 12 10 12 10 13 12 12 10 12 18 10 15 13 16 14 11 19 16 15 13 13 11 11 14 10 13 12 10 160
Systolic blood pressure (mmHg)
140 120 Cholesterol mmol/l 40 50 55 60 65 Age
4 5 6 7 8 4 5 6 7 8 4 5 6 7 8 4
150 200 250 mg/dl
300
5 6 7 8
10-year risk of fatal CVD in populations at high CVD risk 15% and over
SCORE
10%-14% 5%-9% 3%-4% 2% 1% <1%Fig.1–SCOREriskindex.
Source:EuropeanGuidelinesonCVDPreventioninClinicalPractice(version2012).
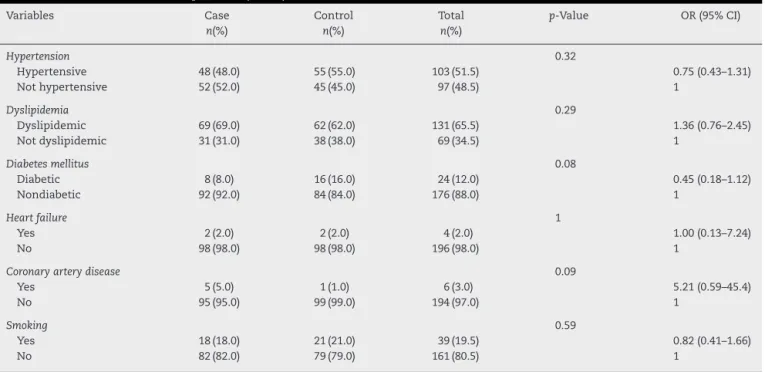
Table1–ComorbiditiesinRApatients(cases)andcontrols.
Variables Case Control Total p-Value OR(95%CI)
n(%) n(%) n(%)
Hypertension 0.32
Hypertensive 48(48.0) 55(55.0) 103(51.5) 0.75(0.43–1.31)
Nothypertensive 52(52.0) 45(45.0) 97(48.5) 1
Dyslipidemia 0.29
Dyslipidemic 69(69.0) 62(62.0) 131(65.5) 1.36(0.76–2.45)
Notdyslipidemic 31(31.0) 38(38.0) 69(34.5) 1
Diabetesmellitus 0.08
Diabetic 8(8.0) 16(16.0) 24(12.0) 0.45(0.18–1.12)
Nondiabetic 92(92.0) 84(84.0) 176(88.0) 1
Heartfailure 1
Yes 2(2.0) 2(2.0) 4(2.0) 1.00(0.13–7.24)
No 98(98.0) 98(98.0) 196(98.0) 1
Coronaryarterydisease 0.09
Yes 5(5.0) 1(1.0) 6(3.0) 5.21(0.59–45.4)
No 95(95.0) 99(99.0) 194(97.0) 1
Smoking 0.59
Yes 18(18.0) 21(21.0) 39(19.5) 0.82(0.41–1.66)
No 82(82.0) 79(79.0) 161(80.5) 1
riskofafatalcardiovasculardiseaseeventwerestratifiedas of“highrisk”.
ThedatabasewasdevelopedinExcelandexportedtoSPSS 16.0program.Statisticalanalysisinvolvedtheevaluationof normality ofquantitative variables. To verify the presence of an association between independent variables and the dependentvariable,thePearsonchi-squaredtestfor qualita-tivevariablesandtheStudent’sttestforquantitativevariables wereused.ORassociationmeasurewasusedwiththe respec-tive95%CIs.
ThestudywassubmittedtoResearchEthics Committee-UNISUL,havingreceivedapprovalforitsrealization.
Results
Dataof100medicalrecordsofRApatientswereincludedto composethecasegroup;anddataof100medicalrecordsof patientswithoutadiagnosisofRAwereincludedtomakeup thecontrolgroup.Allstudyparticipantswerefemale.
ThemeanageofRAgroupwas55.4±8.9years.Inthe con-trolgroup,themeanagewas52.3±7years.Themeanduration ofdiseaseinRApatientswas14±8years.AmongRApatients, 67%had a diagnosisofRAformore than10 years.26% of patientshadanextra-articularmanifestation(inmostcases, pulmonaryinvolvement).Table1liststheanalysisthat deter-mined the association between comorbiditiesof the study participants.Therewere nodifferencesinthefrequencyof comorbiditiesforbothRAandcontrolgroups.
Table 2 reports the differences between SCORE and
mSCOREriskindexmeans.ByanalyzingtheSCOREriskindex for10-yearriskofafatalcardiovasculardiseaseeventforall participantsstudied,thefollowingmeanswereobtained:1.99 (SD:1.89)forRAgroupand1.56(SD:1.87)forthecontrolgroup (p=0.06).UsingthemSCOREriskindex,thefollowingmeans wereobtained:2.84(SD=2.86)inRAgroupand1.56(SD1.87)in
thecontrolgroup,withstatisticalsignificanceforthisvariable (p=0.001).
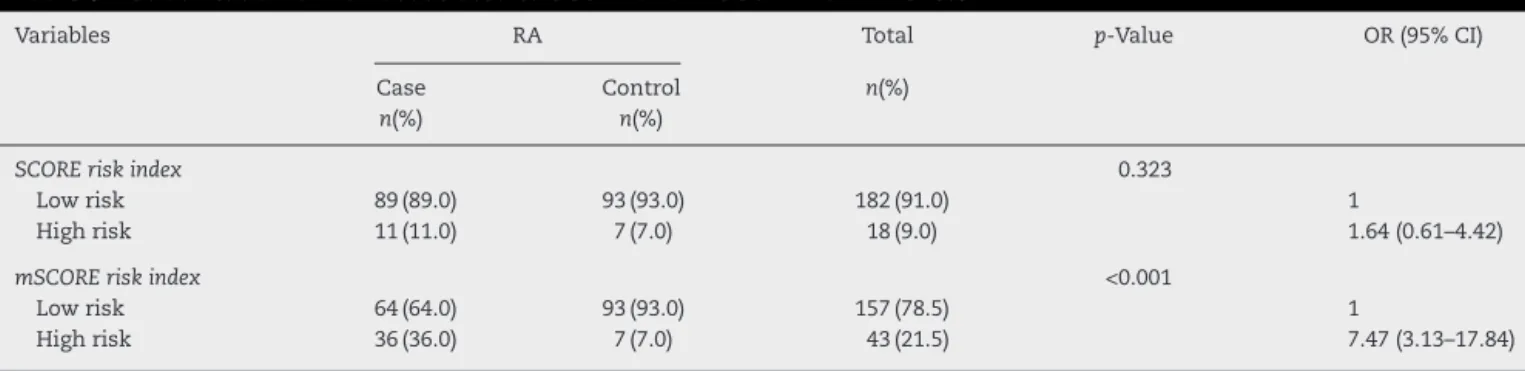
Table3liststheriskstratificationassociatingSCOREand mSCOREindexes.Thestratificationofpatientsstudiedinto subgroupswithhigh-andlow-riskfora10-yearriskofafatal cardiovascular disease event was based onthe SCORE risk index.Thisstratificationshowedthat11%ofRApatientsand 7%ofcontrolgroupsubjectswere classifiedasofhigh-risk (p=0.32).WhenusingthemSCOREforriskstratification,itwas observedthat36%ofRApatientsand7%inthecontrolgroup wereclassifiedasofhigh-risk(p<0.001).
Discussion
Inthisstudy,acomparativeanalysisofpatientswithand with-outRAwasdevelopedinordertoestablishSCOREandmSCORE riskindexesfor10-yearriskofafatalcardiovasculardisease eventinbothgroups.Atfirst,weidentifiedseveral comorbidi-ties oftenpresent instudiedgroupsand thatdefinitelyare relatedtoaworsecardiovascularprognosis.
Table2–MeansofSCOREandmSCOREriskindexesin casesandcontrols.
Variables RA p-Value
Case Control
Mean(SD) Mean(SD)
SCOREriskindex 1.99(1.89) 1.56(1.87) 0.062 mSCOREriskindex 2.84(2.86) 1.56(1.87) 0.001
Table3–StratificationofriskassociatedtoSCOREandmSCOREriskindexes.
Variables RA Total p-Value OR(95%CI)
Case Control n(%)
n(%) n(%)
SCOREriskindex 0.323
Lowrisk 89(89.0) 93(93.0) 182(91.0) 1
Highrisk 11(11.0) 7(7.0) 18(9.0) 1.64(0.61–4.42)
mSCOREriskindex <0.001
Lowrisk 64(64.0) 93(93.0) 157(78.5) 1
Highrisk 36(36.0) 7(7.0) 43(21.5) 7.47(3.13–17.84)
RA,rheumatoidarthritis;SCORE,SystematicCoronaryRiskEvaluation;mSCORE,modifiedSystematicCoronaryRiskEvaluation.
By analyzingthe presenceofhypertension inthe study subjects,theresultsshowedsimilarratesofthis comorbid-ityinbothgroups.Inameta-analysisbyBoyeretal.,12with15
case–controlstudiesselectedwith2956casesand2713 con-trols from 1950to2008,no differencewas observedinthe presenceofhypertensioninbothgroups.Althoughthereare inherentfactors which contribute to the increase ofblood pressure, for example, a lower endothelium-derived nitric oxideexpression,higherendothelinandangiotensinII pro-duction, and use of certain medications (e.g., leflunomide, nonsteroidal anti-inflammatory drugs and corticosteroids), thesefactorspersearenotenoughtodetermineadifferencein prevalenceofhypertensionamongRApatientsversuscontrols withoutthedisease.
Dyslipidemia was a common finding, but this finding wasnotmorefrequentthaninthecontrolgroup.Moreover, Urowitz13foundslightlyhigherlevelsoftotalcholesterolin
patientsdiagnosedwithRAwhencomparedtopatients with-outthedisease.Oneofthefeaturesofthelipidprofileofthese patientswasalsoobserved,thatis,bloodlevelsofHDLwere lowerthaninthegeneralpopulation.Tomsetal.14mention
thatsuchcomorbidityaffects55–65%ofRApatients,bothin early-stageandlate-stagedisease.Turningtheirattentionto bloodlevelsofHDLinthegroupsstudied,theseauthorsfound lower levels ofHDL in RA population. In this same study, theauthorsmentionthat,inadditiontogenetic predisposi-tion(whichmaybeapotentialcauseofdyslipidemiainthese patients),otherfactorswouldbeacting,suchasinflammatory diseaseactivity,physicalinactivityduetoillness,anduseof certainmedications.
Incomparisonwiththegeneralpopulation,patients diag-nosed with RA are at a twofold increasedrisk to suffer a cardiovascularevent;andthemagnitudeofthis increaseis comparabletotherisk ofcardiovascular eventsinpatients with type2 diabetes mellitus.15 Such figures reinforcethe
importanceofidentifyingRApatientsdiagnosedwith under-lyingDM,forthisknowledgecanavoidunfavorableoutcomes. In this study, in comparison with RA group, the control group showed a tendency for a twofold increased preva-lence of DM, but without statistical significance. Changes in blood glucose levels of RA patients can be explained by modifiable factors such as abdominal obesity, use of antihypertensive agents, disease activity, and the use of corticosteroids.16Inameta-analysisbyBoyeretal.,12the
fre-quencyof DM inRA patients washigher than that inthe
controlgroup(p=0.003);andotherstudiesalsofoundsimilar findings.17,18
Anotherimportantcomorbiditystudiedinthismanuscript was smoking, with a similar frequency in both case and controlgroups.Inahistoricalcohortstudy,Kremersetal.19
foundaprevalenceof52%ofsmokinginRApatients(p=0.004) andof43%inthegroupwithoutthedisease.Another meta-analysis, whichreinforcesthe higherfrequencyofsmokers in RA patients versus the general population, was con-ducted by Boyer et al.,12 with OR=1.56 (95% CI 1.35–1.80; p<0.00001).Itisbelievedthatthelowfrequencyofsmoking in RApatientscompared withhistoricalcohorts isderived from the more detailed information received by patients about the harmfuleffects ofthis habit;patients are aware that this habit would result in lower response to treat-ment, more severe disease and increased cardiovascular risk.
Thetoolsdesignedtoassesscardiovascularriskinthe gen-eralpopulation,suchastheFraminghamscore,cannotpredict theactualcardiovascularriskinRApatients,because,despite thekeyroleofinflammationinthedevelopmentof atheroscle-rosis, inclinical practice this factor isoverlooked in many riskstratificationtools.Crowsonetal.,20inastudyof525RA
patientsagedlessthan30years,analyzedFraminghamand Reynoldsscoresforassessmentofcardiovascularrisk.These authorsconcludedthatthesescoressubstantially underesti-matecardiovascularriskinRApatients(bothgenders),mainly inadvancedage,inRF-positivesubjects,andwithpersistently high ratesofESR,whichisanimportantmarkerof inflam-matory activityofthedisease.Suchoutcomescanresultin missed opportunities forpreventive medical interventions, andalsocreateafalsesenseofsecurityinmedicalpractice inthe predictionofthe actualcardiovascularrisktowhich patientsaresubjected.
Then,thegroupdevelopedasimplematrixforrisk calcu-lation,providingadirectestimate of10-year riskofafatal cardiovasculardiseaseeventinaformatsuitableforthe limi-tationsofclinicalpractice.21
InastudybyPetersetal.11thataimedtodevelop
evidence-basedrecommendationsfrom theEuropeanLeagueAgainst Rheumatism(EULAR)inRA,ankylosingspondylitisand pso-riatic arthritispatients, the orientationofthe authors was thatincountriesinwhichtherewasnoevaluationguidelines forcardiovascularriskinthesepopulations,theSCORErisk indexshouldbeused.InanotherstudyconductedbyRosales Alexanderetal.,22theauthorsobservedasignificant
associ-ationamongtheSCOREriskindexandCRPlevels(p<0.034), thepresenceofextra-articularmanifestations(p<0.048),more than 10 years of disease duration (p<0.001), suggesting a relationshipofcardiovascularriskandRAseveritywith cumu-lativeduration ofinflammationmaintainedoverthe years. ThesedataprovidedinformationthatallowedtheEULAR com-mitteeofexpertsmakeanadjustmentofcalculationsforthe SCOREriskindexforpatientswithatleasttwooutofthree ofthefollowingfactors(adiseasewith>10years,RFand/or anti-CCPpositivity,andpresenceofextra-articular manifes-tations),withtheuseofamultiplyingfactorof1.5toobtain themodifiedSCOREriskindex(mSCORE).11
In our study, it is worthwhile to note that RApatients demonstratedagreatertendencyforobtainingahigher pre-dictionof10-yearriskofafatalcardiovasculardiseaseevent whenusingtheclassicalSCOREmatrix,andthatthe signif-icanceofthisdifferencewasestablishedwiththeuseofthe modifiedSCOREriskindex,withtheapplicationofa multiply-ingfactorof1.5tothesubgroup.Thisriskdifference,found inRApatients,isinaccordancewiththehigherprevalence ofcardiovasculareventsandofmortalityfromthiscause,a factalreadyconfirmedinseveralepidemiologicalstudies pre-viouslyconducted.
ThestudybyGómez-Vaqueroetal.,23with200RApatients,
aimedtoassessthe impactofEULARrecommendationson thecardiovascularriskapproach.Itsauthorsfoundthat11% ofpatientstowhomtheclassicalSCOREriskindexwasapplied and14%ofthoseassessedwiththemSCOREwereclassified asofhigh-risk(≥5%)for10-yearriskofafatalcardiovascular diseaseevent.
Data such as these emphasize the need to incorporate thosefactors inherenttothedisease tocardiovascularrisk stratificationtoolsinRApatients;thesefactorsperseincrease thecardiovascularmortalityrates.
Wecanconcludethat,accordingtotheEULAR recommen-dations,theapplicationofthemodifiedSCOREmatrixinRA patientsallowsustorecognize,inthispopulationatrisk,a subgroupofpatientswithahigher10-yearriskofafatal car-diovasculardiseaseeventinneedofanearlyandintensive pharmacologicalinterventionand ofthe useoftherapeutic targets to determine a lower risk of future cardiovascular events.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterests.
r
e
f
e
r
e
n
c
e
s
1.McInnesIB,ScheetG.Thepathogenesisofrheumatoid arthritis.NEnglJMed.2011;365:2205–19.
2.SanghaA.Epidemiologyofrheumaticdiseases. Rheumatology.2000;39Suppl.2:3–12.
3.GabrielSE,MichaudK.Epidemiologicalstudiesinincidence, prevalence,mortality,andcomorbidityoftherheumatic diseases.ArthritisResTher.2009;11:229.
4.Avi ˜na-ZubietaJA,ChoiHK,SadatsafaviM,EtminanM,Esdaile JM,LacailleD.Riskofcardiovascularmortalityinpatients withrheumatoidarthritis:ameta-analysisofobservational studies.ArthritisRheum.2008;59:1690–7.
5.Mäki-PetäjäKM,BoothAD,HallFC,WallaceSM,BrownJ, McEnieryCM,etal.Ezetimibeandsimvastatinreduce inflammation,diseaseactivity,andaorticstiffnessand improveendothelialfunctioninrheumatoidarthritis.JAm CollCardiol.2007;50:852–8.
6.HahnBH,GrossmanJ,ChenW,McMahonM.The
pathogenesisofatherosclerosisinautoimmunerheumatic diseases:rolesofinflammationanddyslipidemia.J Autoimmun.2007;28:69–75.
7.ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
8.VIDiretrizesBrasileirasdeHipertensão.ArqBrasCardiol. 2010;95:1–51.
9.ThirdReportoftheNationalCholesterolEducationProgram (NCEP)ExpertPanelonDetection,Evaluation,andTreatment ofHighBloodCholesterolinAdults(AdultTreatmentPanel III)finalreport.Circulation.2002;106:3143–421.
10.Standardsofmedicalcareindiabetes2011.DiabetesCare. 2011;34Suppl.1:S11–61.
11.PetersMJ,SymmonsDP,McCareyD,DijkmansBA,NicolaP, KvienTK,etal.EULARevidence-basedrecommendationsfor cardiovascularriskmanagementinpatientswithrheumatoid arthritisandotherformsofinflammatoryarthritis.Ann RheumDis.2010;69:325–31.
12.BoyerJF,GourraudPA,CantagrelA,DavignonJL,Constantin A.Traditionalcardiovascularriskfactorsinrheumatoid arthritis:ameta-analysis.JointBoneSpine.2011;78: 179–83.
13.SteinerG,UrowitzMB.Lipidprofilesinpatientswith rheumatoidarthritis:mechanismsandtheimpactof treatment.SeminArthritisRheum.2009;38:372–81. 14.TomsTE,PanoulasVF,KitasGD.Dyslipidaemiain
rheumatologicalautoimmunediseases.OpenCardiovascMed J.2011;5:64–75.
15.PetersMJ,vanHalmVP,VoskuylAE,SmuldersYM,BoersM, LemsWF,etal.Doesrheumatoidarthritisequaldiabetes mellitusasanindependentriskfactorforcardiovascular disease?Aprospectivestudy.ArthritisRheum.
2009;61:1571–9.
16.DesseinPH,JoffeBI.Insulinresistanceandimpairedbetacell functioninrheumatoidarthritis.ArthritisRheum.
2006;54:2765–75.
17.DoranM.Rheumatoidarthritisanddiabetesmellitus: evidenceforanassociation?JRheumatol.2007;34:460–2. 18.SolomonDH,LoveTJ,CanningC,SchneeweissS.Riskof
diabetesamongpatientswithrheumatoidarthritis,psoriatic arthritisandpsoriasis.AnnRheumDis.2010;69:2114–7. 19.KremersHM,CrowsonCS,TherneauTM,RogerVL,GabrielSE.
20.CrowsonCS,MattesonEL,RogerVL,TherneauTM,GabrielSE. Usefulnessofriskscorestoestimatetheriskof
cardiovasculardiseaseinpatientswithrheumatoidarthritis. AmJCardiol.2012;110:420–4.
21.ConroyRM,PyöräläK,FitzgeraldAP,SansS,MenottiA,De BackerG,etal.Estimationoften-yearriskoffatal cardiovasculardiseaseinEurope:theSCOREproject.Eur HeartJ.2003;24:987–1003.
22.RosalesAlexanderJL,MagroChecaC,SalvatierraJ,Cantero HinojosaJ,RayaAlvarezE.Cardiovascularriskassessmentin
rheumatoidarthritispatientsusingtheSCOREchart.Ann RheumDis.2012;71Suppl.3:660.
23.Gómez-VaqueroC,RobustilloM,NarváezJ,Rodríguez-Moreno J,González-JuanateyC,LlorcaJ,etal.Assessmentof