w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Review
article
Iron
deficiency
in
cancer
patients
Flávio
Augusto
Naoum
∗AcademiadeCiênciaeTecnologia,SãoJosédoRioPreto,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received13May2016 Accepted30May2016 Availableonline22June2016
Keywords: Cancer Anemia Irondeficiency Intravenousiron
a
b
s
t
r
a
c
t
Anemiaisafrequentcomplicationincancerpatients,bothatdiagnosisandduring treat-ment, with a multifactorial etiologyin mostcases.Irondeficiency is amongthe most commoncausesofanemiainthissettingandcandevelopinnearlyhalfofpatientswith solidtumorsandhematologicmalignancies.Surprisingly,thisfactisusuallyneglectedby theattending physicianina waythatproper andpromptinvestigationoftheiron sta-tus iseithernot performedorpostponed.Incancerpatients,functionaliron deficiency is thepredominantmechanism,inwhichironavailabilityis reducedduetodiseaseor thetherapy-relatedinflammatoryprocess.Hence,serumferritinisnotreliablein detec-tingirondeficiencyinthissetting,whereastransferrinsaturationseemsmoreappropriate forthispurpose.Besides,lackofbioavailableironcanbefurtherworsenedbytheuseof erythropoiesisstimulatingagentsthatincreaseironutilizationinthebonemarrow.Iron deficiencycancauseanemiaorworsenpre-existinganemia,leadingtoadeclinein perfor-mancestatusandadherencetotreatment,withpossibleimplicationsinclinicaloutcome. Duetoitsfrequencyandimportance,treatmentofthisconditionisalreadyrecommended inmanyspecialtyguidelinesandshouldbeperformedpreferablywithintravenousiron. Theevidencesregardingtheefficacyofthistreatmentaresolid,withresponsegainwhen combinedwitherythropoiesisstimulatingagentsandsignificantincrementsinhemoglobin asmonotherapy.Amongintravenousironformulations,slowreleasepreparationspresent morefavorablepharmacologicalcharacteristicsandefficacyincancerpatients.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Iron
deficiency
is
common
in
cancer
patients
Anemiaisafrequentcomplicationincancerpatients, both atdiagnosis andduringtreatment.Inthe EuropeanCancer AnaemiaSurvey(ECAS),39%ofpatientswereanemicatthe timeofenrollmentinthestudy,and67%hadanemiaduring
∗ Correspondingauthorat:AcademiadeCiênciaeTecnologia.RuaBonfáNatale1860,15020-130SãoJosédoRioPreto,SP,Brazil.Phone
(55)1732334490.
E-mailaddress:[email protected]
chemotherapy. The cause of anemia in these patients is multifactorial,and formany ofthemirondeficiency isthe dominantmechanism.1,2
Iron deficiency can beclassified as absolute,when iron reservesaredepleted,orfunctional,whenironreservesare normalorevenincreased.Thecommoneventinboth situa-tions isthereductionofironavailabilityforerythropoiesis,
http://dx.doi.org/10.1016/j.bjhh.2016.05.009
70%
All
Pancreas Colorectal Lung
GI/EsophagusGenitour inar
y Breast
Gynecological
Testicle Others
Lymphoma Leuk emia
Myeloma
Solid tumors
% ID % anemia
Hematologic malignancies
% of patients
60%
50%
40%
30%
20%
10%
0%
Figure1– Prevalenceofirondeficiencyanemia(ID)andanemiaindifferenttypesoftumors.GI:gastrointestinal.
leading to anemia. In absolute deficiency, for obvious rea-sons,thelackofironinreservesisthemaintriggeringevent of anemia. In the case offunctional iron deficiency (FID), although the reserves are satisfactory, the presence of an inflammatoryprocess causes the iron to become‘trapped’ inmacrophagesand enterocytes, limitingits availability to thebonemarrow,triggeringanemia.Asexpected,FIDisthe predominantmechanismofirondeficiencyassociatedwith cancer.TheprevalenceofFIDinoncologypatientsrangesfrom 29to46%,andofirondeficiencyassociatedtoanemiaranges from7to42%.Figure1showstheprevalenceofirondeficiency andanemiainvarioustypesofsolidtumorsandhematologic malignancies.3
Functional
iron
deficiency
is
the
predominant
mechanism
in
cancer
patients
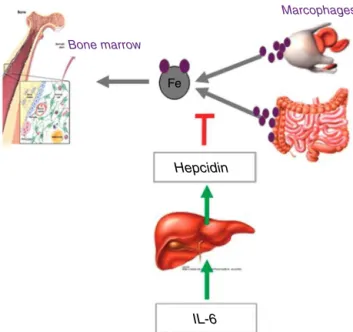
Thedemandforironbythebonemarrowandothertissuesis suppliedbythetransportofthiselementinthecirculationby transferrin.Theirontakenupbytransferrincancomefrom absorptionbyduodenalenterocytesorfromrecycling senes-centerythrocytesbymacrophages.Bothintestinalabsorption andmacrophagerelease ofironare controlledbyhepcidin, aregulatoryhormonesynthesizedbytheliver,which,under increasedconcentration,degradestheironexportprotein, fer-roportin,precludingtheavailabilityofironfortransportation fromtheselocations.4
Inthepresenceofaninflammatoryprocess,iron availabil-ityisreducedtoabout44%ofthenormal.5Thisisduetothe
releaseofinflammatorycytokines,particularlyinterleukin-6, whichactivatesthehepatichepcidintranscriptionpromoting genes,increasinghepcidinconcentrations,andpromotingthe blockageofironinputintothe circulationandreducing its availability(Figure2).6
Thus, even in the presence of adequate iron reserves, cancerpatientsmaydeveloplackofbioavailableiron, espe-cially when treated witherythropoiesis stimulating agents (ESAs)thatrapidlyincreasetheproductionofredbloodcells and the use ofiron.This isthe basicmechanism of func-tionalirondeficiency,theprevalenceofwhichincreasesinthe moreadvancedstagesofcancerandisassociatedwithpoor
performancestatus(TheEasternCooperativeOncologyGroup –ECOG).3
The
importance
of
correct
diagnosis
.
.
.
what
is
there
besides
ferritin?
Traditionally,serumferritinisthemostwidelyusedtestfor thediagnosisofirondeficiency,duetomirroringironreserves. However,becauseitisaproteinoftheacutephaseof inflam-mation,itsdiagnosticapplicabilityisconsiderablyimpairedin thepresenceofacuteorchronicinflammatoryprocesses.In thiscontext,transferrinsaturation(TS)becomesmorereliable fordiagnosticpurposes.7
Itisremarkablethat,intheclinicalpractice,onlyhalfof cancerpatientswithanemiaareinvestigatedastoironprofile andwhentheyare,theinvestigationbasicallyconsistsof fer-ritinmeasurements,whereastransferrinsaturationisrarely used.8Thisisavalidquestion,asamongcancerpatientswith
Bone marrow
Fe
Hepcidin
IL-6
Marcophages
Figure2–Pathophysiologyofanemiaassociatedwith
inflammatoryprocess,highlightingtheinhibitoryactionof
Iron deficiency in cancer patients
Transferrin saturation <20%
Anemia
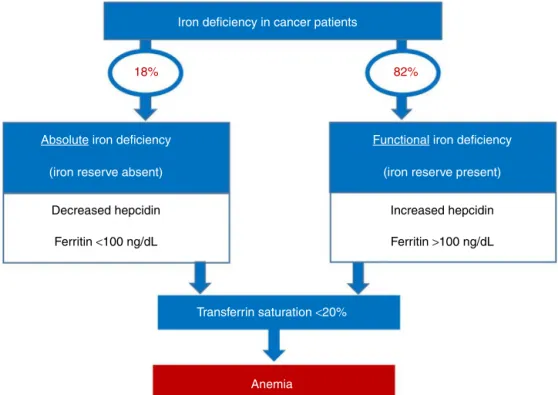
18% 82%
(iron reserve absent)
Decreased hepcidin
Ferritin <100 ng/dL
Absolute iron deficiency
(iron reserve present)
Increased hepcidin
Ferritin >100 ng/dL
Functional iron deficiency
Figure3–Laboratorycharacteristicsthatdifferentiateabsoluteandfunctionalirondeficiencyincancerpatients;thelatter
hasclearpredominanceinthispopulation.
reducedtransferrinsaturation,morethan80%havenormalor elevatedferritinvalues.3
Alsouseful,althoughlessavailableforthispurpose,arethe measurementsofreticulocytehemoglobincontent, determi-nationofthepercentageofhypochromicredbloodcellsinthe sample,solubletransferrinreceptor,amongothers.9
Figure3providesapracticalalgorithmfordifferentiation betweenabsoluteandfunctionalirondeficiency.
Clinical
impact
and
prognosis
of
iron
deficiency
in
cancer
patients
Theimmediatecomplicationsofirondeficiencyistheonsetor worseningofpre-existinganemia,withvaryingclinical reper-cussions, including worsening ofthe quality of lifeof the patients.Thisusuallyaffectsthepatients’performance sta-tus,withtheriskofjeopardizingtheiradherencetotreatment, andmayindirectlyaffecttherapeuticresults.3,10
The
treatment
of
iron
deficiency
in
cancer
patients
is
now
recommended
by
several
guidelines
Currently,thetreatmentofanemiaincancerpatientsbasically consistsofredbloodcelltransfusions,useofESAsandiron supplementation.Themaintherapeuticgoalistoimprovethe qualityoflife,inadditiontotryingtoreducethenumberof bloodtransfusions,whichareassociatedwiththeriskof trans-mittinginfections,hemolyticandnon-hemolytictransfusion reactions,alloimmunization,etc.7,11
Inthiscontext,theuseofESAsandironsupplementation are effective treatment options. However, the response to ESAs in patients undergoing chemotherapy and radiation therapyrangesfrom35to70%,andislimitedbyfactorssuch asirondeficiency,concomitantinfections,neoplasticactivity andpoorbonemarrowreserve.7,11Furthermore,somestudies
and meta-analyzes have raisedthe question of the riskof thromboembolic events with possible increases in mortal-ity associated to the use of ESAs, especiallywith off-label indicationsinpatientswhoarenotonchemotherapy.12
Forthesereasons,supplementationwithironstandsasan attractivetherapeuticoption, includedinseveralguidelines onthetreatmentofcancerpatientswithirondeficiency,either asmonotherapyinordertoimproveanemiaorinassociation withESAstoenhanceresponsetotheseagents(Table1).
Intravenous
iron
is
preferred
in
the
treatment
of
cancer
patients,
especially
formulations
with
slow
iron
release
There are several iron dosages and formulations available for treatment. In cancer patients, oral iron replacementis ineffectivebecauseintestinalironabsorptionisconsiderably reduced inthesepatients, withmorethan 95% ofthis ele-ment being excreted in the feces. Furthermore, the small amountofabsorbedironis‘locked’withintheenterocytesdue tometabolicdisordersinducedbythepreviouslymentioned inflammatorycytokines.Anotherfactorthatimpairsthe out-comeisthedecreasedadherencetooraltreatmentbecauseof thegastrointestinalsideeffects.7,16
100
Only ESAs ESAs + IV iron
Auerbach 200419 25 68 53 87 36 53 73 86 62 77 63 82 65 70 Hedenus
200722 2007Henry23 2008Bastit21 Pedrazzoli200824 Auerbach201020 Steensma201125
90 80 70 60 50 40 Response , % 30 20 10 0
Figure4–Increasesinhemoglobinobservedwitherythropoiesisstimulatingagents(ESAs)aloneandincombinationwith
intravenousiron(IV)incancerpatients.
ironisdirectlycapturedbymacrophages.Incaseoflessstable complexesofintravenousiron,suchassaccharateironand ferricgluconate,thecarbohydratecapsulethatcoatstheiron iseasilydegradedandtheironisquicklyreleased,requiring multiplelow-doseinfusions.However,withmorestable com-plexes,suchasferriccarboxymaltose(FCM),ironrelease is slowandprolonged,enablingtheadministrationofhighdoses ofironinasingleinfusion.Thus,1000mgofironcanbe admin-isteredinasingle15-mininfusionwithouttheriskofreleasing excessiveiron,particularlyasitsfreeortoxicforms.7,11,16,17
Table1–Recommendationsonmonitoringandiron
replacementincancerpatients.
Guidelines Recommendations
National Comprehensive CancerNetwork (NCCN)13
Monotherapywithiron(preferablyIV) isrecommendedforabsoluteiron deficiency(ferritin<30ng/mLandTS <20%)andinpatientsusingESAswith ferritinbetween30and800ng/mLand TSbetween20and50%.IVironcan reducethenumberoftransfusionsin patientswithfunctionaliron deficiency.
AmericanSocietyof ClinicalOncology (ASCO)andthe AmericanSocietyof Hematology(ASH)12
Ironprofilemonitoringis
recommended.Ironreplacementis recommendedifthereisiron deficiency,butthereisnotenough evidenceforgreaterdetailsregarding theformofreplacementand periodicityofmonitoring. EuropeanSocietyfor
MedicalOncology (ESMO)14
Ironprofilemonitoringis
recommended.IVironreplacementin patientswithirondeficiencyproduces incrementsinHbandreducesthe needfortransfusion.
EuropeanOrganization forResearchand TreatmentofCancer (EORTC)15
Ironreplacementshouldberestricted topatientswithabsoluteorfunctional irondeficiency.
IV: intravenous; TS:transferrin saturation;ESAs: erythropoiesis stimulatingagents;Hb:hemoglobin.
Thus,FCMisoneofthemostwidelyusedcompoundsin the treatmentofirondeficiencyincancerpatients,bothin associationwithESAsandasmonotherapy.
The main studies published so far, including a meta-analysis, favor the results of the association of ESAs and intravenousironratherthanESAalone,becauseofthesharp increaseinhematologicresponseevidencedbytheincrement in hemoglobin(Hb –Figure 4),fasterresponse time,better qualityoflife,reducedneedfortransfusionanddoseofESAs whenusedincombinationtherapy.18–25
Inadditiontoclinicalbenefits,thetreatmentof chemother-apyinducedanemiausingFCMwasshowntobemorecost effective,notablybyreducingtheuseanddoseofESAs.26
Regarding the use of intravenous iron as monotherapy, an observational study of 639 solid tumor and onco-hematological patients showed similar increments in Hb
levels with the use of FCM alone and FCM in
asso-ciation with ESAs (1.4g/dL and 1.6g/dL, respectively).27
Similarly, asingledoseof1000mgFCMinanemic patients (Hb 8.5–10.5g/dL, TS<20%, ferritin>40ng/mL in men and >30ng/mL in women) with low grade non-Hodgkin’s lym-phoma and priorchemotherapycomparedtonotreatment showedgreaterincreaseinHb(2.5vs.0.9g/dL).28
A cost minimization analysis of patients scheduled for surgeryforcolorectal cancer,demonstrated thatthe useof FCMbeforesurgeryreducesdirectandindirectcostsof hos-pitalizationcomparedtotheuseofsaccharateironandoral iron.29Thiscostsavingscanbeexplainedbythereducedneed
fortransfusionandhospitalizationtime;thepreoperativeuse ofFCMwasshowninanotherstudyofanemicpatientsina similarscenario.30
Conclusion
Thetreatment of irondeficiency in oncology isalready recommendedbyseveralspecialtyguidelinesandshouldbe carriedoutpreferablywithintravenousiron.Theevidences regardingtheefficacyofthistreatmentaresolid,withabetter responsewhencombinedwithESAandsignificantincrements inHbasmonotherapy.Amongtheavailableintravenousiron formulations,FCMpresentsmorefavorablepharmacological characteristicswithgoodefficacy inthisinflammatory sce-nario,inadditiontoamoreconvenientdosingregimenand goodcost-effectiveratio,asasmallernumberoftransfusions andlowerdosesofESAarerequired.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
Acknowledgement
IgratefullyacknowledgethefinancialsupportofTakedafor thetranslationofthismanuscript.
r
e
f
e
r
e
n
c
e
s
1. ParkS,JungCW,KimK,KimSJ,KimWS,JangJH.Iron deficienterythropoiesismightplaykeyroleindevelopment ofanemiaincancerpatients.Oncotarget.2015;6(40): 42803–12.
2. LudwigH,VanBelleS,Barrett-LeeP,BirgegårdG,Bokemeyer C,GascónP,etal.TheEuropeanCancerAnaemiaSurvey (ECAS):alarge,multinational,prospectivesurveydefiningthe prevalence,incidence,andtreatmentofanaemiaincancer patients.EurJCancer.2004;40(15):2293–306.
3. LudwigH,MüldürE,EndlerG,HüblW.Prevalenceofiron deficiencyacrossdifferenttumorsanditsassociationwith poorperformancestatus,diseasestatusandanemia.Ann Oncol.2013;24(7):1886–92.
4. WangJ,PantopoulosK.Regulationofcellulariron metabolism.BiochemJ.2011;434(3):365–81.
5. WeissG,GoodnoughLT.Anemiaofchronicdisease.NEnglJ Med.2005;352(10):1011–23.
6. GoodnoughLT,NemethE,GanzT.Detectionevaluation,and managementofiron-restrictederythropoiesis.Blood. 2010;116(23):4754–61.
7. LudwigH,EvstatievR,KornekG,AaproM,BauernhoferT, Buxhofer-AuschV,etal.Ironmetabolismandiron
supplementationincancerpatients.WienKlinWochenschr. 2015;127(23/24):907–19.
8. BeguinY,AaproM,BokemeyerC,GlaspyJ,HedenusM, LittlewoodTJ.Currentpracticeindiagnosisandtreatmentof chemotherapy-inducedanemiainfiveEuropeancountries–a patientrecordstudy.Blood.2010;116:1512[abstract].
9. NaoumFA.Doenc¸asquealteramosexameshematológicos. 1sted.SãoPaulo:Atheneu;2010.p.212.
10.CrawfordJ,CellaD,CleelandCS,CremieuxPY,DemetriGD, SarokhanBJ,etal.Relationshipbetweenchangesin hemoglobinlevelandqualityoflifeduringchemotherapyin anemiccancerpatientsreceivingepoetinalfatherapy. Cancer.2002;95(4):888–95.
11.AaproM,ÖsterborgA,GascónP,LudwigH,BeguinY. Prevalenceandmanagementofcancer-relatedanaemia,iron deficiencyandthespecificroleofi.v.iron.AnnOncol. 2012;23(8):1954–62.
12.RizzoJD,BrouwersM,HurleyP,SeidenfeldJ,ArcasoyMO, SpivakJL,etal.AmericanSocietyofHematology/American SocietyofClinicalOncologyclinicalpracticeguidelineupdate ontheuseofepoetinanddarbepoetininadultpatientswith cancer.Blood.2010;116(20):4045–59.
13.NCCN.Cancerandchemotherapy-inducedanemia,Version2; 2016.
14.SchrijversD,DeSamblanxH,RoilaF.
Erythropoiesis-stimulatingagentsinthetreatmentof anaemiaincancerpatients:ESMOClinicalPractice Guidelinesforuse.AnnOncol.2010;21Suppl.5: v244–7.
15.AaproMS,LinkH.September2007updateonEORTC guidelinesandanemiamanagementwith
erythropoiesis-stimulatingagents.Oncologist.2008;13Suppl. 3:33–6.
16.ToblliJE,AngerosaM.Optimizingirondeliveryinthe managementofanemia:patientconsiderationsandtherole offerriccarboxymaltose.DrugDesDevTher.2014;8: 2475–91.
17.GeisserP,BurckhardtS.Thepharmacokineticsand pharmacodynamicsofironpreparations.Pharmaceutics. 2011;3(1):12–33.
18.Gafter-GviliA,Rozen-ZviB,VidalL,LeiboviciL,Vansteenkiste J,GafterU,etal.Intravenousironsupplementationforthe treatmentofchemotherapy-inducedanaemia–systematic reviewandmeta-analysisofrandomisedcontrolledtrials. ActaOncol.2013;52(1):18–29.
19.AuerbachM,BallardH,TroutJR,McIlwainM,AckermanA, BahrainH,etal.Intravenousironoptimizestheresponseto recombinanthumanerythropoietinincancerpatientswith chemotherapy-relatedanemia:amulticenter,open-label, randomizedtrial.JClinOncol.2004;22(7):
1301–7.
20.AuerbachM,SilbersteinPT,WebbRT,AveryanovaS,Ciuleanu TE,ShaoJ,etal.Darbepoetinalfa300or500gonceevery3 weekswithorwithoutintravenousironinpatientswith chemotherapy-inducedanemia.AmJHematol. 2010;85(9):655–63.
21.BastitL,VandebroekA,AltintasS,GaedeB,PintérT,SutoTS, etal.Randomized,multicenter,controlledtrialcomparing theefficacyandsafetyofdarbepoetinalphaadministered every3weekswithorwithoutintravenousironinpatients withchemotherapy-inducedanemia.JClinOncol. 2008;26(10):1611–8.
22.HedenusM,BirgegårdG,NäsmanP,AhlbergL,KarlssonT, LauriB,etal.Additionofintravenousirontoepoetinbeta increaseshemoglobinresponseanddecreasesepoetindose requirementinanemicpatientswithlymphoproliferative malignancies:arandomizedmulticenterstudy.Leukemia. 2007;21(4):627–32.
23.HenryDH,DahlNV,AuerbachM,TchekmedyianS,Laufman LR.Intravenousferricgluconatesignificantlyimproves responsetoepoetinalfaversusoralironornoironinanemic patientswithcancerreceivingchemotherapy.Oncologist. 2007;12(2):231–42.
24.PedrazzoliP,FarrisA,DelPreteS,DelGaizoF,FerrariD, BianchessiC,etal.Randomizedtrialofintravenousiron supplementationinpatientswithchemotherapy-related anemiawithoutirondeficiencytreatedwithdarbepoetin alpha.JClinOncol.2008;26(10):1619–25.
25.SteensmaDP,SloanJA,DakhilSR,DaltonR,KahanicSP, PragerDJ,etal.PhaseIII,randomizedstudyoftheeffectsof parenteraliron,oraliron,ornoironsupplementationonthe erythropoieticresponsetodarbepoetinalfaforpatientswith chemotherapy-associatedanemia.JClinOncol.
2011;29(1):97–105.
anemiatreatmentthroughitsimpacton
erythropoiesis-stimulatingagentsandbloodtransfusion: Frenchhealthcarepayerperspective.JMedEcon. 2012;15(2):225–32.
27.SteinmetzT,TschechneB,HarlinO,KlementB,FranzemM, WamhoffJ,etal.Clinicalexperiencewithferric
carboxymaltoseinthetreatmentofcancerand chemotherapy-associatedanaemia.AnnOncol. 2013;24(2):475–82.
28.HedenusM,KarlssonT,LudwigH,FelderM,RoubertB, BirgegardG.Intravenousferriccarboxymaltoseassole anemiatherapyinpatientswithlymphoidmalignancies,
chemotherapy-inducedanemiaandfunctionaliron deficiency.Blood.2013;122(21):3439.
29.CalvetX,GenéE,ÀngelRuízM,FiguerolaA,VilloriaA,Cucala M,etal.Cost-minimizationanalysisfavoursintravenous ferriccarboxymaltoseoverferricsucroseororalironas preoperativetreatmentinpatientswithcoloncancerand irondeficiencyanaemia.TechnolHealthCare.2016;24(1): 111–20.