REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
CASE
REPORT
Severe
protein-calorie
malnutrition
in
two
brothers
due
to
abuse
by
starvation
Marcela
Montenegro
Braga
Barroso
∗,
Luiza
Martins
Salvador,
Ulysses
Fagundes
Neto
UniversidadeFederaldeSãoPaulo(Unifesp),SãoPaulo,SP,Brazil
Received11January2016;accepted20May2016 Availableonline23August2016
KEYWORDS
Protein-energy malnutrition; Childabuse; Nutritional deficiencies
Abstract
Objective: Todescribethecaseoftwosiblingswithsevereprotein-caloriemalnutritiondueto abusebystarvation.
Casesdescription: Thetwopatientsweresimultaneously referredtotheHospitalMunicipal, wheretheywereadmittedtothePediatricGastroenterologyclinicofauniversityhospitalfor diagnosticinvestigationofthecauseofseveremalnutritionandscreeningtestsforCeliac Dis-ease,CysticFibrosisandEnvironmentalenteropathyamongothers.Theexamswereallnormal, andafterdetailedresearchontheinteractionsofthisfamily,wereachedtheconclusionthatthe malnutritionwasduetoabusebystarvation.Thechildrenspentapproximatelytwomonthsin thehospital,receivingahigh-proteinandhigh-caloriediet,withsignificantnutritionalrecovery.
Comments: Abusebystarvation,althoughrare,shouldalwaysbeconsideredofasoneofthe causesofchildmalnutritionandpediatricianshouldbeawareofthechild’sdevelopment,as wellasthefamilyinteractions,topreventmoreseverenutritionalandemotionalconsequences inthefuture.
©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Desnutric¸ão proteico-calórica; Maus-tratosinfantis; Deficiências
nutricionais
Desnutric¸ãoproteico-calóricagraveemdoisirmãosdevidoaoabusoporprivac¸ão alimentar
Resumo
Objetivo: Descreveroscasosdedoisirmãosacometidosdedesnutric¸ãoprumoteico-calórica gravecausadaporabusoporprivac¸ãoalimentar.
Descric¸ãodoscaso: Osdoispacientesvieramsimultaneamenteencaminhadosdeumhospital municipal, ondeestavam internados, ao Ambulatóriode Gastrenterologia Pediátrica de um
∗Correspondingauthor.
E-mail:[email protected](M.M.Barroso).
http://dx.doi.org/10.1016/j.rppede.2016.06.002
2359-3482/©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY
hospitaluniversitárioparainvestigac¸ãodiagnósticadacausadedesnutric¸ãograve.Foramfeitos examesparapesquisadedoenc¸acelíaca,fibrosecísticaeenteropatiaambiental,entreoutras. Osexamesmostraram-setodosnormaise,apósinvestigac¸ãodetalhadasobreorelacionamento dessa família, chegou-se à conclusão de que a desnutric¸ão tinha como causa o abuso por privac¸ãoalimentar.Ascrianc¸aspassaramcercade2mesesinternadas,receberamumadieta hiperproteicaehipercalórica,comrecuperac¸ãonutricionalsignificativa.
Comentários: Oabusoporprivac¸ãoalimentar,emborararo,deve sempreserpensadocomo umadascausasdedesnutric¸ãoinfantil,devendoopediatraestaratentoaodesenvolvimento dacrianc¸a,bemcomoaoseurelacionamentofamiliar,paraevitarconsequênciasnutricionais eemocionaismaisgravesnofuturo.
©2016SociedadedePediatriadeS˜aoPaulo. PublicadoporElsevier EditoraLtda.Este ´eum artigoOpenAccesssobumalicenc¸aCCBY(http://creativecommons.org/licenses/by/4.0/).
Introduction
Protein-caloriemalnutritioninchildhoodisaworldwide pub-lichealthproblem,especiallyincountriesoflowandmiddle income,beingrelatedtomorethanonethirdofalldeaths ofinfantsandchildrenunderfiveyearsinthesecountries.1
TheUnitedNationsChildren’sFund(UNICEF)recognizes environmental,economicandsocio-politicalfactorsasroot andunderlyingcausesofmalnutrition,withpoverty repre-sentingthecoreoftheproblem.2
Anotherlesscommon,butextremelyseriouscause con-cerns abuse by starvation, when parents or caregivers deliberatelyfail tofeed theirchildren, whichcan leadto riskofdeath.3
The aim of this study is to describe the cases of two siblings suffering fromsevere protein-energy malnutrition duetoabuseby starvation,which characterizesatypeof mistreatment.
Case
description
The two patients were simultaneously referred from the Hospital Municipal de Diadema (HMD), where they were admittedtothePediatricGastroenterologyClinicofEscola Paulista de Medicina for diagnostic investigation of the severeprotein-caloriemalnutritioncauses.
The motherreportedthatheryoungerson,4yearsand 8months,wasfeelingfineathome,whensuddenlyhewent into ‘‘respiratory arrest’’ (sic); so she called the Mobile Emergency Service (SAMU)and there wasneed for resus-citationmaneuvers(sic).Afterthat,thepatientwastaken toHMD,whereitwasdecidedtoadmithim,togetherwith hisolderbrother,duetoapictureofseveremalnutrition.
Sincethen, childrenstarted beingfollowedat our out-patientclinicevery15daysfordiagnosticinvestigationand clinicalfollow-up.
Case1
Male patient, aged 6 years and 11 months, with good weight/heightgainuptoapproximately2yearsold.After thattime,therewasan evidentweightgaindeceleration, whichapparentlyoccurredwithoutanydefinitecause.Itwas alsoobservedthatbetween2and4yearsofagetherewas
norecordofweightandheight,becausethepatientstopped attendingtheBasicHealthUnit(BHU).
After4yearsofage,thesemeasureswereagainrecorded inthevaccinationcard, whichshowedevidentweightand growthimpairment.
According to the mother’s report, the patient had an adequatediet(evaluatedbyanutritionteam).Shedenied the occurrence of diarrhea, constipation, abdominalpain and/ordistensionoranyothergastrointestinalsymptoms.
Regardingthe familyhistory, thepatienthasa brother aged4yearsand8monthswithasimilarpicture.Thefather ishealthy andthe motherwasfollowed at the Psychiatry Service,usedmedications,buthadnodefinitivediagnosis. Atthefirstvisit,themothersaidhernamewasMariadas Grac¸as;however,insubsequentconsultations,we realized thattheir children called herAna Paula. The mother was investigatedonsuspicionofmistreatmentandaccompanied thechildrenduringhospitalizationatHMD.
The familylived in ahousewithbasic sanitation, with runningwater and sewagesystems. Familyincome varied from1to5minimumwages.
On physical examination,thepatient showedaregular general status, extremely emaciated, pale (+/4+), apa-thetic,withscarcesubcutaneoustissue,muscleatrophyof theglutealregionandabdominaldistension.Weight=8.5kg (W/A Z-score=−6.56) and height=87cm (height/age Z
-score=−6.21).
The patient had the following laboratory tests: hemoglobin 9.4g/dL; hematocrit 28.9%; leukocytes 2680; platelets148,000;serumglutamicoxaloacetictransaminase (SGOT) 1.191U/L; serum glutamic pyruvic transaminase (SGPT) 1.043U/L. These changes were attributed to a pictureofsevereprotein-caloriemalnutrition.
Atthefirstconsultation,thediagnosisofsevere protein-calorie malnutrition was characterized and the patient startedbeinginvestigatedforthe followingcauses: celiac disease,cysticfibrosis ofthe pancreasandenvironmental enteropathy,amongothers.
The following laboratory tests were requested: anti-transglutaminaseantibody,sweattest(sodiumandchloride insweat)andupperendoscopywithduodenalbiopsy. Labo-ratorytestswerenegativeforthesuspecteddiagnosesand duodenalbiopsydisclosedfingerlikevilliandceliacdisease wasruledout(Fig.1).
Figure1 Duodenalbiopsyspecimens(case1):meanincrease (10×) showing fingerlike villi, preserved crypts, villus:crypt
ratio4:1.
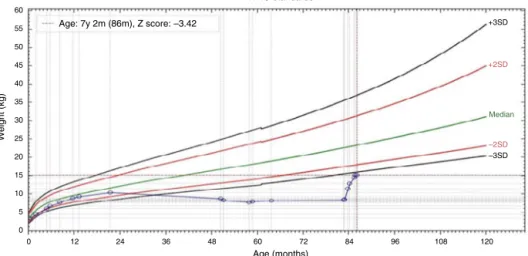
andhigh-proteindiet.The patientshowedexcellent nutri-tionalrecovery (Fig.2) and considerable improvement in moodandphysicalactivity,withthedisappearanceofthe initialapathy(Fig.3).
Theexcellentclinicaloutcometriggeredexclusivelybya high-calorieandhigh-proteindietreinforcedthediagnostic suspicionofmistreatment,withsubsequentprogressionto severeprotein-caloriemalnutritionbystarvation.Thechild waslegallyremovedfromtheirparentsandis,togetherwith hisbrother,inashelter.
Case2
Malepatient,aged4yearsand8months,bornandresiding inthemunicipalityofDiadema,wasreferredtoourservice fromHMD,wherehewashospitalized.
The motherreportedthattheBHUpediatrician started torealizethatthepatientdidnotgainweightafter3years ofage.Shedeniedabdominaldistensionanddiarrhea.She reportedthatthepatientateadequatelyand,accordingto thenutritionteamassessment,itwasnotpossibletoidentify anyprotein-calorierestrictioninrelationtoage.
On physical examination, the child showed regu-lar general status, was very emaciated, weight=7.585kg (weight/ageZ-score=−5.73) andheight=80cm (height/age
Z-score=−6.35).
Atthefirstconsultation,thediagnosisofsevere protein-calorie malnutrition wasmade andthe patientstarted to beinvestigatedfor the samecauses ofmalabsorptive dis-easesthat hisbrotherwasundergoing,withnegativetest results. The duodenal biopsy disclosed fingerlike villi and celiacdiseasewasruledout(Fig.4).
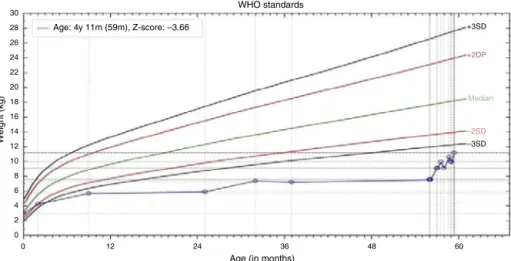
ThepatientremainedhospitalizedfortwomonthsatHMD withhisbrother, receivingahigh calorie andhigh-protein diet,showingexcellentnutritionalrecovery(Figs.5and6), whichreinforcedthediagnosticsuspicionofabuse.
During one of the visits to our clinic, when the chil-drenwerealreadylivingintheshelter,weaskedthesocial workeraboutthefactthathermothersometimessaidher namewasMariadasGrac¸asand,sometimes,AnaPaula.The social worker informedusthat up untilthe older brother wasaged2andahalfyears,thechildrenandtheirparents livedneartherestoftherelatives;however,theymovedto anunknowndestinationandlostcontactwiththefamily.In thisnewhome,thepatient’smothertoldtheneighborsher namewasAnaPaula.
Regardingthechildren’sfather, hesaidthatheworked all day and did not realize that the mother did not feed childrenadequately.Hewasconsideredanaccompliceand thechildrenwerekeptawayfromhim.
Discussion
Malnutrition causedbyfamilyneglect,which is character-izedbyanon-deliberatefailuretomeetthechild’sneeds, can occur due toignorance, low socioeconomic status or evendietarybeliefs.3,4
Ontheotherhand,abusebystarvation,thecauseof mal-nutritioninourtwopatients,differsfromneglectbythefact thatitischaracterizedasdeliberateormaliciousfailureto meetthechild’sneeds.3
Nancyetal.,4in2005, described12malnourished
chil-drenvictimsofabusebystarvationinTexas,USA.Similarly tothepatientsinourstudy,thechildrenwereinvestigated
WHO standards
Age: 7y 2m (86m), Z score: –3.42
60
55
50
+3SD
+2SD
–2SD
–3SD Median 45
40
35
30
Weight (kg) 25
20
15
10
5
0
0 12 24 36 48 60
Age (months)
120 108 96 84 72
Figure3 Patient1atthefirstconsultationand2monthslater.
Figure 4 Duodenal biopsy specimen (case 2): high mag-nification (100×), fingerlike villi, cylindrical epithelium with
nucleus inbasal position,preserved basal membrane, goblet cellspresentalongthevilli,mildlymphoplasmacyticinfiltrate inthelaminapropria.
fororganicdiseases,whichwereruledout.Thesechildren had,regardingtheirhistory,somepointsincommontothat ofourtwopatients,namely: (1)themotherreportedthat tookthechildrentothepediatricianwithsomefrequency, althoughtherewasnorecent recordof medical consulta-tions; (2) the motherof one of the children went tothe healthservicebecausethechild‘‘wasnotbreathing’’,asin thecaseofouryoungerpatient;(3)thechildrenwerealso excludedfromsociallife,andinourcases,hadnocontact withtherestofthefamilyforabouttwoyears.
Regardingthefathers’role,Krieger,5in1974,published
10cases ofchildren subjected tofooddeprivation bythe mothers,inwhichthehusbandsclaimedtheydidnotknow thatthechildren weresubjected tothissituation asthey spentthedayat workanddidnotrealizeit, exactlyasit happenedwiththefatherofthechildreninourstudy.
Inthenationalliterature,althoughtherearemany arti-clesaboutchildabuse,therearefewreportsonmalnutrition causedbyabuseduetostarvation.NudelmannandHalpern,6
30 28 26 24 22 20 18 16 14
Weight (kg)
Age: 4y 11m (59m), Z-score: –3.66
WHO standards
+3SD
+2DP
–2SD
–3SD Median
Age (in months) 12
10 8 6 4 2 0
0 12 24 36 48 60
Figure5 Weight/ageratiochartdemonstratingthenutritionalrecoveryincase2.
Figure6 Patient2atthefirstconsultationand2monthslater.
thesemothershadhigherrates ofdepression,aswellasa higherprevalenceofabuseduringchildhoodandconcluded thatmalnutritionhadamultifactorialorigin.
A differential diagnosis that also deserves to be dis-cussedisMunchausensyndromebyproxy,correspondingto aformofchildabusecausedbyaperpetratorwitha psychi-atricdisorderthatexacerbates,falsifiesorpromotesclinical
histories, laboratoryevidence, cancause physical injuries andinducehospitalizationsforunnecessarytherapeuticand diagnosticprocedures.7
A noteworthy aspect concerns the morphological find-ings in the small intestine at optical microscopy in both patients, considering that the absence of severe injuries couldconstituteanapparentparadox.However,the descrip-tion of morphological alterations of the small intestine mucosainmostcasesofsevereprotein-caloriemalnutrition is accompanied by environmental enteropathy.8,9 In such
circumstances,aspreviouslydemonstrated,atleast approx-imately 65% of individuals, even without a complaint of diarrhea,wouldhaveanovergrowthofcolonicflorainthe smallintestine lumen.10 It is known thatthe colonization
of the small intestine by colonic flora causes malabsorp-tion of dietary nutrients and severe injuries to the small intestinemucosa, duetothe7 alpha-dehydroxylationand deconjugation of primarybile salts, which are converted intosecondarybilesaltsanddeconjugated,beingvery harm-fultothejejunalmucosa.11However,thiswasnotthecase
of our patients, as it was adequately established by the social workers that they lived in a brick house that had waterandsewagetreatmentand,therefore,therewereno environmentalcontaminationconditionsthatcouldleadto bacterial overgrowth. Moreover,after all relevant labora-toryresearch,itwasdefinitelycharacterizedthatthesevere protein-caloriemalnutritionwasexclusivelydueto deliber-atestarvation.Experimentalstudies withratswithsevere protein-caloriemalnutritionintheabsenceoftriggering fac-torsofbacterialovergrowthshowedthatthemorphologyof thesmallintestinedidnotsufferanyalterationsandthevilli werefullypreserved.
Our patients, in spite of the severe protein-calorie malnutrition by starvation, had intestinal villi perfectly compatible withnormality; the inflammatory infiltrate of thelamina propriawasdiscreetand thevillus/cryptratio was 4/1. Interestingly, our patients, as observed in the experimental study of malnourished rats regarding the increased absorptive function, when given a high-protein and high calorie diet, showed rapid nutritional recovery within a short period of time, which proves that their digestive-absorptivefunctionswerekeptintactdespitethe prolongedperiodoffooddeprivation.Thesefindings demon-strate for the first time in humans, to the best of our knowledge,thatsevere protein-caloriemalnutritionis not primarily the cause of severe disorders of the digestive-absorptivefunction: theoccurrenceof anexternal factor, suchas the environmentalcontamination, is necessary to triggerallthepathophysiologicalandsymptomaticprocess describedinenvironmentalenteropathy.
Regardingtheprevalenceofbacterialovergrowth associ-atedwithenvironmentalenteropathyinBrazil,somestudies have beencarriedout withthe lactulosehydrogen breath test.Astudyinvolving83schoolchildrenlivingintherural, urban areas and a slum in a municipality in the country-sideofSãoPaulodisclosedbacterialovergrowthin7.2%of theassessedchildren.12Inthisstudy,theproportionof
bac-terial overgrowth in children living in a slum(18.2%) was statisticallyhigherthanthatofchildrenwhodidnotlivein aslum.
Protein-calorie malnutrition can be caused by organic diseases,poorsocialcondition,neglectandabuseby star-vation. The latter cause is rare, withfew reports in the literature,butithassevereconsequences,bothnutritional andpsychological,for theaffectedchild.The pediatrician playsa keyroleinthe earlydetectionof thesecasesand shouldalwaysbealerttomonitorthechild’sweight/height development,aswellasthefamilyrelationships.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.OwoajeE,OnifadeO,DesmennuA.Familyandsocioeconomic risk factors for undernutritionamong children aged 6 to 23 MonthsinIbadan,Nigeria.PanAfrMedJ.2014;17:161.
2.Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, EzzatiM,etal.Maternalandchildundernutrition:globaland regionalexposuresandhealthconsequences.Lancet.2008;371: 243---60.
3.GoldenMH,SamuelsMP,SouthallDP.Howtodistinguishbetween neglect and deprivational abuse. Arch Dis Child. 2003;88: 105---7.
4.KelloggND,LukefahrJL.Criminallyprosecutedcasesofchild starvation.Pediatrics.2005;116:1309---16.
5.Krieger I. Food restriction as a form of child abuse in tencases ofpsychosocialdeprivationDwarfism. ClinPediatr. 1974;13:127---34.
6.NudelmannC,HalpernR.Opapeldoseventosdevidaemmães de crianc¸as desnutridas: o outrolado da desnutric¸ão. Cienc SaúdeColetiva.2011;16:1993---9.
7.Pires JM, Molle LD. Síndrome de Munchausen por procurac¸ão---Relato de dois casos. J Pediatr (Rio J). 1999;75:281---6.
8.FagundesNetoU,MoraisMB,MachadoNL.Enteropatia ambi-ental em crianc¸as moradoras na periferiada cidade de São Paulo.Capacidadedaabsorc¸ãodaD-xilose.JPediatr(RioJ). 1984;57:33---6.
9.Fagundes-Neto U, Viaro T, Wehba J, Patrício FR, Machado NL.Tropicalenteropathy(environmentalenteropathy)inearly childhood:asyndromecausedbycontaminatedenvironment.J TropPediatr.1984;30:204---9.
10.FagundesNetoU,MartinsMC,LindosoF,PatricioFR. Asymp-tomatic environmental enteropathy among slum-dwelling infants.JAmCollNutr.1994;13:51---6.
11.FagundesNetoU,TeichbergS,BayneMA,MortonB,LifshitzF. Bilesalt-enhancedratjejunalabsorptionofamacromolecular tracer.LabInvest.1981;44:18---26.