w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Review
article
Intravenous
ferric
carboxymaltose
for
the
treatment
of
iron
deficiency
anemia
João
Ricardo
Friedrisch
a,∗,
Rodolfo
Delfini
Canc¸ado
baHospitaldeClínicasdePortoAlegre(HCPA),PortoAlegre,RS,Brazil
bFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16July2014
Accepted14August2015
Availableonline14October2015
Keywords:
Anemia Iron-deficiency Therapeutics Anemia
a
b
s
t
r
a
c
t
Nutritionalirondeficiencyanemiaisthemostcommondeficiencydisorder,affectingmore
thantwobillionpeopleworldwide.Oralironsupplementation isusuallythefirstchoice
forthetreatmentofirondeficiencyanemia,butinmanyconditions,oralironislessthan
idealmainlybecauseofgastrointestinaladverseeventsandthelongcourseneededtotreat
thediseaseandreplenishbodyironstores.Intravenousironcompoundsconsistofaniron
oxyhydroxidecore,whichissurroundedbyacarbohydrateshellmadeofpolymerssuch
asdextran,sucroseorgluconate.Thefirstironproductforintravenoususewasthehigh
molecularweightirondextran.However,dextran-containingintravenousironpreparations
areassociatedwithanelevatedriskofanaphylacticreactions,whichmadephysicians
reluc-tanttouseintravenousironforthetreatmentofirondeficiencyanemiaovermanyyears.
Intravenousferriccarboxymaltoseisastablecomplexwiththeadvantageofbeing
non-dextran-containingandaverylowimmunogenicpotentialandthereforenotpredisposed
toanaphylacticreactions.Itspropertiespermittheadministrationoflargedoses(15mg/kg;
maximumof1000mg/infusion)inasingleandrapidsession(15-minuteinfusion)without
therequirementofatestdose.Thepurposeofthisreviewistodiscusssomepertinentissues
inrelationtothehistory,pharmacology,administration,efficacy,andsafetyprofileofferric
carboxymaltoseinthetreatmentofpatientswithirondeficiencyanemia.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published
byElsevierEditoraLtda.Allrightsreserved.
Introduction
Anemiaiscommon.Nutritionalirondeficiencyanemia(IDA)
is recognized as the most common nutritional deficiency
∗ Correspondingauthorat:Servic¸odeHematologiaClínicaeTransplantedeMedulaÓsseadoHospitaldeClínicasdePortoAlegre,Rua
RamiroBarcelos,2350,SantaCecília,90035-903PortoAlegre,RS,Brazil.
E-mailaddress:[email protected](J.R.Friedrisch).
disorderinboththedevelopedanddevelopingworld,affecting
morethantwobillionpeople.A2008WorldHealth
Organiza-tion(WHO)report,concentratingonpre-schoolchildrenand
women, estimatedthatworldwideoneinfourpeople were
affected by IDA, with pregnant women and preschool-age
http://dx.doi.org/10.1016/j.bjhh.2015.08.012
1516-8484/©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Allrights
Table1–Disadvantagesoforalirontherapy.
Gastrointestinaladverseevents Lackofadherencetotherapy Insufficientlengthoftherapy
Limitedduodenalabsorptionduetoconcomitantgastrointestinal pathology(inflammatoryboweldiseaseoranyothercauseof chronicinflammation,malignancy)
Longcoursetherapy–1to2monthstoresolveanemiaand3to6 monthstoreplenishbodyironstores
childrenatthegreatestrisk.1Highprevalencesofanemiaare
associatedwitholderage,2andwithacuteandchronic
condi-tions,suchaschronickidneydisease.3
Inapopulation-basedstudydesignedtodetectthe
preva-lenceofanemiainahealthypopulationofchildren(18months
to7years)andwomen(14–30years)testedin2006–2007inthe
stateofRioGrandedoSul,Brazil,themedianprevalenceof
anemiawas45.4%in2198childrenand36.4%in1999women.4
ThehighprevalenceofIDAhassubstantialconsequencesnot
onlyonhealthbutalsoonsubsequentsocioeconomicissues,
includingdecreasedworkcapacityandproductivity.1
Oral
iron
therapy
Ironhasbeenusedtotreatanemiaformorethan300years.
However, it was not until the 19th century when Pierre
Blaudintroducedferroussulfatethatirontherapybecamethe
standardtreatmentforIDA.4
Treatmentwithoralironsupplementsissimple,
inexpen-siveandarelatively effectivewayoftreating irondeficient
conditions.If responsedoesnotoccur within3–4weeksof
suitabletreatment,thereisnoreasontocontinueoraliron
therapy.Rather,anexplanationforfailureshouldbesought.
Ontheotherhand,itisverywellknownthatoralironisaless
thanidealtreatment.Table1showsthemaindisadvantages
ofthistherapy.
Noncompliancewith aprescribed courseof oraliron is
common,andevenincompliantpatients,limitedintestinal
absorptionfailstocompensatefortheironneedsinthe
pres-enceofongoingbloodlossesorinflammatoryconditions.5–7
Inaddition,adequateironstoresareessentialtoachieve
maximum benefit from erythropoiesis-stimulating agents
(ESAs).Lowironstoresanddecreasedavailabilityofironare
themostcommonreasonsforresistancetotheeffectofthese
agents.Thus,oralirontherapyshouldnotbeconsideredfor
chronickidneydisease (CKD)patientsonhemodialysisand
cancerpatientsreceivingESAsbecauseoftheinflammatory
state.Inthisscenario,oralironispoorlyabsorbedfromthe
intestinaltract duetothe upregulationofhepcidin,a
pep-tidehormonethatplaysacentralroleinironhomeostasis.8
Inaddition, ininflammatoryboweldisease(IBD),the
possi-bilitythat iron may furtherdamage the intestinal mucosa
shouldpromptseriousthoughtabouttheuseofintravenous
(IV)ratherthanoralirontherapy.9–14
Intravenous
iron
therapy
Treatment with IV iron in some clinical situations could
presentsomeadvantagesoveroraliron,suchasfasterand
Table2–Clinicalindicationsforintravenousiron therapy.
Post-gastrectomy/bariatricsurgery Anemiaofchronickidneydisease Intestinalmalabsorptionsyndromes Anemiaassociatedtoinflammatorydiseases Inflammatoryboweldiseases
Anemiaofcancer
Intolerancetooralironornon-compliancetoanoralregimen Iron-refractoryirondeficiencyanemias
Hereditaryhemorrhagictelangiectasias(Osler-Weber-Rendu disease)andangiodysplasiaduetoothercauses(incaseswhen oralironisnottoleratedorinsufficientfortreatment)
higher increases of hemoglobin (Hb) levels and body iron stores.15–23
For these reasons, modern formulations of IV iron
have emerged as a safe and effective alternative for IDA
management.9–14 The main clinical indications forIV iron
treatmentarelistedinTable2.
Newer
intravenous
iron
formulations
Inthelasttwoyears,threenewIVironcompoundshavebeen
releasedforclinicaluseinpatientswithIDA.Twoarecurrently
approvedforuseinEurope(ferriccarboxymaltose[FCM],24–29
andironisomaltoside1000[Monofer®]30andoneintheUnited
States(Ferumoxytol[FeraHeme®]).31–33
Intheirpre-registrationtrials,allofthesethreenew
com-pounds could potentially have a better safety profilethan
the more traditional IV preparations, particularly because
these products can be given more rapidly and in larger
doses than their predecessors.They are promisingfor the
complete replacementofironwithin15–60min.Theuseof
FCMinBrazilwasrecentlyapprovedbytheBrazilianHealth
Regulatory Agency, Agência Nacional de Vigilância Sanitária
(ANVISA).
Ferric
carboxymaltose
FCMisaparenteralirondextran-freeproductandthefirstof
thenewagentsapprovedforrapidandhigh-dose
replenish-mentofdepletedironstores.24FCMisanironcomplexthat
consistsofaferrichydroxidecorestabilizedbyacarbohydrate
shell.Thedesignofthemacromolecularferrichydroxide
car-bohydratecomplexallowscontrolleddeliveryofirontothe
cellsofthereticuloendothelialsystemandsubsequent
deliv-erytotheiron-bindingproteins,ferritinandtransferrin,with
minimalriskoflargeamountsofionicironbeingreleasedinto
theserum.24
FCM is a stable complex with the advantage of being
non-dextran-containingandhavingaverylowimmunogenic
potentialandthereforenotpredisposedtohighriskof
ana-phylacticreactions.Itspropertiespermittheadministration
oflargedoses (15mg/kg;maximum of1000mg/infusion) in
asingleand rapidsession(15-minuteinfusion) withoutthe
Efficacy
of
ferric
carboxymaltose
ThetherapeuticefficacyofIVFCMhasbeenevaluatedin
sev-eralrandomized,PhaseIII,open-label,controlled,multicenter
trialsinadiverserangeofconditionsassociatedwithabsolute
orfunctionalirondeficiencywithorwithoutanemia.These
conditionsincludepatientswithIBD,abnormaluterine
bleed-ing(AUB),postpartumIDA,chronicheartfailure(CHF),anemia
inpregnancyinthesecondandthirdtrimester,post-partum
anemia(PPA)andCKDpatientsonhemodialysisornot.Most
ofthesetrialsusedoralironasacomparator,andFCMwas
showntohavebetterefficacycomparedtooralironinterms
ofimprovementofHblevelsparticularlywithregardtobody
ironreplenishment(significantlyfasterandgreaterwithFCM
thanferroussulfate).3,24–28,34
Inmostofthesetrials,patientsreceivedeitherFCMdoses
of≤1000mg,administeredIVover≤15minororalferrous
sul-fate(FeSulf),325mg(65mgiron)threetimesdaily,or304mg
(100mgiron)twicedaily.3,24–28,34
FCMwas usuallyadministered untilthe patient’s
calcu-lated totalironreplacementdose was achieved.Treatment
withFCMimprovedindicesofanemia:Hb,ferritinand
trans-ferrinsaturation[TSAT]values.34
In patients on hemodialysis (HD) with IDA secondary
toCKD, FCMdemonstrated anefficacy comparableto iron
sucrose(IS)inachievinganincreaseinHb.34,35
InpatientswithIBDorPPA,improvementsinHblevelswere
morerapidwithFCMthanwithFeSulf.25,34,36
PatientswithPPAreceivingFCM,comparedtothose
receiv-ingoraliron,achieveda≥2.0g/dLincreaseinHbearlier(seven
daysversus14days;p-value<0.001)andweremorelikelyto
achievea≥3.0g/dLincreaseinHbatanytimebeginningon
Day 14(86.3% versus60.4%;p-value<0.001).Moreover they
weremorelikelytoachieveanHblevel>12.0g/dLbytheendof
thestudy(Day42;90.5%versus68.6%,p-value<0.01).Serum
ferritinincreasedintheIVFCMtreatmentgroup,butnotin
theoralirongroup.Differencesbetweengroupswere
signif-icantateachstudytimepoint.TSATincreasedsignificantly
at every time point in both groups; however, FCM-treated
patientsshowedhigherTSATateachtimepointafterthefirst
week.34,36
FCMimprovedthequalityoflifeofpatientstoanextent
equivalent to oral FeSulf in patients with IBD or PPA,
and to a greater extent than oral FeSulf in women with
AUB.25,27,34,36
FCMalsoimprovedthequalityoflifeaswellasfunctional
symptomsandexercisecapacityinpatientswithCHF.26,34
A multicenter comparative study that compared the
efficacy of FCM versus IS for correcting preoperative
ane-miain patients undergoingmajor elective surgeryshowed
limitationsofIStoachievehigh-levelironrepletion
includ-ing the number and frequency of doses (maximum dose
500mg per week) and duration of administration (60min
for a 200mgdose). In contrast, FCM attained iron
replen-ishment more frequently (82% versus 62%, respectively;
p-value=0.007) with fewer treatment sessions [2 versus 5,
respectively;p-value=0.001],showedahigherfinalHblevel
withatrendtowardahigherrateofanemiacorrection,and
patientsreceived intraoperativeand/or postoperativeblood
transfusionslessfrequently.TherewerenoIViron-related
life-threateningadverseevents,andthefrequencyofmildadverse
eventswassimilarwithbothIVproducts.37
Ferric
carboxymaltose
safety
The safety ofFCM was tested in a total of 20 phase II/III
databasetrialsthatevaluated5799subjectsexposedtoFCM,a
largerdatabasethanforanyotherIVironformulationreported
todate.38
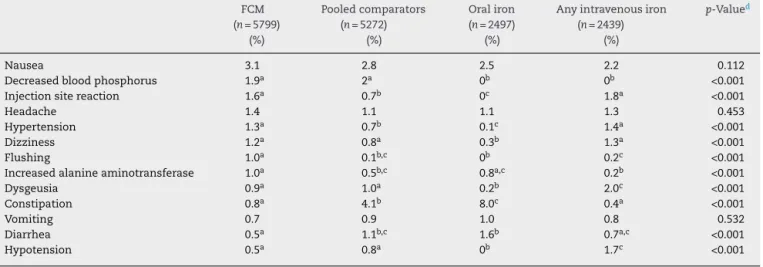
In this larger database the event rates are compared
betweensubjectsexposedtoFCMandsubjectsexposedtooral
iron,anyIViron,orpooledcomparators(includinganyIViron
formulationavailableatthetimethetrialswereconducted,i.e.
IS,ferricgluconate,orlowandhighmolecularweightiron
dex-tran,ororalironaswellasaplacebo).38WhencomparingFCM
tootherIVironformulations,theratesofnausea,injectionsite
reactions(i.e.discoloration,extravasation,orpain),headache,
hypertension,dizziness,constipation,vomitinganddiarrhea
aresimilar.Theratesofdysgeusiaandhypotensionarelower
in the FCM groupcompared with the other IViron group.
However,the ratesofdecreasedblood phosphate, flushing,
andincreasedalanineaminotransferasearehigherintheFCM
groupthantheotherIVirongroup.Drug-relatedadverse
reac-tionsreportedbyatleast1%oftreatedpatientsareshownin
Table3.36
Injection site reactions (i.e.discoloration, extravasation,
pain)mayoccurwithanyIVironformulations.38Such
reac-tionswerereportedin1.6%ofsubjectsreceivingFCMinthe
pooledphaseII/IIIdatabasecomparedwith1.8%ofsubjects
receivinganyotherIViron(Table3).38Thesediscoloredregions
maybelonglasting(severalmonths)andcanbeacosmetic
concern.Ithasbeenfoundthattheincidenceofinjectionsite
discolorationafterFCMadministrationmaybegreatlyreduced
bythepracticeofflushingtheinfusioncatheterwithsaline
beforewithdrawingtheneedletoavoiddribblingofFCMinto
thesubcutaneoustissue.38
Hypersensitivityreactions,includingsomethatarefatal,
are adverseeventsthatoccurtosomeextentforallIViron
formulations.Sofar,asinglecaseoffatalityhasbeen
asso-ciatedwithFCM.39Standardwarningtextisrequiredbythe
FDAtobeincludedinallthe prescribinginformationofall
IV irons marketed in the USA, advising that patients may
presentwithshock,clinicallysignificanthypotension,lossof
consciousness,orcollapse.Thetextstatesthatitisnecessary
tomonitorpatientsforsignsandsymptomsof
hypersensitiv-ityduringandafterIVironadministrationforatleast30min
and untilclinicallystablefollowingcompletionofthe
infu-sion.Inaddition,itisstatedthatsuchagentsareadministered
onlywhen personneland therapies are immediately
avail-ableforthetreatmentofserioushypersensitivity reactions.
Similarly,theEuropeanMedicinesAgencyrecentlycompleted
areviewofpost-marketingsafety dataforIVirons
(includ-ing FCM)and concludedthat allIVironshavea smallrisk
ofcausingallergicreactionswhichcanbelifethreateningif
nottreatedpromptly.40InthetwoprimaryFCM750mgtrials,
serious anaphylactic/anaphylactoidreactionswere reported
in0.1%(2/1775)ofsubjectsreceivingFCMand0.1%(1/1783)of
Table3–Drug-relatedtreatment-emergentadverseevents(%)(≥1%intheferriccarboxymaltose(FCM)groupphaseII/III database).38
FCM (n=5799)
(%)
Pooledcomparators (n=5272)
(%)
Oraliron (n=2497)
(%)
Anyintravenousiron (n=2439)
(%)
p-Valued
Nausea 3.1 2.8 2.5 2.2 0.112
Decreasedbloodphosphorus 1.9a 2a 0b 0b <0.001
Injectionsitereaction 1.6a 0.7b 0c 1.8a <0.001
Headache 1.4 1.1 1.1 1.3 0.453
Hypertension 1.3a 0.7b 0.1c 1.4a <0.001
Dizziness 1.2a 0.8a 0.3b 1.3a <0.001
Flushing 1.0a 0.1b,c 0b 0.2c <0.001
Increasedalanineaminotransferase 1.0a 0.5b,c 0.8a,c 0.2b <0.001
Dysgeusia 0.9a 1.0a 0.2b 2.0c <0.001
Constipation 0.8a 4.1b 8.0c 0.4a <0.001
Vomiting 0.7 0.9 1.0 0.8 0.532
Diarrhea 0.5a 1.1b,c 1.6b 0.7a,c <0.001
Hypotension 0.5a 0.8a 0b 1.7c <0.001
a,b,cDifferentlettersrepresentstatisticaldifferences(p-value<0.05).
d Chi-squaretest.
MostofthehypertensiveeventsintheFCMgroupoccurred
duringthe observationperiodimmediately followingstudy
drugadministrationandmostofthemwereresolvedwithin
30min.TheFCMprescribinginformationrecommends
mon-itoring patients for signs and symptoms of hypertension
followingeachFCMadministration.38
Atransientdropinbloodphosphatewasafindinginthe
clinicaltrialsofFCM.Noneofthecasesofhypophosphatemia
inthesetrials was associatedwithserious adverse events.
Innearlyall casestherewasnoclinicalsignexceptforthe
lowlaboratoryvalue.36,38,39,41,42Hypophosphatemiaisrelated
toan increase infibroblast growth factor 23 (FGF23)
activ-ity,anosteocyte-derivedhormonethatregulatesphosphate
andvitaminDhomeostasis.ElevatedFGF23activityincreased
urinary excretion of phosphate, decreased calcitriol levels,
andincreasedparathyroidhormonelevels,causing(insome
patientstreatedwithFCM)transient,mostlyasymptomatic
hypophosphatemia.38,42
Regardingtolerabilityandthesafetyprofile,theclinical
tri-alswithFCMevaluated 5799subjectsexposed to FCMand
mostdrug-relatedadverseeventswereconsideredtransient
andmild tomoderateinintensity. Treatment wasnot
per-manentlydiscontinuedinanypatientduetoadverseevents.
ThesestudiesconcludedthatFCMiswelltoleratedandwitha
clinicallymanageablesafetyprofilewhenappropriatedosing,
correctscheduleofinfusionandmonitoringareused.3,24–28,34
No safety concerns have been identified in breastfed
infantsofmothersreceivingFCMandadministrationinthe
secondandthirdtrimesterofpregnancyissafeandeffective.43
Conclusions
Oralironsupplementsareaninexpensiveandeffectivewayof
treatingIDApatientsandtheiradministration,intheabsence
ofinflammationorsignificantongoingbloodloss,cancorrect
anemia,providedsignificantdosesofironcanbetolerated.
Insomeclinical situations,oralironisaless thanideal
treatment becauseofthe increasedrate ofgastrointestinal
adverse events,particularly when using ferrous iron
com-pounds,andthelong courseneededtoresolveanemiaand
toachievereplenishmentofbodyironstores.
In cases where oral iron is ineffective, associated with
adverseeventsorcannotbeused,IVironcompoundsare
treat-mentoptions.
FCMhasbeenavailableinEuropesinceitsapprovalin2007
andintheUSAsince2009;itiscurrentlymarketedinover50
countriesandrecentlybecameavailableinBrazil.
Since2007severaltrialshavebeencompleted,confirming
thesafetyandeffectivenessofFCMinthetreatmentofIDAin
avarietyofclinicalsettings.
FCMpermitsamuchhighersingledoseofIVirontobe
administeredoverashorterperiod.
AnotherindicationforFCMisanemiaassociatedtochronic
inflammation,whenelevatedlevelsofhepcidinmayinduce
proteolyticdegradationofferroportinmoleculesthatare
nec-essaryfortransportingironfromthegastrointestinaltractto
thecirculation.
TheabilitytotreatIDAthatisunresponsivetooralironina
broadrangeofpatientsinoneortworapidadministrationsis
likelytoincreasepatients’complianceandmayimprovethe
qualityoflifeandsignificantlyreducehealthcarecosts.
FCM representsan importantnewtherapeuticmodality
thatofferssignificantclinicalbenefit,andtherebycanreduce
morbidityandmortalityfrommanypathologicalconditions
associatedwithirondeficiency.
Overall, FCMisconsidered anewoptimaltreatmentfor
parenteralironadministration,providingaveryefficientand
convenientmeansofdeliveringironinpatientswithIDA.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. deBenoistB,McLeanE,EgliI,CogswellM.Worldwide prevalenceofanaemia1993–2005:WHOglobaldatabaseon anaemia.Geneva:WorldHealthOrganization;2008,41p.
2. GaskellH,DerryS,AndrewMooreR,McQuayHJ.Prevalenceof anaemiainolderpersons:systematicreview.BMCGeriatr. 2008;8:1.
3. NationalInstituteforHealthandClinicalExcellence.Clinical
guideline39:anaemiamanagementinpeoplewithchronic
kidneydisease(CKD)[Internet].UK:NationalInstitutefor
HealthandClinicalExcellence;2006.Availablefrom:
http://guidance.nice.org.uk/CG39[cited15.07.14].
4. SillaLM,ZelmanowiczA,MitoI,MichalowskiM,HellwingT, ShillingMA,etal.Highprevalenceofanemiainchildrenand adultwomeninanurbanpopulationinsouthernBrazil.PLOS ONE.2013;8(7):e68805.
5. BrugnaraC,BerisP.Irontherapy.In:BeaumontC,BerisP, BeuzardY,BrugnaraC,editors.Disordersoferythropoiesis, erythrocytesandironmetabolism.Paris:EuropeanSchoolof Haematology;2009.p.512–28.
6. GisbertJP,GomollonF.Commonmisconceptionsinthe diagnosisandmanagementofanemiaininflammatorybowel disease.AmJGastroenterol.2008;103(5):1299–307.
7. CookJD.Diagnosisandmanagementofiron-deficiency anaemia.BestPractResClinHaematol.2005;18(2):319–32.
8. CoyneDW,AuerbachM.Anemiamanagementinchronic kidneydisease:intravenousironstepsforward.AmJ Hematol.2010;85(5):311–2.
9. Mu ˜nozM,Gómez-RamírezS,García-ErceJA.Intravenousiron ininflammatoryBowelldisease.WorldJGastroenterol. 2009;15(37):4666–74.
10.ErichsenK,UlvikRJ,NysaeterG,JohansenJ,OstborgJ,Berstad A,etal.Oralferrousfumarateorintravenousironsucrosefor patientswithinflammatoryboweldisease.ScandJ
Gastroenterol.2005;40(9):1058–65.
11.GascheC,WaldhoerT,FeichtenschlagerT,MaleC,MayerA, MittermaierC,etal.Predictionofresponsetoironsucrosein inflammatoryboweldisease-associatedanemia.AmJ Gastroenterol.2001;96(8):2382–7.
12.GisbertJP,BermejoF,PajaresR,Perez-CalleJL,RodriguezM, AlgabaA,etal.Oralandintravenousirontreatmentin inflammatoryboweldisease:hematologicalresponseand qualityoflifeimprovement.InflammBowelDis.
2009;15(10):1485–91.
13.SchroderO,MickischO,SeidlerU,deWeerthA,DignassAU, HerfarthH,etal.Intravenousironsucroseversusoraliron supplementationforthetreatmentofirondeficiencyanemia inpatientswithinflammatoryboweldisease–arandomized, controlled,open-label,multicenterstudy.AmJGastroenterol. 2005;100(11):2503–9.
14.LindgrenS,WikmanO,BefritsR,BlomH,ErikssonA,Granno C.Intravenousironsucroseissuperiortooralironsulphate forcorrectinganaemiaandrestoringironstoresinIBD patients:arandomized,controlled,evaluator-blind, multicentrestudy.ScandJGastroenterol.2009;44(7):839–45.
15.TrainaF.Deficiênciadeferronopacientesubmetidoà ressecc¸ãogástricaouintestinal:prevalência,causas, repercussõesclínicas,abordagemdiagnósticaeprevenc¸ão. RevBrasHematolHemoter.2010;32:78–83.
16.Canc¸adoRD,LoboC,FriedrichJR.Tratamentodaanemia ferroprivacomferroporviaparenteral.RevBrasHematol Hemoter.2010;32:121–8.
17.Canc¸adoRD,BrasilSA,NoronhaTG,ChiattoneCS.Avaliac¸ão daeficáciadousointravenosodesacaratodehidróxidode ferroIIInotratamentodepacientesadultoscomanemia ferropriva.RevBrasHematolHemoter.2007;29(2):123–9.
18.Canc¸adoRD,BrasilSA,NoronhaTG,ChiattoneCS.Ouso intravenosodesacaratodehidróxidodeferroIIIempacientes comanemiaferropriva.RevAssocMedBras.2005;51(6):323–8.
19.FernandesN,AbritaRR,doCarmoWB,CarvalhoGH,SilvaJH, LopesTM,etal.Impactodotratamentointravenosocom sacaratodehidróxidodeferroIIInosmarcadoresséricosde deficiênciadeferroenahemoglobinaséricaempacientes comdoenc¸arenalcrônicapré-dialítica.JBrasNefrol. 2007;29(1):33–7.
20.Canc¸adoRD,Mu ˜nozM.Intravenousirontherapy:howfar havewecome?RevBrasHematolHemoter.2011;33(6):461–9.
21.AbensurH.Deficiênciadeferronadoenc¸arenalcrônica.Rev BrasHematolHemoter.2010;32Suppl.2:84–8.
22.BlascoPG,LevitesMR,MônacoC.Ferroendovenosomelhora sintomasdepacientescominsuficiênciacardíacaquetêm deficiência.DiagnTrat.2010;15(3):125–6.
23.FabronJúniorA.Ferroendovenosonotratamentodaanemia ferropriva:seguroeeficaz.RevBrasHematolHemoter. 2007;29(2):106–8.
24.Lyseng-WilliamsomKA,KeatingGM.Ferriccarboxymaltose:a reviewofitsuseiniron-deficiencyanaemia.Drugs.
2009;69(6):739–56.
25.KulniggS,StoinovS,SimanenkovV,DudarLV,KarnafelW, GarciaLC,etal.Anovelintravenousironformulationfor treatmentofanemiaininflammatoryboweldisease:the ferriccarboxymaltose(FERINJECT)randomizedcontrolled trial.AmJGastroenterol.2008;103(5):1182–92.
26.AnkerSD,CominColetJ,FilippatosG,WillenheimerR, DicksteinK,DrexlerH,etal.Ferriccarboxymaltosein patientswithheartfailureandirondeficiency.NEnglJMed. 2009;361(25):2436–48.
27.VanWyckDB,MangioneA,MorrisonJ,HadleyPE,JehleJA, GoodnoughLT.Large-doseintravenousferriccarboxymaltose injectionforirondeficiencyanemiainheavyuterine bleeding:arandomized,controlledtrial.Transfusion. 2009;49(12):2719–28.
28.CovicA,MircescuG.Thesafetyandefficacyofintravenous ironcarboxymaltoseinanaemicpatientsundergoing haemodialysis:amulti-centre,open-label,clinicalstudy. NephrolDialTransplant.2010;25(8):2722–30.
29.MacdougallL,ChappeliJ,ChaiMO.Ironsupplementation:
focusonferriccarboxymaltose[Internet].HospitalPharmacy
Europe;2010.Availablefrom:http://www.
hospitalpharmacyeurope.com/featured-articles/iron-supplementation-focus-ferric-carboxymaltose[cited 15.07.14].
30.JahnMR,AndreasenHB,FuttererS,NawrothT,Schunemann V,KolbU,etal.Acomparativestudyofthephysicochemical propertiesofironisomaltoside1000(Monofer),anew intravenousironpreparationanditsclinicalimplications.Eur JPharmBiopharm.2011;78(3):480–91.
31.SinghA,PatelT,HertelJ,BernardoM,KauszA,BrennerL. SafetyofferumoxytolinpatientswithanemiaandCKD.AmJ KidneyDis.2008;52(5):907–15.
32.ProvenzanoR,SchillerB,RaoM,CoyneD,BrennerL,Pereira BJ.Ferumoxytolasanintravenousironreplacementtherapy inhemodialysispatients.ClinJAmSocNephrol.
2009;4(2):386–93.
33.LuM,CohenMH,RievesD,PazdurR.FDAreviewof ferumoxytol(Feraheme)forthetreatmentofirondeficiency anemiainadultswithchronickidneydisease.AmJHematol. 2010;859(5):315–9.
34.BraileG.Efficacyandsafetyofferricarboximaltosein correctingirondeficiencyanemia:areviewofrandomized controlledtrialsacrossdifferentindications.
Arzneimittelforschung.2010;60(6a):386–98.
irondeficiencyanaemiainhaemodialysispatients.In:Poster presentedattheXLVERA-EDTACongress.2008(Poster MP375).
36.VanWyckDB,MartensMG,SeidMH,BakerJB,MangioneA. Intravenousferriccarboxymaltosecomparedwithoralironin thetreatmentofpostpartumanemia:arandomized
controlledtrial.ObstetGynecol.2007;1102(Pt1):267–78.
37.BisbeE,Garcia-ErceJA,Diez-LoboAI,MunozM.Amulticentre comparativestudyontheefficacyofintravenousferric carboxymaltoseandironsucroseforcorrectingpreoperative anaemiainpatientsundergoingmajorelectivesurgery.BrJ Anaesth.2011;107(3):477–8.
38.BregmanDB,GoodnoughLT.Experiencewithintravenous ferriccarboximaltoseinpatientswithirondeficiencyanemia. TherAdvHematol.2014;5(2):48–60.
39.USFoodandDrugAdministrationCenterforDrugEvaluation
andResearch[Internet].Availablefrom:http://www.
accessdata.fda.gov/drugsatfdadocs/nda/2013/ 203565Orig1s000MedR.pdf[cited15.07.14].
40.EuropeanMedicinesAgencyNewrecommendationsto
manageriskofallergicreactionswithintravenous
iron-containingmedicines[Internet].Availablefrom:
http://www.ema.europa.eu/docs/enGB/documentlibrary/ Pressrelease/2013/06/WC500144874.pdf[cited15.07.14]. 41.WolfM,KochTA,BregmanDB.Effectsofirondeficiency
anemiaanditstreatmentonfibroblastgrowthfactor23and phosphatehomeostasisinwomen.JBoneMinerRes. 2013;28(8):1793–803.
42.SchoutenBJ,HuntPJ,LiveseyJH,FramptonCM,SouleSG. FGF23elevationandhypophosphatemiaafterintravenous ironpolymaltose:aprospectivestudy.JClinEndocrinol Metab.2009;94(7):2332–7.