INVESTIGATION
OF THE
SALMONELLA TYPHI-PARA TYPHICARRIER
STATE IN CASES OF SURGICAL
INTERVENTION
FOR GALLBLADDER
DISEASE1
Conrad0 Ristori,z H&ctor Rodriguez,*
Patricia Vicent,* Her&n
Lobos,S
Karen D’Ottone,j
Julio Garcia,3 Maria Eugenia Pinto,4
Patricia Nercelles,4 and Luis Cisneros5
High typhoidfever morbidity in Chile, combined with outside evidence of a cor- relation between the S. typhi carrier state andgallbladder disease, led to a st&y of 1,000 bile specimens jam vesicular disease patients. The results suggest that the high prevalence of gallbladder disease in Chile filays an important background role in the transmission of typhoidfever.
Introduction
Typhoid fever morbidity has exhibited a rising trend in Chile, particularly since 1976, reaching annual rates as high as 120 cases per 100,000 inhabitants (1,). This situation is sur- prising, partly because the country is not among the world’s least developed in terms of either economic or sanitary conditions, and partly because the problem is particularly severe in Santiago, which accounts for two- thirds of the cases, even though Santiago’s water supply and excreta disposal systems provide the highest degree of coverage af- forded any Chilean city (I-3).
As is well-known, a leading role in typhoid transmission is played by carriers (4-S), their numbers augmented by the existence of at least three subclinical or inapparent cases for each case diagnosed. For this reason, a high prevalence of gallbladder disease in Chile (7- II) prompted us to seek a link between that disease and typhoid transmission, similar to the one reported in other countries. (Past epi- demiologic and pathologic surveys in Chile
l Al so appearing in Spanish in the B&in de la Ofiina
Sanitaria Panamericana 93(4), 1982.
2Program Support Department, Ministry of Health of
Chile.
%nstitute of Public Health of Chile. $San Juan de Dios Hospital, Santiago, Chile. %hort-term consultant from the University of Mary- land, U.S.A.
had revealed the presence of gallstones in 50 and 20.5 per cent of adult female and male survey populations, respectively-7, 8.)
Goals
The aim of the study was to analyze the aerobic bacterial flora of bile obtained from cholecystectomy patients in the city of Santia- go, checking particularly for salmonellae of the typhi and paratyphi types. Similar surveys performed in countries with low incidences of enteric infections had revealed the presence of a wide variety of bacteria in bile from roughly a third of the surgically treated gallbladder disease cases but none in the S. typhi-paratyphi group (12-18). It was hoped that the findings of our study, when projected to include the total estimated number of gallbladder disease cases in Santiago, would help in developing an approximate idea of the number of typhoid carriers in that city.
Materials and Methods
The study, which was limited to the urban area of Santiago, was supported by the surgi- cal departments of the city’s principal adult
hospitals. Specimens were taken during a
three-month period beginning in July 1980 from patients selected at random, until the targeted total of 1,000 specimens had been collected.
162 PAHO BULLETIN l vol. 16, no. 2, 1982
These specimens were obtained by surgeons at the participating facilities, who extracted bile from cholecystectomy patients by gall- bladder puncture at the time of surgery. Each bile specimen thus obtained, together with a sample of the patient’s blood, was sent to the Public Health Institute of Chile. There the bile specimens were tested for the presence of aerobic microorganisms by culturing in blood agar and for salmonellae by culturing in sal- monella-shigella and xylose-lactose desoxy- cholate media, while the blood samples were tested for S. typhi by subjecting them to Widal’s serum test. Concurrently, one partic- ipating hospital (the San Juan de Dios Hospi- tal) tested the bile specimens obtained from its own patients for anaerobic microorganisms. An account of the results obtained with these latter tests is to be published separately.
Results
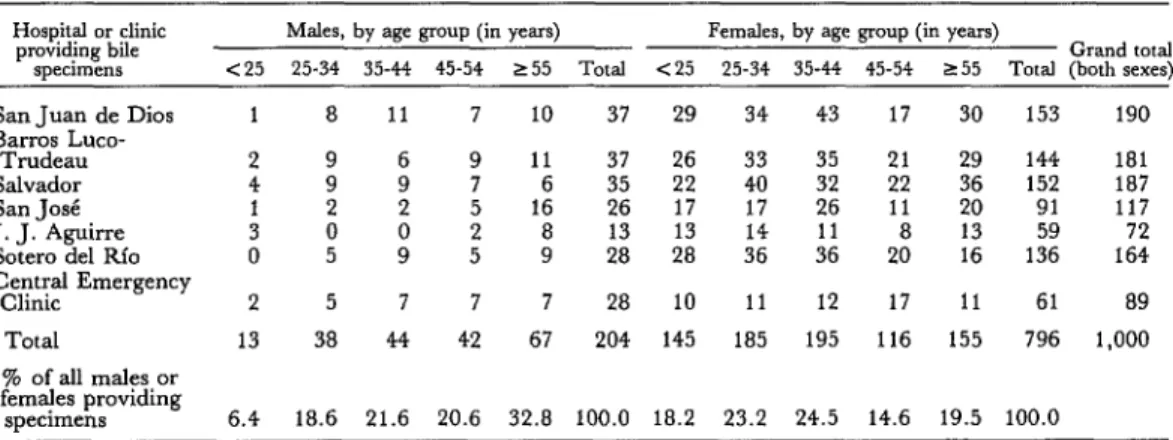
Table 1 shows the sex and age distribution of the 1,000 cholecystectomy patients from
whom bile specimens were obtained. Far
more cholecystectomies were performed on
females than on males, the ratio of male to female cholecystectomy patients being on the order of 4: 1 or 5: 1 at all the participating fa- cilities except the Central Emergency Clinic, which handled only emergencies and where the ratio was roughly 2:l. This exception can
be explained by the relatively greater frequen- cy with which men were operated on for acute conditions (including empyemas, cholangitis, and obstructions).
As Table 1 also indicates, the proportion of male subjects given the operation increased with age, the smallest part of the total (6.4 per cent) being comprised of males under 25 years old and the largest (32.8 per cent) being com- prised of males over 54 years old. The age dis- tribution offemale subjects wasmore uniform, the group under 25 years old accounting for a fair share (18.1 per cent) of the total and those over 54 accounting for a relatively modest 19.5 per cent.
The leading cause of surgery was gallstones, which prompted 45.7 and 51.9 per cent of the operations in males and females, respectively. The next leading causes were chronic chole- cystitis (prompting 28.6 and 31.2 per cent, respectively) and acute cholecystitis (prompt- ing 23 .O and 13.5 per cent, respectively).
Vesicular empyema, cancer, and other
diagnoses accounted for a very small propor- tion (less than 4 per cent) of the operations. However, the percentage of cases involving gallstones was somewhat higher than indi- cated, because a significant share of the pa- tients operated on for cholecystitis were found to have gallstones.
The percentages of bile cultures yielding positive bacteriologic results, by place of oper-
Table 1. Surgical subjects providing bile specimens, by age, vex, and the Santiago hospital or clinic
where the operation was performed (July-October 1980).
Hospital or clinic
providing bile Males, by age group (in years) Females, by age group (in years) Grand total
specimens <25 25-34 35-44 45-54 255 Total <25 25-34 35-44 45-54 255 Total (both sexes)
San Juan de Dios B;;~~;,uco-
Salvador San Jod J. J. Aguirre Sotero de1 Rio
Clk;m$ Emergency
Total
% of all males or fem;?es providing
specimens 1 2 4 i 0 2 13
6.4 18.6 21.6 20.6 32.8 100.0 la.2 23.2 24.5 14.6 19.5 100.0
a 9 9 i 5 5 38
11 7 10 37 29 34
11 6 16 a 9 37 ;z 13 28
26 33
22 40
17 17
:i ;6’
7 7 7 28 10 11
44 42 67 204 145 185
43 35 ;z ifi 12 195
17 30 153 190
21 22 11 a 20 29 2 13 16
144 la1
152 la7
91 117
59 72
136 164
17 11 61 a9
Ristori et al. l SALMONELLA TYPHI-PARATYPHI CARRIER STATE 163
ation and sex, are shown in Table 2. One of the highest rates of positivity was found in specimens from the San Juan de Dios Hospi- tal, a fact that could be wholly or partly ac- counted for by special circumstances involving a number of those specimens. Specifically, the San Juan de Dios Hospital, besides testing for anaerobic microbes, also tested for aerobic bacteria at its own laboratory. These latter tests did not precisely match those performed at the Public Health Institute, because the institute employed media selective for S. typhi
that may have discouraged development of
other species. Therefore, the fact that the results of 51 examinations performed at the San Juan de Dios Hospital’s laboratory are in- cluded in the results reported here could have contributed to the fairly high positivity rate found among specimens from that facility.
The highest percentage of positive speci- mens was obtained from patients at the Cen- tral Emergency Clinic, a facility where only emergency surgery was performed and where acute conditions accounted for a large share of the cases involved.
Overall, taking specimens from the seven participating facilities together, male subjects were found to yield a higher percentage of positive specimens (35.8 per cent) than did female subjects (26.6 per cent), a finding that could be associated with the higher incidence of acute conditions observed among male sub- jects.
Table 3 compares the results for males and
females in different age groups. Among
males, if one ignores the small number of specimens from males under 25 years old, one observes a rise in the rate of positive results among older age groups. This rise was not so
pronounced among females-except in the
oldest female group (55 and over), where the rate of positive results was 49.4 per cent.
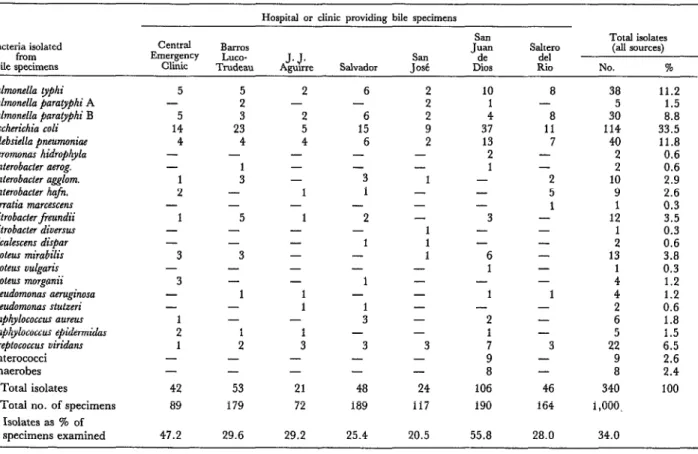
As Table 4 indicates, 340 bacterial isolates were obtained from the 1,000 bile cultures examined. The observation is consistent with the results of a number of foreign studies. The
most frequently encountered bacteria were
Escherichia coli (accounting for 33.5 per cent of
the isolates), bacteria in the S. typhi-paratyphi group (21.5 per cent), Klebsiella pneumoniae (11.8 per cent), and Streptococcus uiridans (6.5 per cent). Other aerobic bacteria accounted for smaller percentages. Overall, the total of 340 isolates were obtained from 285 bile speci- mens, some specimens yielding multiple iso- lates.
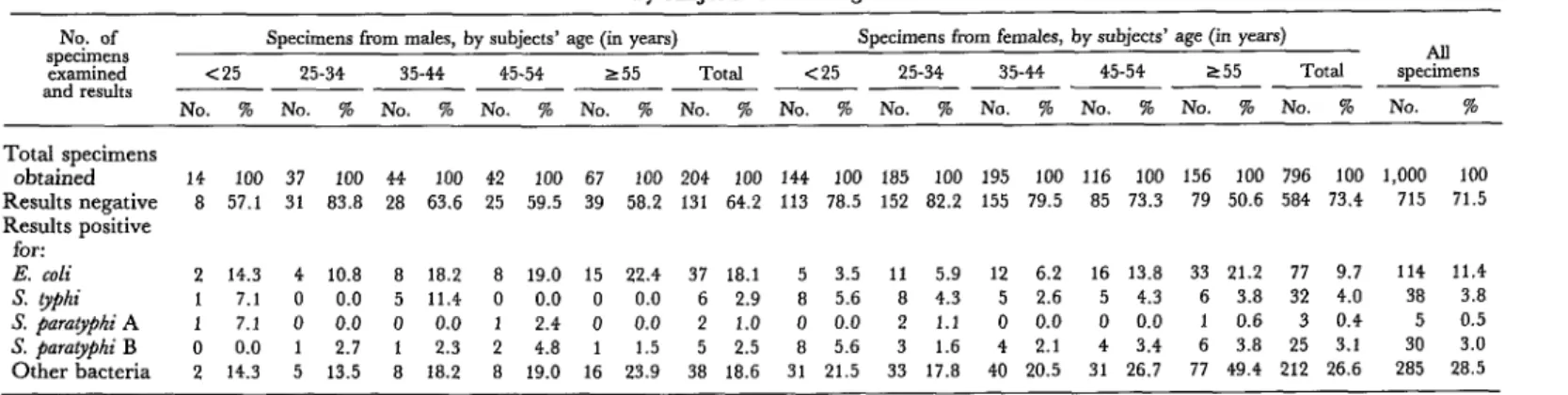
Table 5 shows the distribution of salmonel- la, E. co& and other isolates by the subjects’ sex and age. In general, far more males (18.1 per cent) than females (9.7 per cent) yielded bile specimens positive for E. coli; the percent- age of specimens positive for E. coli increased with age among both sexes, reaching its peak in the group over 54 years old. It was quite
common for E. coli to be isolated from
specimens that also yielded other bacteria. The percentages of specimens found posi- tive for S. typhi and S. paratiphi were quite similar. Specifically, S. typhi was encountered in specimens from 2.9 and 4.0 per cent of the male and female subjects, respectively, while S. parapphi A was found in 1 .O and 0.4 per cent, respectively, and S’. paratyphi B was found in 2.5 and 3.1 per cent, respectively. The age distribution of the male subjects yielding these various isolates could not be analyzed effectively because of the small num- bers of specimens involved. In the case of women, a slight decline in the percentage of positive cultures was observed with increasing age, but this was not statistically significant. Because S. typhi accounts for the bulk of the diagnosed enteric infections caused by itself and 5’. paratyphi, it seems evident that the results (showing roughly equal proportions of the two microorganisms) do not reflect what is observed in clinical practice.
Table 2. Results of bile specimen cultures, by sex and tbe Santiago facility providing the specimen.
Hospital or $nic providing SpXltllCtX
San Juan de Dios Barros Loco-Trudeau Salvador
San JOSE J. J. Aguirre Sotero de1 Rio
Central Emergency Clinic
Total
specimens from males
TCJtal NO. NO.
specimens negative positive
37 16 21
3”: 30 23 12 7
26 21 5
13 9 4
28 18 10
28 14 14
204 131 73
%
positive
56.8 18.9 34.3 19.2 30.8 35.7 50.0
35.8
Specimens from females Specimen from both sexes
Total NO. NO. % Total NO. NO. %
specimens negative positive positive specimens negative positive positive
153 115 38 24.8 190 131 59 31.1
144 101 43 29.9 181 131 50 27.6
152 116 36 23.7 187 139 48 25.7
91 75 16 17.6 117 96 21 17.9
59 40 19 32.2 72 49 23 31.9
136 101 35 25.7 164 119 45 27.4
61 36 25 41.0 89 50 39 43.8
796 584 212 26.6 1,000 715 285 28.5
Table 3. A comparison of culture results obtained with bile specimens from different sexes and age groups.
Sex of subjects providing specimens
and bacteriologic results
Male specimens:
Positive Negative
Total
Female sfiecimem:
Positive Negative
Total
All specimens:
Positive Negative
Total
Age of subjects providing specimens (in years)
<25 25-34 35-44 45-54 255 All age groups
NO. % NO. % NO. % NO. % NO. % NO. %
6 42.9 6 16.2 16 36.4
::
40.5 28 41.8 73 35.8
8 57.1 31 83.8 28 63.6 59.5 39 58.2 131 64.2
14 100.0 37 100.0 44 100.0 42 100.0 67 100.0 204 100.0
31 21.5 33 17.8 40 20.5 31 26.7 77 49.4 212 26.6
113 78.5 152 82.2 155 79.5 85 73.3 79 50.6 584 73.4
144 100.0 185 100.0 195 100.0 116 100.0 156 100.0 796 100.0
37 23.4 39 17.6 56 23.4 48 30.4 105 47.1 285 28.5
121 76.6 183 82.4 183 76.6 110 69.6 118 52.9 715 71.5
Table 4. Bacterial isolates obtained from the 1,000 bile specimens examined.
Bacteria isolated from bide specimens
Salmonella typhi Salmonella paratyphi A Salmonella paratyphi B Eschenchia coli Klebsiella pneumoniae Aeromonas hidrophyla Enterobacter aerog. Enterobacter agglom. Enterobacter hafn. Serratia marcescens Citrobacter freundii Citrobacter diversus Alcalescenr dispar Proteus mirabilis Proteus vulgaris Proteus morganii Pseudomonas aeruginosa Pseudomonas stutreri Staphylococcw awes Staphylococcus epidermidas Streptococcus viridans Enterococci Anaerobes
Total isolates
Total no. of specimens Isolates as % of specimens examined
Hospital or clinic providing bile specimens
central BalT0.Y Juan San Salter0 Total isolates
Emergency LlU2.Y
AJ&;re SClll D%s
de1 (all .3ources)
Chic Trudeau Salvador .los6 Rio NO. %
5 - 5 14 4 - - 1 2 - 1 - - 3 - 3 - - : 1 - - 42 89
47.2 29.6 29.2 25.4 20.5 55.8 28.0 34.0
5 2 3 23 4 - : - - 5 - - 3 - - 1 - - 1 2 - - 53 179 2 - 2 5 4 - - - 1 - 1 - - - - - 1 1 - 1 3 - - 21 72 6 - 6 15 6 - -3 1 -2 - 1 - - 1 - 1 3 - 3 - - 48 189 ; 2 9 2 - - 1 - - - - -
- 2
- 1
3 7
- 9
- 8
24 106
117 190
10 1 4 37 13 2 1 - - - 3 - - 6 1 - 1 8 - 8 11 7 - -2 5 1 - - - - - - 1 - - - 3 - - 46 164
38 11.2
5 1.5
30 8.8
114 33.5
40 11.8
2 0.6
2 0.6
10 2.9
9 2.6
1 0.3
12
1 Z:i
2 0.6
13 3.8
:
0.3 1.2
4 1.2
2 0.6
6 1.8
5 1.5
22 6.5
9 2.6
8 2.4
340 100
Table 5. Isolates of E. co& S. Evphi, S. $~rat#i A, S. $arat&&hi B, and other bacteria obtained from the 1,000 bile specimen tested, bv subiects’ sex and aae.
No. of Specimens from males, by subjects’ age (in years)
specimens ~ Specimens from females, by subjects’ age (in years) All
examined <25 25-34 35-44 45-54 255 Total <25 25-34 35-44 45-54 255 Total specimens
md res,&s ___ ~ ~ ~ ___ ___ - ___ ___ ~ ___ ~
NO. % No. % No. % No. % No. % No. % No. % No. % No. % No. 96 No. % No. 56 No. %
Total specimens
obtained 14 100 37 100 44 100 42 100 67 100 204 100 144 100 185 100 195 100 116 100 156 100 796 100 1,000 100
Results negative 8 57.1 31 83.8 28 63.6 25 59.5 39 58.2 131 64.2 113 78.5 152 82.2 155 79.5 85 73.3 79 50.6 584 13.4 715 71.5
Results positive for:
E. coli 2 14.3 4 10.8 8 18.2 8 19.0 15 22.4 37 18.1 5 3.5 11 5.9 12 6.2 16 13.8 33 21.2 77 9.7 114 11.4
S. yphi 1 7.1 0 0.0 5 11.4 0 0.0 0 0.0 6 2.9 8 5.6 8 4.3 5 2.6 5 4.3 6 3.8 32 4.0 38 3.8
S. pmqphi A 1 7.1 0 0.0 0 0.0 1 2.4 0 0.0 2 1.0 0 0.0 2 1.1 0 0.0 0 0.0 1 0.6 30.4 5 0.5
S. pnra~phi B 0 0.0 1 2.7 1 2.3 2 4.8 1 1.5 5 2.5 8 5.6 3 1.6 4 2.1 4 3.4 6 3.8 25 3.1 30 3.0
Ristori et al. l SALMONELLA TYPHI-PARATYPHI CARRIER STATE 167
Table 6. Observed effect of time elapsed between bile specimen procurement and culturing upon rates of bacterial isolation.
Time elapsed between end of operation and inoculation of culture
Bacteriologic results
172 hours
No. of
specimens %
~-72 hours
No. of
specimens % Elapsed time not known specimens AU
Results negative
Results positive for: S. typhi-paratyphi group Other bacteria
Total no. of specimens
487 69.6 127 76.0 91 715
55 7.7 11 6.6 7 73
162 22.7 29 17.4 21 212
714 100.0 167 100.0 119 1,000
Overall, the rate of S. typhi-@aralyphi isolation per cent of those negative for 0 antibody pro- seemed less affected by the time lag than was vided bile specimens positive for S. typhi. Con- the rate of all bacterial isolations, the isolation versely, only 181 (19.9 per cent) of the test rate dropping from 7.7 to 6.6 per cent for subjects providing specimens negative for S. specimens yielding S. typhi-paratyphi, while typhi tested positively for H antibody, and dropping from 22.7 to 17.4 per cent for speci- only 122 (13.4 per cent) tested positively for 0
mens yielding other kinds of bacteria. antibody.
Table 7 compares the bile culture isolation results with results of the Widal tests per- formed with the patients’ blood specimens. As may be seen, the percentages of specimens yielding S. &phi isolates increased as the Widal “H” and “0” antibody titers rose. Overall, only 1.6 per cent of the subjects negative for H antibody (yielding titers below 1:40) and 1.7
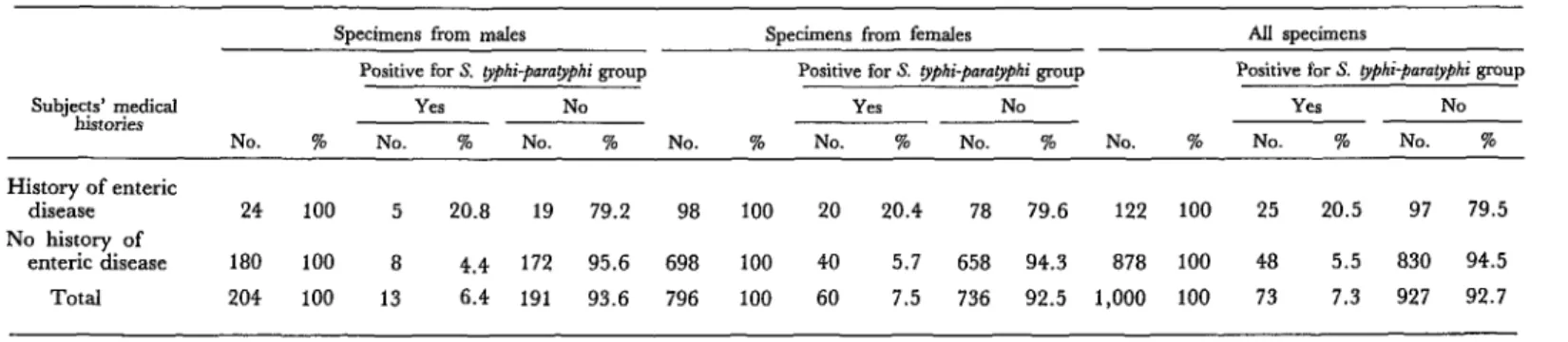
Table 8 compares the test subjects’ medical histories of enteric infection with the bile spec- imen culture results. Among the males, 20.8 per cent of those with a history of enteric dis- ease provided specimens yielding S. gphi or S. paraophi isolates, whily only 4.4 per cent of those without such a history yielded specimens positive for bacteria of either type. Similarly,
Table 7. A comparison of subjects yielding positive Widal test results (titers of 1:40 or more) for H and 0 antibody and subjects providing bile specimens positive for S. ~$hi.
Wiaizl titers obtained with H antigen:
S 1:20 1:40 or 1:80 2 1:160
Widal titers obtained with 0 antigen:
51:20 1:40 or 1:80 >1:160
No. of subjects tested
No. of subjects not tested
Bile specimen bacteriologic results
Positive for S. fyphi Negative for S. typhi
NO. % NO. %
Total specimens
NO. %
12 1.6 728 98.4 740 100
15 8.3 166 91.7 181 100
8 34.8 15 65.2 23 100
14 1.7 787 98.3 801 100
15 11.4 117 88.6 132 100
6 54.5 5 45.5 11 100
35 909 944
3 53 56
Table 8. A comparison of bile specimen results and subjects with a medical history of enteric disease.
Subjects’ medical histories
History of enteric disease
No history of enteric disease
Total
Specimens from m&s Specimens fmm females All specimens
Positive for S. pphi-parat@hyphi group Positive for S. typhi-para~~hyphi group Positive for S. #hi-parotypki group
Yes NO Yes NO Yes NO
No. % No. % No. % No. % No. % No. % No. % No. 7% No. %
24 100 5 20.8 19 79.2 98 100 20 20.4 78 79.6 122 100 25 20.5 97 79.5
180 100 8 4.4 172 95.6 698 100 40 5.7 658 94.3 878 100 48 5.5 830 94.5
Ristori et al. l SALMONELLA TYPHI-PARATYPHI CARRIER STATE 169
20.4 per cent of the women with a history of enteric disease (as compared to 5.7 per cent without such history) yielded specimens posi- tive for these organisms. Naturally, these his- tories of past infection were clearer in cases where the infection was relatively recent. Overall, it seems reasonable to assume that the correlation between a history of enteric in- fection and isolation of S. typhi or S. pamtyphi would have been more conclusive but for the aforementioned high incidence of subclinical or ambulatory cases in which the infection was not evident.
Discussion and Conclusions
A number of points regarding S. #hi in Chile appear to deserve mention. To begin with, the annual incidence of typhoid fever in Chile is greater than that observed in many poorer countries with climates more propi- tious for disease transmission. Furthermore, the disease is especially common in the city of Santiago, which has only a third of the na- tional population but roughly two-thirds of the typhoid cases.
It is known that S. typhi carriers play a larger role in typhoid fever transmission than do people with disease symptoms; but the studies demonstrating this have invariably relied on coproculture, an imprecise method that tends to be resisted by test subjects if serially repeated.
At the same time, there is evidence that members of the S. typhi-paratyphi group cause gallbladder disease, and also that if they infect people already suffering from gallbladder problems the carrier state will tend to occur more frequently and to be more prolonged than in people without gallbladder problems. In this vein, it should be noted that the preva- lence of gallbladder disease in Chile is one of the highest in the world.
Another significant point is that approxi- mately four times more cholecystectomies were performed on women than on men dur- ing the study period. However, men given the
serious and acute conditions, while a relatively larger share of women given the operation were suffering from gallstones or chronic cholecystitis.
Regarding the results of our bile cultures, 2 1.5 per cent of the bacterial isolates obtained were members of the S. typhi-paratyphi group. This percentage exceeded the isolation rate of any single bacteria except E. coli (which ac- counted for 33.5 per cent of the isolates), and also exceeded the magnitude of anything pre- viously reported in the literature. However, it should be noted that previous reports on this subject have come from countries with higher levels of economic development and lower in- cidences of enteric disease. Further surveys of the kind reported here in countries where typhoid fever remains a serious problem would provide a better basis for assessing the validity of the conclusions indicated by our work.
No clear correlation was observed between isolation of any specific bacteria from the bile culture and a record of past disease, except in cases of very recent infections. This finding can be attributed mainly to the frequency of ambulatory and inapparent infections, espe- cially with S. paratyphi B, an organism isolated from the bile cultures almost as often as S. @hi but one producing infections that were not often clinically diagnosed.
There was a fair degree of correlation be- tween positive bile culture results and the H and 0 antibody titers detected by the Widal agglutination tests.
Overall, applying the positivity rate for the S. typhi-paratyphi group that we obtained from bile cultures (7.3 per cent) to the total esti- mated number of gallbladder pathologies in metropolitan Santiago (500,000) or the entire country (1,200,OOO) suggests the presence of a vast number of ambulatory carriers-especial- ly in the female population that bears the major responsibility for food preparation.
170 PAHO BULLETIN l Vol. 16, no. 2, 1982
chronic carriers is increased by the high pre- vailing rates of gallstones and gallbladder pathologies. Indeed, there is good reason to suggest that this high prevalence of gallbladder pathologies can account for the unusually high frequency of S. @hi and S. parapphi infections in a country where the socioeconomic, sanita- ry, and climatic conditions would seem less than ideally suited to transmission of these
organisms. It would also appear that the chances of sharply reducing this problem depend upon the degree of success achieved in testing new live and attenuated oral vaccines that besides protecting against clinical mani- festations can produce intestinal immunity and a consequent reduction in the number of disease carriers.
ACKNOWLEDGMENTS
This study was carried out with the cooper- of the Santiago health services. The authors ation of the surgical departments of the San also gratefully acknowledge the cooperation
J uan de Dios, Salvador, Barros Luco- received from Drs. Jorge Toro, Mario Reyes,
Trudeau, Sotero de1 Rio, San Jose, and J. J. and Catterina Ferreccio, and from technicians Aguirre Hospitals of Santiago, the city’s Cen- Luz Zapata and Aurora Maldonado of the tral Emergency Clinic, andthe epidemiologists Institute of Public Health.
SUMMARY
Chile has experienced relatively high typhoid morbidity in recent years, the annual incidence going as high as 120 cases per 100,000 inhabitants. Because correlations had been found elsewhere be- tween gallbladder disease and the carrier state responsible for much typhoid transmission, a study was made of bile and blood specimens from 1,000 patients whose gallbladders were surgically re- moved in July-October 1980. The seven health facilities providing these specimens were located in metropolitan Santiago, which had been experienc- ing a considerably higher typhoid incidence than the rest of the country.
About four times as many surgical interventions were performed on women than on men, contirm- ing that there was a generally higher incidence of gallbladder disease among the former. However, a higher proportion of the male patients were admit- ted for acute vesicular disease.
Bile specimens yielding bacterial isolates were obtained from 35.8 per cent of the male patients and 28.5 per cent of the female patients. These 285 positive specimens yielded 38 Salmonella typhi and 35 S. pamgphi isolates. Overall, S. typhi was isolated from 11.2 per cent of the positive bile specimens and 3.8 per cent of the 1,000 specimens examined. These results correlated fairly well with the results of Widal agglutination tests performed with blood specimens from the same patients.
Gallbladder pathologies are quite common in Chile, there being an estimated 500,000 cases in Santiago alone. This fact, together with the fre- quent occurrence of the carrier state in gallbladder disease cases-as shown by the findings of this study-helps to explain the high observed incidence of typhoid fever.
REFERENCES
(1) Ministerio de Sahrd, Departamento de Plani- (2) Romero, H., et al. Aporte a la epidemiologfa iicacion. Anuurios estadisticos de1 Minkterio de Salud: de la iiebre tifoidea. Rev&a Chilena de Higieney Me- Enfermedades de not$icaci& obligatoria. Anuario 1980. dicina Preventiva 13:65-77, 1951.
Ristori et al. l SALMONELLA TYPHI-PARATYPHI CARRIER STATE 171
tual de la epidemiologfa de la fiebre tifoidea en la Provincia de Santiago. Rev&a Chilena de Higiene y Medicina Preventiva 15(3-4):53-67, 1953.
(4) Lobos, H., J. Garcia, C. Aguilar, E. Greve, M. Olivares, R. Bustos, M. E. Valenzuela, L. Zapata, and H. Romero. Estudio bacteriolbgico comparative de lechugas (lactuca sativa) provenien- tes de 10s alrededores de Santiago y region costera. Boletin de1 I&it&o Bacten’olbgico de Chile 18~33-37, 1976.
(5) Armijo, R., A. Pizzi, and H. Lobos. Preva- lencia de portadores tificos despuis de1 tratamiento con cloramphenicol. Bol Of Sanit Panam 62:295-302, 1967.
(6) Ames, W. R., and M. Robins. Age and sex as factors in the development of the typhoid carrier state, and a method for estimating carrier preva- lence. Am J Public Health 33:221-230, 1943.
(7) Brett, M., and D.J.P. Barker. The world distribution of gallstones. Int J Epidemiol5(4):335- 341, 1976.
(8) Marinovic, I., Cl. Guerra, and G. Larach. Incidencia de litiasis biliar en material de autopsias y anahsis de composition de 10s &Iculos. Rev&a Mkdica de Chile 100:1320-1327, 1972.
(9) Medina, E., A. M. Kaempffer, V. Croizet, M. Larrazabel, and M. Toporowicz. Epidemiolo- gfa de las colecistopatias en Chile: I. Volumen y caracterfsticas generales de1 problema; II. Factores de importancia en el estudio de autopsias. Revista Mkdica de Chile 100:1376-1389, 1972.
(10) Fukunaga, F. H. Gallbladder bacteriology, histology, and gallstones: Study ofunselected chole- cystectomy specimens in Honolulu. Arch Surg 106: 169-171, 1973.
(11) Puffer, R. R., and G. Griffith. Patterns of Urban Mortality. PAHO Scientific Publication 151. Pan American Health Organization, Washington, D.C., 1968.
(12) Goswitz, J. T. Bacteria and biliary tract disease. Am J Surg 128:644-645, 1974.
(13) Mason, G. R. Bacteriology and antibiotic selection in biliary tract surgery. Arch Surg 97:533- 537, 1968.
(14) Singh, Z., N. A. Wani, M. S. Misgar, and P. A. Rasnid. Evaluation of bacteria and biliary tract diseases. Inl Surg 62 (10):564-565, 1977.
(15) Magner, W., and J. M. Hutcheson. Chole- cystitis: A. Bacteriological and experimental study. Can Med Assoc J, November 1932, pp. 469-477.
(16) Martin, R., J. Bogart, and J. Heggers. An endogenous source for wound infections based on quantitative bacteriology of the biliary tract. Surgery 86(3):471-476, 1970.
(17) Delikaris, P. G., P. 0. Michail, G. D. Klonis, N. C. Haritopoulos, B. C. Golematis, and D. A. Dreiling. Biliary bacteriology based on intra- operative bile cultures. Am J Gastroenterol 68:51-55, 1977.