w w w . r b o . o r g . b r
Original
Article
Comparative
radiographic
analysis
on
the
anatomical
axis
in
knee
osteoarthritis
cases:
inter
and
intraobserver
evaluation
夽
Luiz
Felipe
Matos
a,
Marcos
Giordano
b,
Gustavo
Novaes
Cardoso
b,
Rafael
Baptista
Farias
b,
Rodrigo
Pires
e
Albuquerque
c,∗aHospitalFederaldoAndaraí,RiodeJaneiro,RJ,Brazil
bHospitaldaForc¸aAéreadoGaleão,RiodeJaneiro,RJ,Brazil
cKneeSurgeryService,InstitutoNacionaldeTraumatologiaeOrtopedia(INTO),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12May2014 Accepted1July2014 Availableonline28May2015
Keywords:
Osteoarthritis/radiography Knee
Lowerextremity
a
b
s
t
r
a
c
t
Objective:Tomakeacomparativeinterandintraobserveranalysisonmeasurementsofthe anatomicalaxisbetweenpanoramicradiographsofthelowerlimbsinanteroposterior(AP) viewwithbipedalweight-bearing,onshortfilm.
Methods:Anaccuracystudycomparingradiographicmeasurementson47kneesofpatients attendingthekneesurgeryoutpatientclinicduetoosteoarthritis.Theradiographic evalua-tionusedwasasstandardizedforthetotalkneearthroplastyprogram,includingpanoramic APviewsofthelowerlimbsandshortradiographsofthekneesinAPandlateralviews,all withbipedalweight-bearing.Followingthis,theanatomicalaxisofthelowerlimbsorthe femorotibialanglewasmeasuredbyfiveindependentexaminersonthepanoramicand shortAPradiographs;threeoftheexaminerswereconsideredtobemoreexperiencedand two,lessexperienced.Allthemeasurementsweremadeagainbythesameexaminersafter anintervalofnotlessthan15days.Thestatisticalanalysiswasperformedusingthe intr-aclasscorrelationcoefficient,inordertoevaluatetheinterandintraobserverconcordance oftheanatomicalaxismeasurements.
Results:Fromthestatisticalanalysis,itwasobservedthattherewasstronglysignificant concordance betweenthe anatomicalaxis measurements onthe panoramic andshort radiographs,forallthefiveexaminersandforbothmeasurements.
Conclusions: Undertheconditionsstudied,shortradiographswereequivalenttopanoramic radiographsforevaluatingtheanatomicalaxisofthelowerlimbsinpatientswithadvanced osteoarthritis.Themeasurementsusedalsoshowedhighratesofinterandintraobserver concordanceandreproducibility.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedintheDepartmentofOrthopedicsandTraumatologyandtheDepartmentofRadiologyoftheHospitaldaForc¸aAérea doGaleão,RiodeJaneiro,RJ,Brazil.
∗
Correspondingauthor.
E-mail:[email protected](R.P.eAlbuquerque). http://dx.doi.org/10.1016/j.rboe.2015.05.003
joelho.
Avaliac¸ão
inter
e
intraobservadores
Palavras-chave:
Osteoartrite/radiografia Joelho
Extremidadeinferior
r
e
s
u
m
o
Objetivo: Fazeraanálisecomparativaintereintraobservadordamedidadoeixoanatômico entreasradiografiaspanorâmica,dosmembrosinferiores(MMII)comraioanteroposterior (AP)eapoiobipodálicoeAPcomcargabipodalemfilmecurto.
Métodos: Foifeitoestudodeacuráciaquecomparoumedidasradiográficasem47joelhosde pacientesdoambulatóriodecirurgiadojoelho,porosteoartrite(OA).Aavaliac¸ãoradiográfica usadafoiapadronizadaparaaprogramac¸ãodeATJ,incluindoasincidênciaspanorâmicados MMIIemAPeasradiografiascurtasdosjoelhosemAPeperfil,todascomapoiobipodálico. Emseguida,asradiografiaspanorâmicasecurtasemAPtiveramoseixosanatômicosdos MMIIouângulofemorotibial(AFT)medidosporcincoexaminadoresindependentes,dos quaistrêseramconsideradosmaisexperientesedoismenosexperientes.Todasasmedidas foramrefeitaspelosmesmosexaminadoresemumintervalonãomenordoque15dias.A análiseestatísticafoifeitacomousodocoeficientedecorrelac¸ãointraclasses(ICC)para avaliaraconcordâncianamedidadoeixoanatômicointereintraobservadores.
Resultados:Apósanáliseestatísticaobservou-seforteconcordânciasignificativaentreoeixo anatômicomedidonasradiografiaspanorâmicaecurtaparatodososcincoexaminadores eparaambasasmedidas.
Conclusões: Nascondic¸ões estudadasa radiografia curtaequipara-se à panorâmicana avaliac¸ãodoeixoanatômicodosMMIIempacientescomOAavanc¸ada.Amensurac¸ãousada tambémmostraaltataxadeconcordânciaereprodutibilidadeintereintraobsevadores.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
The alignment of the lower limbs, evaluated according to their anatomicaland mechanical axes,isconsidered to be a fundamental element in the genesis and progression of degenerativejointdiseaseorosteoarthritis(OA)oftheknee.1–6
Valgusorvarusdeformitiesofthekneearerelatedtotherisk thatthelateralandmedialcompartments,respectively,may beaffected.2,3,5,6Knowledgeofthisalignmentalsobecomes
essentialforadequatetherapeuticplanningforpatientswith kneeOA,especiallyforthosewhoareawaitingosteotomyor arthroplasty,aswellasfortheirpostoperativefollow-up.3,7–10
Although clinical assessment is correct and necessary, radiographicexaminationisafundamentaltoolfor preopera-tiveplanning.3,7–10Panoramicradiographyofthelowerlimbs
inAPviewwithweightborneeitherononefootoron two feetisconsideredtobethegoldstandardandiswidely recom-mendedinthesesituations.1–4,7–13However,shortradiographs
ofthekneesremainessentialforbetterunderstanding, stag-ingandclassificationofdegenerativedisease,inAPandlateral views,alsowithweight-bearing.2,5,6,14–18Therearelogistic
dif-ficultiesinproducingpanoramicradiographs,whichmaybeof dubiousqualitywhenperformed.Thehipsoranklesareoften omitted,whichmaybebecauseofpoorpositioningbetween theapparatusandthepatient,inadequatepenetrationofone oftheextremitiesorincompatibilitybetweenthesizesofthe filmandpatient. Moreover,panoramicradiography exposes patientstogreaterquantitiesofionizingradiationandleads toadditionalcosts.5,6,15Inthislight,weconceptualizedastudy
with the following objectives:to evaluate the reliability of
measurementsofthefemorotibialangle(FTA)onshort radio-graphsincomparisonwiththevaluesfoundonpanoramic radiographs ofthe lower limbs; and toevaluatethe repro-ducibilityofinterobserverandintraobservermeasurements.
Materials
and
methods
Anaccuracystudy wasconductedtocompareradiographic measurementson50knees,fromthefirstpatientswho pre-sentedatthekneesurgeryoutpatientclinicofourinstitution withanindicationfortotalkneearthroplasty(TKA)because ofOA:KellgrenandLawrence193or4andAhlbäck203–5,as
assessedbytheseniorresearcher(MNG).Theonlyexclusion criterionwasaradiographicexaminationofinadequate qual-ity,andthreekneeswerethuseliminatedfromthisstudy.The radiographic evaluationusedwas theonestandardizedfor schedulingTKA,includingpanoramicradiographsofthelower limbsinAPview(longradiographs)andshortradiographsof thekneesinAPinlateralviews,allwithweightborneontwo feet.
Theradiographicexaminationswereperformedinthe radi-ology sectorofourservice usingthe PrestigeSI apparatus. The equipment wasoperated bya singleradiology techni-cian,withouttheaidofradioscopy.Carewastakentoensure that the knees were extendedtotheir maximum and that thepatients’patellaewerefacingforwards.Thefilmsforthe panoramicradiographsallmeasured130cm×35cm(Kodak®) and the films for the short radiographs, 24cm×30cm (Kodak®). Following this,the anatomical axesofthe lower
Fig.1–Panoramicradiographofthelowerlimb.
fiveindependentexaminers.Twoofthese(MNGandRPA)were consideredtobemoreexperiencedandhadbeentitular mem-bersoftheBrazilianSocietyofOrthopedicsandTraumatology (SBOT)formorethan5years;one(LFM)wasconsideredtohave intermediate-levelexperienceandhadbeenatitularmember oftheSBOTforlessthan1year,andwasdoingspecialization traininginkneetraining;andtwo(GNCandRBF)were consid-eredtobelessexperiencedandwerestudyinginthethirdyear ofmedicalresidencyinorthopedicsandtraumatology.Allof themeasurementsweremadeagainbythesameexaminers afteranintervalofnotlessthan15days.
The anatomical axis was evaluated on the panoramic radiographsbymeansoflinestracedoutalongthelongaxes ofthefemurandtibia(Fig.1).Themeasurementtechniquefor theshortradiographswasassuggestedbyKhanetal.,6based
onthepreviousstudiesofHsuetal.11andKrausetal.5Apoint
wasdefinedonthefemuratthecenteroftheintercondylar space,andanotherone10cmproximally,atthemidpointof thedistancebetweenthetwoexternalcortexes.The measure-mentonthetibiastartedfromapointmarkedatthecenter ofthe tibialeminences,withasecondpoint marked10cm distally,atthemidpointofthedistancebetweenthetwo exter-nalcortexes.Linesjoiningthefemoralandtibialpointswere tracedoutandtheirintersectioncorrespondedtothe anatom-icalaxisorfemorotibialangle(FTA)(Fig.2).
Twenty-sevenpatientswereevaluated,ofwhom24were women(88.9%)and3weremen(11.1%),withameanageof73 yearsand4months(range:from48yearsand5monthsto88 yearsand2months)(Table1).
InrelationtothestagingoftheOA,30knees(63.8%)were classifiedasKellgrenandLawrence19gradeIII and17(36.2%)as gradeIV.AccordingtotheAhlbäckclassification,20asmodified byKeyesetal.,21fivekneesweregradeIII (10.6%),30gradeIV (63.9%)and12gradeV (25.5%)(Table1).
Fig.2–ShortradiographofthekneeinAPview,with weight-bearingontwofeetandusingthetechniqueofFTA measurement.
Inthestatisticalmethodology,theinterandintraobserver concordanceregardingthemeasurementsoftheanatomical axiswereevaluatedusingtheintraclasscorrelationcoefficient (ICC).22Thecriterionadoptedfordeterminingsignificancewas
thelevel of1%.TheanalysiswasprocessedusingtheSPSS statisticalpackage,version13.0.
ItisknownthattheclosertheICCistoone,thestronger (ormoreperfect)theconcordanceisbetweentheobservers.In thiscase,thetechniquesweresimilarfromanumerical (quan-titative)pointofview.Ontheotherhand,theclosertozerothe ICCis,thegreaterthediscordancewillbe,meaningthatthe valuescannotbereproducedandthedifferencesobservedare notrandom.
Through several studies and simulations,it canbe said that:
ICC≤ 0.20–noconcordance; 0.20<ICC≤ 0.40–weakconcordance; 0.40<ICC≤ 0.60–moderateconcordance; 0.60<ICC≤0.80–strong(good)concordance; ICC>0.80–verystrong(excellent)concordance.
Results
Patientnumber Age(years) Rightknee Rightknee Leftknee Leftknee Ahlbäck KellgrenandLawrence Ahlbäck KellgrenandLawrence
1 68.7 4 3
2 67.8 4 3 4 3
3 88.2 5 4 5 4
4 76.4 4 3 5 4
5 61.4 3 3 3 3
6 71.1 4 4
7 82.2 5 4
8 74.2 4 3 5 4
9 74 4 3 4 3
10 72 4 4 4 3
11 65 3 3 4 3
12 74.6 4 4 4 3
13 69.7 4 3 4 3
14 76.9 5 4
15 83.2 5 4
16 74.1 4 3 4 3
17 75.6 4 4 4 3
18 60.7 3 3 3 3
19 71.8 4 3 4 3
20 83.7 5 4 5 4
21 69 4 3 4 3
22 74.3 4 4 5 4
23 85 5 4 5 4
24 72.7 4 3 4 3
25 48.4 4 3 4 3
26 66 4 3
27 85.2 4 3
Source:hospitalfiles,2013.
radiographs,itwas7.7◦.Inthefinalmeasurements,themean
FTA on the short radiographs was 7.5◦ and on the long
radiographs,7.6◦.Consideringeachexaminerseparately,the
anatomicalaxismeasurementvariedbyamaximumof13◦
betweenthelongandshortradiographsandbyamaximum
of6◦ betweentheinitialandfinalmeasurements.Fromthe
statisticalanalysis,itwasobservedthattherewasstrongly sig-nificantconcordance(ICC>0.88,asaminimum)betweenthe evaluationsusingshortandpanoramicradiographs(p<0.001),
Table2–Concordancebetweenradiographs:short versuspanoramic.
Observer ICC 95%CI pValue
Measurement1 RBF 0.885 0.804–0.934 <0.001 GNC 0.915 0.853–0.952 <0.001 MNG 0.941 0.897–0.967 <0.001 LFM 0.914 0.851–0.951 <0.001 RPA 0.945 0.903–0.969 <0.001 Measurement2 RBF 0.928 0.874–0.959 <0.001 GNC 0.944 0.902–0.968 <0.001 MNG 0.953 0.918–0.974 <0.001 LFM 0.916 0.854–0.952 <0.001 RPA 0.945 0.903–0.969 <0.001
Source:hospitalfiles,2013.
ICC,intraclasscorrelationcoefficient;95%CI,95%confidence inter-valforICC.
forallthefiveobserversandforbothofthemeasurements (Table2).
Itwasalsoobservedthattherewasstronglysignificant con-cordance(ICC>0.97,asaminimum)betweenmeasurements 1and2(p<0.001),forallthefiveobserversandforbothtypes ofradiograph(Table3).
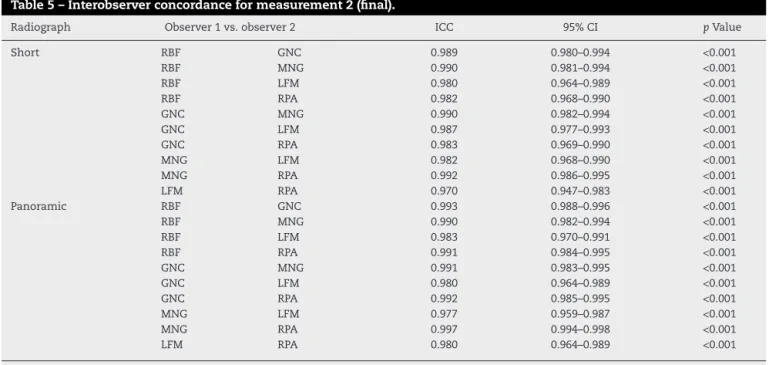
Finally,itwasobservedthattherewasstronglysignificant concordance(ICC>0.96,asaminimum)betweenallpairsof observers (p<0.001),forbothtypesofradiographandusing measurements1and2(Tables4and5).
Table3–Intraobserverconcordance:measurement1 (initial)versusmeasurement2(final).
Radiograph Observer ICC 95%CI pValue
Short RBF 0.989 0.980–0.994 <0.001 GNC 0.986 0.975–0.992 <0.001 MNG 0.996 0.992–0.998 <0.001 LFM 0.989 0.980–0.994 <0.001 RPA 0.998 0.997–0.999 <0.001 Panoramic RBF 0.977 0.959–0.987 <0.001 GNC 0.988 0.979–0.994 <0.001 MNG 0.997 0.995–0.999 <0.001 LFM 0.986 0.975–0.992 <0.001 RPA 0.998 0.997–0.999 <0.001
Source:hospitalfiles,2013.
Table4–Interobserverconcordanceformeasurement1(initial).
Radiograph Observer1vs.observer2 ICC 95%CI pValue
Short RBF GNC 0.984 0.972–0.991 <0.001
RBF MNG 0.987 0.977–0.993 <0.001
RBF LFM 0.977 0.959–0.987 <0.001
RBF RPA 0.979 0.963–0.988 <0.001
GNC MNG 0.982 0.968–0.990 <0.001
GNC LFM 0.973 0.952–0.985 <0.001
GNC RPA 0.976 0.957–0.986 <0.001
MNG LFM 0.972 0.951–0.984 <0.001
MNG RPA 0.993 0.988–0.996 <0.001
LFM RPA 0.968 0.943–0.982 <0.001
Panoramic RBF GNC 0.981 0.966–0.989 <0.001
RBF MNG 0.978 0.960–0.987 <0.001
RBF LFM 0.977 0.960–0.987 <0.001
RBF RPA 0.981 0.966–0.989 <0.001
GNC MNG 0.989 0.980–0.994 <0.001
GNC LFM 0.981 0.967–0.989 <0.001
GNC RPA 0.990 0.982–0.994 <0.001
MNG LFM 0.980 0.964–0.989 <0.001
MNG RPA 0.997 0.994–0.998 <0.001
LFM RPA 0.981 0.967–0.989 <0.001
Source:hospitalfiles,2013.
ICC,intraclasscorrelationcoefficient;95%CI,95%confidenceintervalforICC.
Discussion
Theappropriateradiographicmethodforevaluatingpatients withkneeOAisstillamatterofdebate.5,6,9,13–16,18Panoramic
radiography is traditionally recommended whenthere is a need to assess the lower-limb alignment.1–4,7–13 Moreland
etal.7statedthatitwasessentialformeasuringtheaxial
align-mentofthelowerlimbs.However,itisdifficulttoperform,
oftenpresentsdeficientquality, exposespatientstogreater amountsofionizingradiationandismoreexpensive.5,6,15
Krausetal.5comparedkneealignmentsusingpanoramic
radiographsonthelower limbsinAPviewandusingshort radiographsinaflexedpositioninposteroanterior(PA)view, andalsocomparedthesewithclinicalmeasurements.They observed that the results from clinical measurements and from short radiographs correlated well with those from panoramicradiographs.Theythereforeconcludedthatthese
Table5–Interobserverconcordanceformeasurement2(final).
Radiograph Observer1vs.observer2 ICC 95%CI pValue
Short RBF GNC 0.989 0.980–0.994 <0.001
RBF MNG 0.990 0.981–0.994 <0.001
RBF LFM 0.980 0.964–0.989 <0.001
RBF RPA 0.982 0.968–0.990 <0.001
GNC MNG 0.990 0.982–0.994 <0.001
GNC LFM 0.987 0.977–0.993 <0.001
GNC RPA 0.983 0.969–0.990 <0.001
MNG LFM 0.982 0.968–0.990 <0.001
MNG RPA 0.992 0.986–0.995 <0.001
LFM RPA 0.970 0.947–0.983 <0.001
Panoramic RBF GNC 0.993 0.988–0.996 <0.001
RBF MNG 0.990 0.982–0.994 <0.001
RBF LFM 0.983 0.970–0.991 <0.001
RBF RPA 0.991 0.984–0.995 <0.001
GNC MNG 0.991 0.983–0.995 <0.001
GNC LFM 0.980 0.964–0.989 <0.001
GNC RPA 0.992 0.985–0.995 <0.001
MNG LFM 0.977 0.959–0.987 <0.001
MNG RPA 0.997 0.994–0.998 <0.001
LFM RPA 0.980 0.964–0.989 <0.001
Source:hospitalfiles,2013.
panoramic radiographs were unavailable.5 McGrory et al.15
were unableto demonstrateany advantageforlong radio-graphsovershortradiographsforpreoperativeplanning.
Furthermore,inageneralmanner,shortradiographson thekneesareindispensableatanyphaseofdegenerativejoint disease.2,5,6,14–18 Therefore,if shortradiographscanprovide
reliableinformationon alignments,panoramic radiographs becomeunnecessary.Thiswasourmotivationforthepresent study.
From a methodological point of view,we attempted as muchaspossibletoreproducethesituationencounteredby orthopedistsintheirdailyclinicalpractice.Thepatients’ posi-tioningwasnotcheckedusingradioscopybeforeproducing theradiographs,giventhatthisisaresourcesfoundinveryfew centersinBrazil.Thepatientsweresimplyinstructedtokeep theirkneesextendedasmuchaspossible,withthepatellae orthogonaltotheX-raytube,soastominimizethepossibility ofrotationaldeviation.
Moreland et al.7 postulated that rotation of the lower
limbsaffectstheapparentalignment.Inkneeswithpoor flex-ion,externalrotationsimulatesanincreaseinvarus,while internal rotation accentuates valgus. This emphasizes the importanceofproperlydirectingthepatellaeforwards,soas toattenuatethisproblem.7Similarresultswerepresentedby
Brouweretal.,13whorecommendedthatfluoroscopyshould
onlybeusedonkneeswithcontractureswhenflexed. Specognaetal.9demonstratedthatradiographsproduced
withweight-bearingononefootwerenotsuperiortothose withweight-bearingonbothfeet,inevaluationson40patients withkneeOAinassociationwithvarusdeformity.Theyeven recommended that weight-bearing on both feet should be used routinely in preoperative assessments.Based on this finding,wealsochosetouseradiographswithweight-bearing onbothfeet.
Withregardtotheresults,it wasobservedthattheFTA measurementson the shortradiographsusing the method described here were concordant with those obtained from longradiographs.Inrelationtothestrengthofconcordance, itwasnoticedthattherewasanimprovementwhenthe mea-surementsweremadeforthesecondtime,probablybecause ofgreater familiaritywith the method presented. Another importantfindingwasthatbetterresultswereobtainedbythe moreexperiencedexaminers inbothmeasurements. How-ever,eventhemeasurementsmadebythelessexperienced examinerspresentedahighconcordanceindex.
Khan et al.6 were able to demonstrate an association
betweentheevolutionofthekneeOAandtheangular devi-ations measuredon shortradiographsusing the technique describedinthepresentstudy.However,theydidnotventure toindicatethisradiographictechniquealoneforpreoperative planningofosteotomy.6
Regarding the interobserver evaluation, it was again observedthatforbothmeasurements,therewasgreater con-cordance(i.e.greaterICC)betweenthetwoexaminerswith greaterexperience.However,independentofthelevelof expe-rience,therewashighconcordancebetweenallthepairsof examiners.
Finally,theintraobserverconcordancepresentedthesame behavior as seen in the preceding evaluation, with high
relationobtainedamongthosewithgreatestexperience. Thus, the resultsfrom the present study demonstrated that themethod proposedformeasuringthe FTA onshort radiographswasreliableandreproducible,independentofthe experienceoftheexaminingphysician.Othercorrelated eval-uationswouldservetostrengthenthedataseeninthepresent studyandwouldopenuptheprospectofsimplifying evalua-tionsontheangulardeviationsofthelowerlimbsinpatients withkneeOA.
Conclusions
Under the conditionsofthis study,shortradiographs were equaltopanoramicradiographsforevaluatingthe anatomi-calaxisofthelowerlimbsinpatientswithadvancedOA.The measurementusedalsoshowedhighinterandintraobserver concordanceandreproducibility.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.SharmaL,LouC,CahueS,DunlopDD.Themechanismofthe effectofobesityinkneeosteoarthritis:themediatingroleof malalignment.ArthritisRheum.2000;43(3):568–75.
2.SharmaL,SongJ,FelsonDT,CahueS,ShamiyehE,Dunlop DD.Theroleofkneealignmentindiseaseprogressionand functionaldeclineinkneeosteoarthritis.JAMA.
2001;286(2):188–95.
3.CerejoR,DunlopDD,CahueS,ChanninD,SongJ,SharmaL. Theinfluenceofalignmentonriskofkneeosteoarthritis progressionaccordingtobaselinestageofdisease.Arthritis Rheum.2002;46(10):2632–6.
4.FelsonDT,GogginsJ,NiuJ,ZhangY,HunterDJ.Theeffectof bodyweightonprogressionofthekneeosteoarthritisis dependentonalignment.ArthritisRheum.2004;50(12):3904–9. 5.KrausVB,VailTP,WorrelT,McDanielG.Acomparative
assessmentofalignmentangleofthekneebyradiographic andphysicalexaminationmethods.ArthritisRheum. 2005;52(6):1730–5.
6.KhanFA,KoffMF,NoiseuxNO,BernhardtKA,O’ByrneMM, LarsonDR,etal.Effectoflocalalignmentoncompartmental patternsofkneeosteoarthritis.JBoneJointSurgAm. 2008;90(9):1961–9.
7.MorelandJR,BassetLW,HankerGJ.Radiographicanalysisof theaxialalignmentofthelowerextremity.JBoneJointSurg Am.1987;69(5):745–9.
8.KawakamiH,SuganoN,YonenobuK,YoshikawaH,OchiT, HattoriA,etal.Effectsofrotationonmeasurementoflower limbalignmentforkneeosteotomy.JOrthopRes.
2004;22(6):1248–53.
9.SpecognaAV,BirminghamTB,HuntMA,JonesIC,JenkynTR, FowlerPJ,etal.Radiographicmeasuresofkneealignmentin patientswithvarusgonarthrosis:effectofweightbearing statusandassociationswithdynamicjointload.AmJSports Med.2007;35(1):65–70.
11.HsuRW,HimenoS,CoventryMB,ChãoEY.Normalaxial alignmentofthelowerextremityandload-bearing distributionattheknee.ClinOrthopRelatRes. 1990;(255):215–27.
12.BrouwerRW,JakmaTS,Bierma-ZeinstraSM,GinaiAZ, VerhaarJA.Thewholelegradiograph:standingversussupine fordeterminingaxialalignment.ActaOrthopScand. 2003;74(5):565–8.
13.BrouwerRW,JakmaTS,BrouwerKH,VerhaarJA.Pitfallsin determiningkneealignment:aradiographiccadavericstudy.J KneeSurg.2007;20(3):210–5.
14.LonnerJH,LairdMT,StuchinSA.Effectofrotationandknee flexiononradiographicalignmentintotalknee
arthroplasties.ClinOrthopRelatRes.1996;(331):102–6. 15.McGroryJE,TrousdaleRT,PagnanoMW,NigburM.
Pre-operativehip-to-ankleradiographsintotalknee arthroplasty.ClinOrthopRelatRes.2002;(404):196–202. 16.PeterfyC,LiJ,ZaimS,DuryeaJ,LynchJ,MiauxY,etal.
Comparisonoffixed-flexionpositioningwithfluoroscopic
semi-flexedpositioningforquantifyingradiographic joint-spacewidthintheknee:test–retestreproducibility. SkeletRadiol.2003;32(3):128–32.
17.SchmidtJE,AmramiKK,ManducaA,KaufmanKR.
Semi-automateddigitalimageanalysisofjointspacewidth inkneeradiographs.SkeletRadiol.2005;34(10):639–43. 18.RadtkeK,BecherC,NollY,OstermeierS.Effectoflimb
rotationonradiographicalignmentintotalknee
arthroplasties.ArchOrthopTraumaSurg.2010;130(4):451–7. 19.KellgrenJH,LawrenceJS.Radiologicalassessmentof
osteo-arthrosis.AnnRheumDis.1957;16(4):494–502. 20.AlhbäckS.Osteoarthritisoftheknee.Aradiographic
investigation.ActaRadiolDiagn.1968;277Suppl.:7–72. 21.KeyesGW,CarrAJ,MillerRK,GoodfellowJW.Theradiographic
classificationofmedialgonarthrosis–correlationwith operationmethodsin200knees.ActaOrthopScand. 1992;63(5):497–501.