w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Food
intake
assessment
and
quality
of
life
in
women
with
fibromyalgia
夽
Emmanuelle
Dias
Batista
a,∗,
Aline
Andretta
a,
Renata
Costa
de
Miranda
b,
Jéssica
Nehring
c,
Eduardo
dos
Santos
Paiva
a,
Maria
Eliana
Madalozzo
Schieferdecker
baHospitaldeClínicas,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
bPost-GraduateProgramonFoodandNutritionSecurity,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
cUniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27August2014 Accepted2March2015
Availableonline11September2015
Keywords:
Fibromyalgia Qualityoflife Pain Foodintake Foodregistration
a
b
s
t
r
a
c
t
Objective:Tocomparethefoodintakeofwomenwithandwithoutfibromyalgiaandverify
ifthefoodintakeofpatientswithfibromyalgiainterfereswiththepainandqualityoflife.
Methods:Studyparticipantswerewomenwithfibromyalgia(FM)seeninFibromyalgia
Out-patientClinic,HospitaldasClínicas/UFPRandacontrolgroup(CT)withhealthywomen. DatacollectionwasconductedfromMarchtoOctober2012.Fortheassessmentoffood intakeweusedtheFoodRegistrationandtheanalyzeditemsweretotalcalories, carbohy-drates,proteins,lipids,vitamins(A,C,B12,DandE)andminerals(folate,selenium,zinc, iron,calciumandmagnesium).ThesoftwareusedwasAvanutriOnline®.Toevaluatethe qualityoflife,theFibromyalgiaImpactQuestionnaire(FIQ)andpainthresholdwereused.
Results:43patientswithFMand44healthywomenwereevaluated.CTgroupshoweda
meanconsumptionofnutrientsgreaterthanFMgroupexceptforiron.However,onlycaloric intake,carbohydrates,proteinsandlipidsingramsandpercentageoflipids,vitaminA,E, B12,folate,seleniumandcalciumwerestatisticallysignificant.InFMgroup,therewasa neg-ativecorrelationbetweenvitaminEandFIQandapositivecorrelationbetweenpercentage ofproteinandpainthreshold.
Conclusion: WomenwithFMshowedalowerqualitativeandquantitativeintakein
compar-isonwithCTgroup.OnlyvitaminEcorrelatedwithqualityoflifeandpercentageofprotein inthedietwithsensationofpain.
©2015ElsevierEditoraLtda.Allrightsreserved.
夽
StudyconductedatDepartmentofNutrition,EndocrinologyandRheumatology,UniversidadeFederaldoParaná(UFPR),Curitiba,PR, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](E.D.Batista). http://dx.doi.org/10.1016/j.rbre.2015.08.015
Avaliac¸ão
da
ingestão
alimentar
e
qualidade
de
vida
de
mulheres
com
fibromialgia
Palavras-chave:
Fibromialgia Qualidadedevida Dor
Ingestãoalimentar Registroalimentar
r
e
s
u
m
o
Objetivo:Compararaingestãoalimentardemulherescomesemfibromialgiaeverificarsea
ingestãoalimentardaspacientescomfibromialgiainterferenasensac¸ãodedorequalidade devida.
Métodos:Participaramdoestudomulherescomfibromialgia(FM)atendidasnoAmbulatório
deFibromialgiadoHospitaldeClínicas/UFPReparaogrupocontrole(CT)foramconvidadas mulheressaudáveis.Acoletadedadosfoifeitademarc¸oaoutubrode2012.Paraaavaliac¸ão doconsumoalimentarfoiusadooRegistroAlimentareositensanalisadosforam:calorias totais,carboidratos,proteínas,lipídeos,vitaminas(A,C,B12,DeE)eminerais(folato,selênio, zinco,cálcio,ferro emagnésio).OsoftwareusadofoioAvanutriOnline®.Paraavaliac¸ão daqualidadedevidafoiusadooQuestionáriodeImpactodaFibromialgia(FIQ)elimiar doloroso.
Resultados: Foramavaliadas43pacientescomFMe44 mulheressaudáveis.OgrupoCT
apresentouconsumomédiodenutrientessuperioraogrupoFM,comexcec¸ãoparaoferro. Entretanto,somenteaingestãocalórica,carboidratos,proteínaselipídeosemgramas, por-centagemdelipídios,vitaminaA,E,B12,folato,selênioecálcioforamestatisticamente significativas.NogrupoFMhouvecorrelac¸ãonegativaentrevitaminaEeFIQecorrelac¸ão positivaentreporcentagemdeproteínaelimiardoloroso.
Conclusão: AsmulherescomFMapresentaramingestãoqualitativamentee
quantitativa-menteinferioraogrupoCT.SomenteavitaminaEapresentoucorrelac¸ãocomaqualidade devidaeaporcentagemdeproteínanadietacomasensac¸ãodedor.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Fibromyalgia(FM)isoneofthemostfrequentrheumatic dis-eases.InBrazil,FMaffectsabout2–3%ofthepopulation, usu-allyappearbetween30and35yearsofageandismore com-monamongwomen.1,2Accordingtotheclassificationcriteria
oftheAmericanCollegeofRheumatology,thedefinitionofthis syndromeusestwovariables:Bilateralpainaboveandbelow thewaistplusaxialpainandawidespreadchronicpainover threemonths’duration,andpainonpalpationofatleast11 of18specificsitesinthebody,knownastenderpoints.3
Together with the pain, these patients often have a
decreaseintheirqualityoflifeduetosymptomssuchassleep disturbances,fatigue,morningstiffness,subjectivesenseof accumulationofbodyfluids,extremityparesthesias, depres-sion,headache,dizzinessandboweldisorders.1,2
Althoughitsetiologyandpathogenesisarenotknown,
evi-dence suggests that some individuals may have a genetic
predisposition to this disease when exposed to certain
environmental factors.Studies suggest involvement ofthe hypothalamus–pituitary–adrenalaxisandtheautonomic
ner-vous system in response to stress in patients showing
vulnerabilityforthisdisease,oritssymptoms.4–6
Theeatinghabitsofthesepatientsareimportant,the
rea-sonforwhichstudieshaveshownimprovementinsymptoms
ofthediseasewithabalancedandhealthydiet.7–10
VegetariandietsappeartoalleviatesomesymptomsofFM, andthismaybeduetotheirlowfatandproteincontent,high levelsoffiber,vitaminC,betacarotene,minerals(magnesium,
potassium,zinc,selenium) and antioxidants.8 Accordingto
the Brazilian Society ofRheumatology,care mustbe taken withnutritioninFMpatients,forinstance,reducingthe con-sumptionofsugar,salt,fatand alcoholand increasingthe intakeoffiber,fruits,vegetablesandfluidsinordertoavoid theappearanceofotherchronicdiseasesandofoverweight.9
Specificmicronutrientssuchascalcium(Ca)andmagnesium (Mg)areimportantinmusclecontractions,forhelpingto
pro-duce muscle spasms and nerve impulses.Evidence shows
thatincreasingintakeoffoodsourcesoftryptophancanbe beneficial,becausethisaminoacidplaysaroleinserotonin synthesis.10
Thestrategyforthetreatmentoffibromyalgiarequiresa multidisciplinaryapproach,withorwithoutpharmacological treatment.
The aimofthis study is tocompare the food intakeof womenwithandwithoutfibromyalgiaandverifyifthefood intakeoffibromyalgiapatientsinterfereswiththeirperception ofpainandwithqualityoflife.
Patients
and
methods
Thisisananalytical,cross-sectional,observationalstudy.The projectwasapprovedbytheHumanResearchEthics Commit-teeofHospitaldasClínicas,UniversidadeFederaldoParaná
(CEP-HC/UFPR). Female patients diagnosed with
the same age group were invited. All womenin the study signedanInformedConsentForm.Theexclusioncriteriain
the study were medication change in the last four weeks,
useofcorticosteroidsandvitaminsupplements,unbalanced hypothyroidism, being pregnant or breastfeeding, illiterate women,andfoodregistrationnotfilled.Datacollectiontook placebetweenMarchandOctober2012.
Fortheassessmentoffoodconsumption,aFoodRegistry wasused.Eachvolunteerwasinstructedtoregisterthree non-consecutivedaysofdieting(twoweekdaysandoneweekend day)andshouldincludedetailedfoodsorpreparations.Later the data were tabulated in the Avanutri Online® software andthemean3-dayintakewasadjustedtoreduce intraper-sonalandinterpersonalvariation.Theitemsexaminedwere total calories, carbohydrates, proteins, lipids, vitamins (A, C,B12,D andE)and minerals(folate, selenium,zinc,iron, calciumandmagnesium).Toassesstheadequacyof macronu-trients(carbohydrates,proteinsandlipids),AMDR(Acceptable MacronutrientDistributionRange)11 wasused asthe base;
forvitaminsandminerals,EAR(EstimatedAverage Require-ments)wasused.12,13
Toanalyze the subjects’ quality oflife,the participants completedtheFibromyalgiaImpactQuestionnaire(FIQ).14FIQ
assesses how muchthe disease interferes withday-to-day
activitiesthroughascorefrom 0to100.Thus,thecloserto 100,thegreatertheimpactofthediseaseonqualityoflife.
Tomeasurepainthreshold,theFisheralgometer,adevice thatdeterminestheintensityofpressureonaparticulararea, wasused.Inthisstudy,theareausedtochecktheintensityof painenduredbythesubjectwastherighttrapeziusmuscle. Themeasurementswereperformedintriplicatebythesame examiner.
Thenutritionalstatusofthestudyparticipantswas mea-suredusingtheBodyMassIndex(BMI),accordingtotheWorld HealthOrganization(WHO1998).15Tocalculatetheheight,we
usedaTonelli&Gomesstadiometer.Bodyweightwas mea-suredwiththeparticipantswearingtheminimumamountof clothesonaportabledigitalscalewithamaximumcapacity of150kg.
Forstatisticalanalysis,theMann–WhitneyUtestwasused todetectdifferencesbetweenmeansofnon-parametricdata,
and Spearman correlation was appliedfor non-parametric
data.Rsoftwareversion2.11.1(2010-5-31)Statgraphics Cen-turion and SPSSStatistics 17.0were usedinthe statistical analysis.Thelevelofsignificancewassetatp≤0.05.
Results
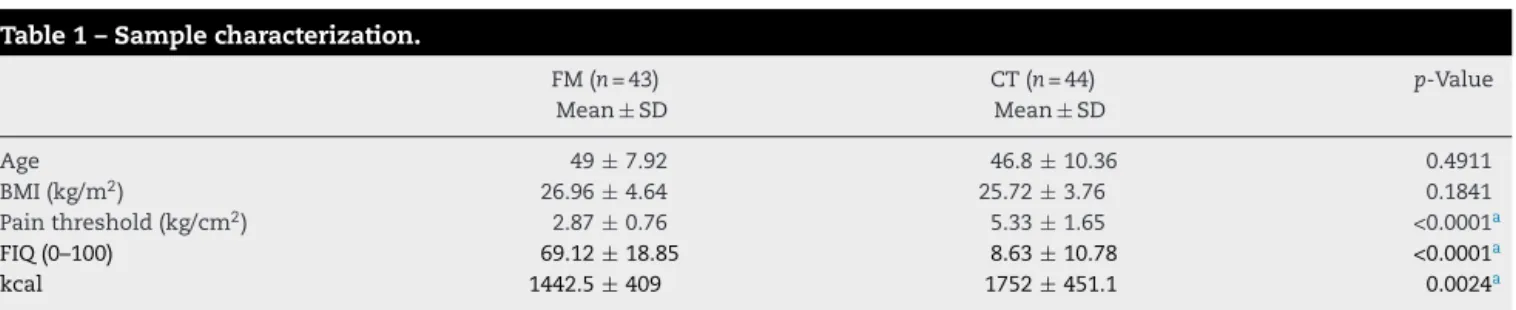
103womenwereevaluatedinthisstudy;ofthistotal,16were excludedforlackofdataontheirFoodRegister.Thefinal sam-pleconsistedof43patientswithfibromyalgiaand44controls. AgeandBMIweresimilarinbothgroups,whilepainthreshold, FIQandcalorieintakeweresignificantlydifferent(Table1).
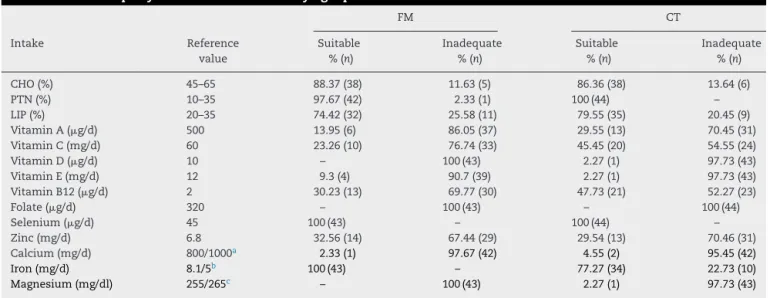
TheproperdistributionofmacronutrientsinthedietofFM patientswas88.37%(n=38)forcarbohydrates(CHO),97.67% (n=42)forproteins(PTN),and74.42%(n=32)forlipids(LIP). Ontheotherhand,incontrolgroup,86.36%(n=38)ofpatients exhibitedasuitabledistributionofCHO,100%(n=44)ofPTN, and79.55%(n=35)ofLIP.InFMgroup,inadequateintakeof micronutrientswaspresentinover65%ofpatients,exceptfor
consumptionofironandselenium,with100%ofadequacy.
InCTgroup,themicronutrientsthatshowedthehighest per-centageofadequacywereseleniumwith100%andironwith 77.27%.Folateintakewasinappropriatein100%andtheother micronutrientspresentedlowintakepercentagesofadequacy (Table2).
When CHO, PTN and LIP intake (in g) was compared
betweenFMversusCTgroup,astatisticaldifferencewasnoted.
However, whenthe percentage ofadequacy ofthesesame
nutrientswascompared,onlyLIPshoweddifference(Table3). Asformicronutrientintake,CTgroupshowedanadjusted meanintakehigherthanFMgroup,exceptforiron.Vitamin A,E,B12,folate,selenium,calciumandironintakesshoweda statisticallysignificantdifference(Table4).
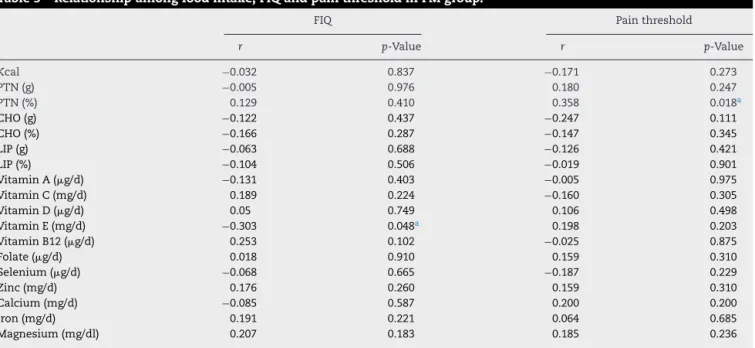
InthecorrelationsofFIQandpainthresholdversus
nutri-ent intake in FM group, it was observed that vitamin E
showed amoderateand negativecorrelationwithFIQ, and
%PTNpresentedamoderateandpositivecorrelationwithpain threshold(Table5).
Discussion
FMandCTgroupsshowednostatisticaldifferenceinthe vari-ablesageandBMI,revealinghomogeneity.Asexpected,FIQ andpainthresholdvaluesweredifferent,butthecontrolgroup foodintakewashigherwithrespecttocalories.
FMgrouphadaloweradjustedmeanintakeof macronutri-ents(ingrams),vitaminsandmineralsversusCTsubjects,with theexceptionofiron.However,vitaminA,E,B12,folate, sele-niumandcalciumintakeswerestatisticallysignificant.The
Table1–Samplecharacterization.
FM(n=43) Mean±SD
CT(n=44) Mean±SD
p-Value
Age 49±7.92 46.8±10.36 0.4911
BMI(kg/m2) 26.96±4.64 25.72±3.76 0.1841
Painthreshold(kg/cm2) 2.87±0.76 5.33±1.65 <0.0001a
FIQ(0–100) 69.12±18.85 8.63±10.78 <0.0001a
kcal 1442.5±409 1752±451.1 0.0024a
FM,fibromyalgiagroup;CT,controlgroup;SD,standarddeviation;BMI,BodyMassIndex;FIQ,FibromyalgiaImpactQuestionnaire;p-value,value oftheprobabilityassociatedwiththetestedstatistics.
Table2–Theadequacyoffoodintakeoffibromyalgiapatientsandcontrols.
FM CT
Intake Reference
value
Suitable %(n)
Inadequate %(n)
Suitable %(n)
Inadequate %(n)
CHO(%) 45–65 88.37(38) 11.63(5) 86.36(38) 13.64(6)
PTN(%) 10–35 97.67(42) 2.33(1) 100(44) –
LIP(%) 20–35 74.42(32) 25.58(11) 79.55(35) 20.45(9)
VitaminA(g/d) 500 13.95(6) 86.05(37) 29.55(13) 70.45(31)
VitaminC(mg/d) 60 23.26(10) 76.74(33) 45.45(20) 54.55(24)
VitaminD(g/d) 10 – 100(43) 2.27(1) 97.73(43)
VitaminE(mg/d) 12 9.3(4) 90.7(39) 2.27(1) 97.73(43)
VitaminB12(g/d) 2 30.23(13) 69.77(30) 47.73(21) 52.27(23)
Folate(g/d) 320 – 100(43) – 100(44)
Selenium(g/d) 45 100(43) – 100(44) –
Zinc(mg/d) 6.8 32.56(14) 67.44(29) 29.54(13) 70.46(31)
Calcium(mg/d) 800/1000a 2.33(1) 97.67(42) 4.55(2) 95.45(42)
Iron(mg/d) 8.1/5b 100(43) – 77.27(34) 22.73(10)
Magnesium(mg/dl) 255/265c – 100(43) 2.27(1) 97.73(43)
FM,fibromyalgiagroup;CT,controlgroup;%CHO,carbohydrateintakepercentage;PTN%,proteinintakepercentage;LIP%,lipidintake percent-age;n,numberofpatients.
a 19–50years:800mg/dand>51years:1000mg/d. b 19–50years:8.1mg/dand>51years:5mg/d. c 19–30years:255mg/dand>31years:265mg/d.
Table3–Macronutrientfoodintakeinfibromyalgiaandcontrolgroups.
AMDR FM(n=43)
Mean±SD
CT(n=44) Mean±SD
p-Value
Carbohydrates(g) – 191.79±62.05 226.48±65.06 0.0152a
Carbohydrates(%) 45–65 52.95±6.33 51.72±5.56 0.4474
Proteins(g) – 58.57±18.97 68.5±17.9 0.0102a
Proteins(%) 10–35 16.5±3.57 15.87±3.2 0.2136
Lipids(g) – 45.78±17.28 61.05±20.45 0.0007a
Lipids(%) 20–35 28.15±5.69 31.01±4.96 0.0214a
FM,fibromyalgiagroup;CT,controlgroup;SD,standarddeviation;AMDR,AcceptableMacronutrientDistributionRanges;p-value,valueofthe probabilityassociatedwiththetestedstatistics.
a Statisticallysignificantdifference(p<0.05)betweenFMandCTgroupswithMann–Whitneytest.
Table4–Micronutrientfoodintakeinfibromyalgiaandcontrolgroups.
EAR FM(n=43)
Mean±SD
CT(n=44) Mean±SD
p-Value
VitaminA(g/d) 500 302.7±231.29 446.14±274.03 0.0021a
VitaminC(mg/d) 60 49.47±29.27 66.9±51.73 0.2571
VitaminD(g/d) 10 1.78±1.65 2.04±1.98 0.4348
VitaminE(mg/d) 12 6.58±3.83 10.29±0.87 <0.0001a
VitaminB12(g/d) 2 1.96±2.2 2.4±1.85 0.0359a
Folate(g/d) 320 83.29±55.27 101.27±0.05 0.0015a
Selenium(g/d) 45 48.46±0.07 51.97±0.09 <0.0001a
Zinc(mg/d) 6.8 5.67±2.59 5.75±2.36 0.8221
Calcium(mg/d) 800/1000b 404.13±235.53 510.87±210.2 0.0428a
Iron(mg/d) 8.1/5c 11.64±0.23 9.52±3.78 <0.0001a
Magnesium(mg/dl) 255/265d 135.84±58.87 149.86±49.9 0.1712
FM,fibromyalgiagroup;CT,controlgroup;SD,standarddeviation;EAR,EstimatedAverageRequirement;p-value,valueoftheprobability associatedwiththetestedstatistics.
a Statisticallysignificantdifference(p<0.05)betweenFMandCTgroupswithMann–Whitneytest. b 19–50years:800mg/dand>51years:1000mg/d.
Table5–Relationshipamongfoodintake,FIQandpainthresholdinFMgroup.
FIQ Painthreshold
r p-Value r p-Value
Kcal −0.032 0.837 −0.171 0.273
PTN(g) −0.005 0.976 0.180 0.247
PTN(%) 0.129 0.410 0.358 0.018a
CHO(g) −0.122 0.437 −0.247 0.111
CHO(%) −0.166 0.287 −0.147 0.345
LIP(g) −0.063 0.688 −0.126 0.421
LIP(%) −0.104 0.506 −0.019 0.901
VitaminA(g/d) −0.131 0.403 −0.005 0.975
VitaminC(mg/d) 0.189 0.224 −0.160 0.305
VitaminD(g/d) 0.05 0.749 0.106 0.498
VitaminE(mg/d) −0.303 0.048a 0.198 0.203
VitaminB12(g/d) 0.253 0.102 −0.025 0.875
Folate(g/d) 0.018 0.910 0.159 0.310
Selenium(g/d) −0.068 0.665 −0.187 0.229
Zinc(mg/d) 0.176 0.260 0.159 0.310
Calcium(mg/d) −0.085 0.587 0.200 0.200
Iron(mg/d) 0.191 0.221 0.064 0.685
Magnesium(mg/dl) 0.207 0.183 0.185 0.236
FIQ,FibromyalgiaImpactQuestionnaire;PT,painthreshold;r,correlationcoefficient;p-value,valueoftheprobabilityassociatedwiththetested statistics.
a Statisticallysignificantdifference(p<0.05),withSpearmancorrelation.
resultsindicatethatFMpatientspresentedqualitativelyand quantitativelylowerintakesversusCTsubjects.
Thecombinationoftheantioxidantsfoundinvitaminsand mineralswithanalgesicagentscanreducethedosesofthese drugsandconsequentlyimprovethesensationofpainofFM patients.Itwasalsodemonstratedthatantioxidantsare criti-calinreducingtheoxidativestressinducedbyFM.16Basedon
thisstudy,itwasnotedthatapropernutritionalguidancefor thesepatientscandecreasethesymptomsofthedisease.
Inmost ofthe FM subjects, aninadequate ingestion of vitaminCwasobserved.Richardetal.16showedthatthe
pro-longeduseofanalgesicscanincreasetheexcretionofvitamin Candpotassium,causing,asaresult,irondeficiencyanemia. WomenwithFMexhibitedanadequateintakeofiron,andthe presenceofanemiawasnotassessedinthisstudy. Maintain-ingahealthyandbalanceddietwithvitaminsandmineralsis importanttominimizefuturedeficiencyintheirbloodlevels. WhenpainthresholdandFIQwererelatedtofoodintake
ofFMpatients,vitaminEshowedamoderateand negative
correlationwithFIQ,indicatingthatthehighertheintakeof thisvitamin,thebetterwouldbethequalityoflife.Studies showthatantioxidant-richdietsimprovethesymptomsofFM bypromotingvasodilation.Katzetal.17explainthatthepain
inFMmightoccurduetovasomotordysregulation,whichin turncausesmusclehypoperfusion.
InthestudybySakaryaetal.,18theauthorsevaluatedblood
levelsofantioxidantvitaminsandmagnesiumandcorrelated withclinical parametersofFM. Theauthors foundno cor-relationbetweenvitaminsA,C,EandMglevels,numberof tenderpoints,painseverity,functionalabilityanddepression inpatientswithFM.Theresultssuggestthatpoorintakeof thesenutrientsdonotnecessarilysignifylowbloodlevels.
%PTNinthenutritionofFMwomenhadamoderateand
positive correlation with pain threshold, showing that the
higher the proteinpercentage,the greater the toleranceto pain.PatientswithFMshowedPTNintakewithinAMDR rec-ommendations,andarguablyifthispercentagewereoutside normalrange,theresultwould notbethesame.Thestudy byShiavonandPortero19 evaluatedproteinorigin,
conclud-ing that the lower consumptionofanimal proteinand the
higherconsumptionofvegetableprotein,associatedwiththe
consumption of fruits, vegetables and legumes, provide a
healthierstatetobodytissues.Butourstudydidnotassessthe ingestedPTNquality;thus,itwasnotpossibletocheckifthe intakeofPTNofdifferentoriginswouldinterferedifferently inpainthreshold.
A relationship between food intake and pain was also
foundinthestudybyBelletal.20;theseauthorsfoundthat
folateandvitaminB12areessentialforregulationofcentral nervoussystem,andthattheirdeficiencyresultsin periph-eralneuropathypain.WhilevitaminCdeficiencycancause myalgiaandbonepain,vitaminDdeficiencycancause mus-culoskeletalpain.
Althoughtherelationshipoftheotherstudiednutrientsin improvingthequalityoflifeandpainsensitivityhasalready beenestablished,inourstudy,wecould notverifyany sta-tisticalcorrelation,possiblyduetothesmallsamplesizeor becauseofahighlyinadequateintakeofseveral micronutri-ents.
FM isa chronicdisease that manifestsitself differently frompersontoperson,affectingthequalityoflifeofpatients
thankstophysicalandpsychologicalsymptoms.The
phar-macologicaltreatmentaloneisinadequateformostpatients; thus,multidisciplinary approaches havebeen usedin clin-ical practice. Studies have shown that the combination of
moderate physical activity and supplementation/intake of
antioxidants may be beneficial, because this combination
Conclusion
WomenwithFMexhibitedaqualitativelyandquantitatively
lower intakeversus CTsubjects. Vitamin Eshowed a
mod-erateandnegativecorrelationwithqualityoflifeand with percentageofproteininthediet,andamoderateand posi-tivecorrelationwithpainthreshold.Theseresultsshowthe
importance of a proper and healthy nutrition to improve
FM symptoms. More studies are needed to determine the
potentialassociationbetweenclinicalparametersofFMand macronutrientandmicronutrientintake.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. HeymannRE,PaivaES,HelfensteinMJ,PollakDF,MartinezJE, ProvenzaJR,etal.Consensobrasileirodotratamentoda fibromialgia.RevBrasReumatol.2010;50:56–66.
2. SociedadeBrasileiradeReumatologia–SBR.Fibromialgia. SBR;2004[ProjetoDiretrizes].
3. WolfeF,SmytheHA,YunusMB,BennettRM,BombardierC, GoldenbergDL,etal.TheAmericanCollegeofRheumatology 1990criteriafortheclassificationoffibromyalgia:reportof theMulticenterCriteriaCommittee.ArthritisRheum. 1990;33:160–72.
4. PillemerSR,BradleyLA,CroffordLJ,MoldofskyH,Chrousos GP.Theneuroscienceandendocrinologyoffibromyalgia. ArthritisRheum.1997;40:1928–39.
5. DadabhoyD,CroffordLL,SpaethM,RussellIJ,ClauwDJ. Biologyandtherapyoffibromyalgia:evidence-based biomarkersforfibromyalgiasyndrome.ArthritisResTher. 2008;10:211.
6. BuskilaD,Sarzi-PuttiniP.Biologyandtherapyoffibromyalgia: geneticsaspectsoffibromyalgiasyndrome.ArthritisRes Ther.2006;8:218–22.
7. SienaLS,MarroneL.Ainfluênciadaalimentac¸ãonareduc¸ão ounoagravamentodossintomasapresentadosempacientes portadoresdefibromialgia.RevistaSaúdeePesquisa. 2010;3(3):339–43.
8. DonaldsonMS,SpeightN,LoomisS.Fibromyalgiasyndrome improvedusingamostlyrawvegetariandiet:an
observationalstudy.BMCComplementAlternMed.2001;1:7.
9.SociedadeBrasileiradeReumatologia–SBR.Dieta;2013. Availableat:http://www.fibromialgia.com.br/novosite/index. php?modulo=pacientesartigos&idmatmat=11&idmat=10 [accessed25.09.13].
10.SierraC,MargaritMIB.AlimentaciónemFibromialgia. Barcelona:AFIBROM;2007.
11.Dietaryreferenceintakesforenergy,carbohydrate,fiber,fat, fattyacids,cholesterol,protein,andaminoacids;2002/2005. http://www.nap.edu/[accessed17.09.13].
12.InstituteofMedicine(IOM),FoodandNutritionBoard.Dietary referenceintakes(DRI)forvitaminC,vitaminE,seleniumand carotenoids.Washington:NationalAcademyPress;2000. 13.InstituteofMedicine(IOM),FoodandNutritionBoard.Dietary
referenceintakes(DRI)forvitaminA,vitaminK,arsenic, boron,chromium,cooper,iodine,iron,manganese, molybdenum,nickel,silicon,vanadiumandzinc. Washington:NationalAcademyPress;2000.
14.MarquesAP.Validac¸ãodaversãobrasileiradoFibromyalgia ImpactQuestionnaire(FIQ).RevistaBrasileirade
Reumatologia.2006;46(1):24–31.
15.WHO(WorldHealthOrganization).Obesity:preventingand managingtheglobalepidemic.ReportofaWHOconsultation onobesity.Geneva:WHO;1998.
16.RichardR,VáclavH,PekárkováI,KrejcováJ,RacekJ,Ladislav TL,etal.Freeradicalsafterpainfulstimulationareinfluenced byantioxidantsandanalgesics.NeuroendocrinolLett. 2003;24(5):304–9.
17.KatzDL,GreeneL,AliA,FaridiZ.Thepainoffibromyalgia syndromeisduetomusclehypoperfusioninducedby regionalvasomotordysregulation.MedHypotheses. 2007;69:517–25.
18.SakaryaST,AkyolY,BedirA,CanturkF.Therelationship betweenserumantioxidantvitamins,magnesiumlevels,and clinicalparametersinpatientswithprimaryfibromyalgia syndrome.ClinRheumatol.2011;30:1039–43.
19.ShiavonAV,PorteroKCC.Aspectosfisiopatológicose nutricionaisdafibromialgia.RevistaNutric¸ãoemPauta. 2004;12(64):35–40.
20.BellRF,BorzanBJ,KalsoCE,SimonnetG.Food,pain,and drugs:doesitmatterwhatpainpatientseat?Pain. 2012;153(10):1993–6.
21.MustafaN,SelamiA,FerayS,KadirY,OmerC,SevilayE,etal. VitaminsCandEtreatmentcombinedwithexercise
modulatesoxidativestressmarkersinbloodofpatientswith fibromyalgia:acontrolledclinicalpilotstudy.InfHealthc USA.2010;13(6):498–505.