REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Validation
of
the
Brazilian
version
of
Behavioral
Pain
Scale
in
adult
sedated
and
mechanically
ventilated
patients
Isabela
Freire
Azevedo-Santos
a,
Iura
Gonzalez
Nogueira
Alves
a,
Manoel
Luiz
de
Cerqueira
Neto
b,
Daniel
Badauê-Passos
a,c,
Valter
Joviniano
Santana-Filho
a,b,c,
Josimari
Melo
de
Santana
a,b,c,∗aUniversidadeFederaldeSergipe(UFS),ProgramadePós-Graduac¸ãoemCiênciasdaSaúde,Aracaju,SE,Brazil
bUniversidadeFederaldeSergipe(UFS),DepartamentodeFisioterapia,Aracaju,SE,Brazil
cUniversidadeFederaldeSergipe(UFS),ProgramadePós-Graduac¸ãoemPsicologia,Aracaju,SE,Brazil
Received15October2015;accepted23November2015 Availableonline17May2016
KEYWORDS Validationstudies; Painmeasurement; Intensivecareunits; BehavioralPainScale; BrazilianBPS
Abstract
Backgroundandobjectives: The BehavioralPain Scaleisa pain assessmenttool for
uncom-municative andsedatedIntensive CareUnitpatients. The lackofaBrazilian scalefor pain assessmentinadultsmechanicallyventilatedjustifiestherelevanceofthisstudythataimedto validatetheBrazilianversionofBehavioralPainScaleaswellastocorrelateitsscoreswiththe recordsofphysiologicalparameters,sedationlevelandseverityofdisease.
Methods:Twenty-five Intensive Care Unit adult patients were included in this study. The
BrazilianBehavioralPainScaleversion(previouslytranslatedandculturallyadapted)andthe recordingofphysiologicalparameterswereperformedbytwoinvestigatorssimultaneously dur-ingrest,duringeyecleaning(non-painfulstimulus)andduringendotrachealsuctioning(painful stimulus).
Results:Highvaluesofresponsivenesscoefficient(coefficient=3.22)wereobserved.The
Cron-bach’salphaoftotalBehavioralPainScalescoreateyecleaningandendotrachealsuctioning was0.8.TheintraclasscorrelationcoefficientoftotalBehavioralPainScalescorewas≥0.8at eyecleaningandendotrachealsuctioning.TherewasasignificanthighestBehavioralPainScale score duringapplicationofpainfulprocedurewhencompared withrestperiod (p≤0.0001). However,nocorrelationswereobservedbetweenpainandhemodynamicparameters,sedation level,andseverityofdisease.
∗Correspondingauthor.
E-mail:[email protected](J.M.Santana). http://dx.doi.org/10.1016/j.bjane.2015.11.003
0104-0014/©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC
Conclusions:ThispioneervalidationstudyofBrazilianBehavioralPainScaleexhibits satisfac-toryindexofinternalconsistency,interraterreliability,responsivenessandvalidity.Therefore, theBrazilianBehavioralPainScaleversionwasconsideredavalidinstrumentforbeingusedin adultsedatedandmechanicallyventilatedpatientsinBrazil.
©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE Estudosdevalidac¸ão; Mensurac¸ãodador; Unidadesdeterapia intensiva;
EscaladeDor Comportamental; EDCbrasileira
Validac¸ãodaversãoBrasileiradaEscalaComportamentaldeDor(BehavioralPain Scale)emadultossedadosesobventilac¸ãomecânica
Resumo
Justificativaeobjetivos: AEscalaComportamentaldeDor(BehavioralPainScale)éuma
fer-ramenta de avaliac¸ão da dor para pacientes não-comunicativos e sedados em unidade de tratamentointensivo(UTI).Afaltadeumaescalabrasileiraparaaavaliac¸ãodadoremadultos sobventilac¸ãomecânicajustificaarelevânciadesteestudoqueteveporobjetivovalidara ver-sãobrasileiradaEscalaComportamentaldeDor(ECD),bemcomocorrelacionarseusescores comosregistrosdeparâmetrosfisiológicos,níveldesedac¸ãoegravidadedadoenc¸a.
Métodos: Vintee cinco pacientesadultos internados em UTI foram incluídos nesteestudo.
A versãobrasileira daECD(previamentetraduzida eadaptadaculturalmente)eosregistros dosparâmetrosfisiológicosforamrealizadossimultaneamentepordoisavaliadoresduranteo repouso, durantealimpeza dosolhos (estímulo não doloroso)e duranteaaspirac¸ão endo-traqueal(estímulodoloroso).
Resultados: Valores elevados do coeficiente de coeficiente de responsividade
(coefi-ciente=3,22)foramobservados.OcoeficientealfadeCronbachdoescoretotaldaECDdurante alimpezadosolhose aspirac¸ão endotraquealfoi de0,8.Ocoeficiente decorrelac¸ão intra-classedoescoretotaldaECDfoi≥0,8durantealimpezadosolhoseaspirac¸ãoendotraqueal. HouveumescoresignificativamentemaisaltonaECDduranteaaplicac¸ãodoestímulodoloroso emcomparac¸ãocomoperíododedescanso(p≤0,0001).Noentanto,nãoforamobservadas correlac¸õesentredoreparâmetroshemodinâmicos,níveldesedac¸ãoegravidadedadoenc¸a.
Conclusões:Esteestudopioneirodevalidac¸ãodaECDbrasileiraapresentaíndicessatisfatórios
deconsistênciainterna,confiabilidadeentreavaliadores,responsividadeevalidade.Portanto, aversãodaECDbrasileirafoiconsideradauminstrumentoválidoparaserusadoempacientes adultossedadoseventiladosmecanicamentenoBrasil.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Criticallyill patients frequently experience pain and dis-comfort during Intensive Care Unit (ICU) stay. ICUs are specialized centers where subjects are exposed to dif-ferent factors which causes acute pain including routine procedures,1---5 such as endotracheal suctioning, turning,
peripheralandcentralintravenouspuncturing.6Thus,pain
assessment and treatment in mechanically ventilated ICU patientshavebeenconsideredimportantandstudiedinlast twodecades.7
TheSocietyofIntensiveCareMedicinerecommendsthat painshouldberoutinelymonitoredinalladultICUpatients.8
Patient’sself-reportsofpain,physiologicalparametersand scalesbasedontypicalbehaviorsconstituteavailable meth-odsintheassessmentofpain.However,criticallyillpatients areoftenunabletoeffectivelycommunicateduetosevere illness,mechanicalventilation,administrationofsedatives
andanalgesicsoradecreasedlevelofconsciousness.4,9,10On
theotherhand,patientsmaybeevaluatedbyphysiological parameters and through the use of scales based on typi-calbehaviors. However,physiological parameters,suchas bloodpressure,heartrate,peripheraloxygensaturationand respiratoryrateappeartobelessvalidforpainassessment in ICU patients due to underlying disease and treatment withinotropes andvasopressor medicines.11---13 Therefore,
theSocietyofIntensiveCareMedicineadvisestheuseofpain assessmenttoolsthatfocusmainlyonbehavioralindicators ofpain.8
In this context, in order to quantify pain in mechani-cally ventilated patients, Behavioral Pain Scale (BPS) was firstlyvalidatedinEnglish.6TheBPSwastranslatedinfour
languages6,14---16andvalidatedjustintwoofthem.6,15Several
studieshaveshownthatBPSisreliableandresponsive.10,17---25
this topic. This occurs because the nonexistence of vali-datedscalesinBrazilianPortuguesetomeasurepaininICU patients.InBrazil,theBPSwasfirstlytranslatedtoBrazilian Portugueseinapreliminarystudyrecentlypublishedbyour group.26 Itwasappliedinmechanicallyventilatedpatients
showingtobeverypromisingasatoolformeasuringpain inBrazilianICUpatients.Thus,theimportanceofpain mea-surementinnon-verbalpatientshospitalizedinICUsandthe absenceofavalidatedBrazilianscaleforthispurpose high-lightstherelevance ofthisstudy.Taking intoaccountthe potentialoftheBPStomeasurepaininmechanically venti-latedpatients,26thisstudyaimedtoanalyzethereliability,
responsivenessandvalidityofthetranslatedBPStoBrazilian Portuguese.
Methods
Sample
Weperformedacross-sectionalstudywitharepeated mea-surementdesignin25sedatedandmechanicallyventilated subjects admitted at a cardiac ICU of a public hospital. Sample size was estimated based ona precision of Cron-bach␣as0.90±0.05 fora scale with3 subscalesasBPS.
Thus,aminimumof25subjectsshouldbeassessedinthis study.18 Allsubjectswerelegallyrepresentedbytheir
con-servators,whohavesignedthetermofconsent,oncethey wereunconsciousorinuseofsedativemedicines.The Fed-eralUniversityof Sergipeandhospitalethicalcommittees approvedthestudyprotocol.
Patients whowere sedated andunconscious, in use of mechanical ventilation and in the postoperative period (immediate or delayed) of Coronary Artery Bypass Graft (CABG) or Valve Surgery (VS) were included in our sam-ple. Exclusion criteria considered those with age less than 18 years old and/or with one of these conditions that could change behavioral expressions: quadriplegia, peripheral neuropathy, stiffness due to decortication or
decerebrationorinuseofneuromuscularblockersduringthe assessment.
Validationmethodologicalprocedures
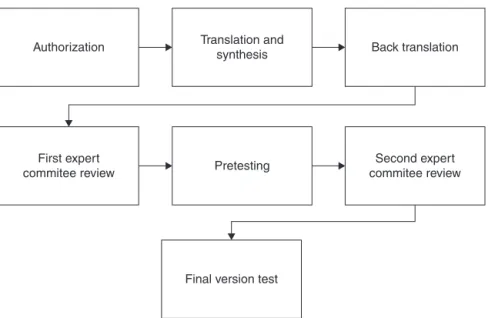
TheBrazilianversionofBPSwasdevelopedaftervalidation processbasedonpre-establishedprocedures27,28 asshown
inFig.1.
Thefirstfiveprocedures(fromauthorizationto pretest-ing)wereperformedinthepreliminarystudypublishedby ourgroup.26 Duetotheoccurrenceofdoubtsand
discrep-ancy among investigators regarding the adequacy of the meaningsof eachitemtoclinical practiceduring pretest-ing,asecondexpertcommitteereviewwasdone.Afterthis reviewandconsensus,the‘‘BrazilianBPSapplicationguide’’ wascreatedwithexplicationsandpracticeadequacyofthe sub-items(SeeSupplementalDigitalContent,whichisatext documentwithBrazilianBPSguide).
TrainingoftheICUstaff
For final version test phase, four professionals from the ICU staff (three physical therapists and one nurse) were recruitedandtrainedtoparticipateasinvestigatorsinthis study.TheyindividuallyreadBrazilianBPSapplicationguide beforedatacollectiontostandardizetheassessment. Expla-nationsfor any doubts were done toavoid biason items interpretation.
Each of these health professionals had specific activ-ities during the evaluation. The physical therapists were responsible for pain assessment (register of BPS scores simultaneously by two of them) and physiological param-eters recording (multimodal monitor observation), while the nurse performed the routine procedures (painful and non-painful).For reliabilitymeasurement, they couldnot keepanykindofcommunicationbetweenthemduringthis process.
Authorization
First expert
commitee review Pretesting
Final version test
Second expert commitee review Translation and
synthesis Back translation
Datacollection
Beforepainassessment,baselinedataasage,sex,clinical diagnoses,useofsedativeand/oranalgesicsandseverityof disease(APACHEIIscore)29 wasrecordedbasedonmedical
recordinformation.Patient’ssedationlevelwasassessedby usingboth Ramsay andRASSscales.30---32 These toolswere
chosen to establish the inability of subjects to verbalize causedbysedativedrugseffects.
Studyprocedures
Pain assessment withBrazilian BPSoccurred in three dif-ferent moments: at rest (stable subject in bed), during EyeCleaning(EC) withcottonsoaked in saline0.9% (non-painful procedure)24 and during Endotracheal Suctioning
(ETS) with the catheter insertion on the airway (painful procedure)24,26,33---35Inadditiontopainscores,hemodynamic
parameterswererecordedduringthethreephasesof evalu-ation.SystolicBloodPressure(SBP),DiastolicBloodPressure (DBP),MeanBloodPressure(MBP),HRandSpO2were mea-suredthroughnon-invasivemethods.
Statisticalanalysis
DatawereanalyzedwithSPSSStatisticsversion22.0(SPSS, Inc.,Chicago, IL) and Graph Pad Prism 5 (GraphPad Soft-ware,Inc.,LaJolla,CA).Baseline datawererepresented asmean±standarderrorof mean.t-TestandFisherexact testcomparedthetypeofsurgeryandpostoperativeperiod data.
Reliability, responsiveness and validity were the psy-chometric properties analyzed on Brazilian BPS version. InterraterreliabilityoftheBPSwastestedbythecalculation ofIntraclassCorrelationCoefficients(ICC)andinternal con-sistencywasassessedwithCronbach’scoefficient˛.These werecalculatedforBrazilianBPStotalscoresandforeach sub-itemduringECand TS.Valuesbetween 0.70and0.80 wereconsideredasacceptable,andvalues>0.8asgood.36,37
Responsiveness is the capacity to detect significant changesover time.Thiscoefficient wasobtainedby divid-ingthedifferencebetweenthemeanscoresoftheBrazilian BPSat restandduringpainfulproceduresbytheStandard Deviation(SD)ofthemeanscoresatrest.Acoefficientvalue higherthan0.8wasconsideredsatisfactory.38
The abilityofa scaletomeasurewhatit intends char-acterizes the instrument validity. It was established in threeways: construct, criterion and content. Pain scores were not normally distributed, and therefore, nonpara-metricstatisticaltestswereapplied.Spearmancorrelation wascalculatedtocompareBrazilianBPSscoresduringETS withphysiologicalparameters,Ramsay,RASSandAPACHEII scores(construct validity),whileFriedman’stest followed byDunnpost hoctest wasusedtoanalyzepainscore dif-ferencesovertheassessmentmoments(criterionvalidity). Semantic, idiomatic, conceptual and practical review of Brazilian BPS items by an expert committee at pre-test phaseand final version test consisted oncontent validity analysis.28
Hemodynamic data were normally distributed, thus to determine changesonphysiological parameters over time
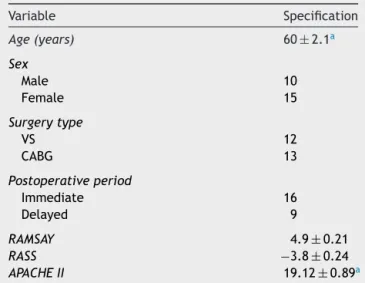
Table1 Demographicdata(n=25subjects).
Variable Specification
Age(years) 60±2.1a
Sex
Male 10
Female 15
Surgerytype
VS 12
CABG 13
Postoperativeperiod
Immediate 16
Delayed 9
RAMSAY 4.9±0.21
RASS −3.8±0.24
APACHEII 19.12±0.89a
VS,valvesurgery;CABG,coronaryarterybypassgraft;
Immedi-ate,1haftersurgery;Delayed,24haftersurgery.
a Datais represented as mean±standarderror of mean or
absolutefrequency,whenrelevant.
(at rest, duringEC andETS) onewayANOVAfor repeated measureswasperformed.Onlysubjectswithcomplete eval-uationrecordingsweresuitableforanalysis.Significancefor allstatisticaltestswassetatp≤0.05.
Results
Twenty-five patients were included in this sample study. Baselinedata(age,sex,surgerytype,postoperativeperiod, APACHEIIscore)arepresentedinTable1.
There was no significant difference between subjects undergone to VS or CABG in the immediate or delayed postoperativeperiod(p≥1.0).Similarly,itwasnotverified influenceofsurgerytypeandpostoperativeperiodon seda-tiveandseverityofdiseaseparameters(p≥0.05).Thus,the surgerytypeandpostoperativeperioddidnotinfluencethe results.
Allpatients weresedated incontinuousinfusion (mida-zolam and fentanyl)at the evaluation moment, one hour (immediateperiod)ormorethanforty-eighthours(delayed period,5±1.2days)aftersurgeryprocedure. Neuromuscu-lar blockersandanalgesic drugswerenotadministeredat the 8hourspreviously totheassessment, tonot interfere withthedatacollected.
Reliability
Considering the satisfactory established values for Cron-bach˛,36ahighrelationbetweenthescalesitems(internal consistency)occurredinECandETSprocedures(Cronbach ˛=0.8,each).
Table2 PhysiologicalvariablesatthethreeassessmentmomentswithBrazilianBehavioralPainScale.
Variable Rest Eyecleaning Endotrachealsuctioning p-Valuea
SBP(mmHg) 122.4±3.6 119.4±3.8 123.4±4.2 0.5 DBP(mmHg) 71.5±2.8 69.7±3.9 73.1±3.9 0.4 MBP(mmHg) 82.4±3.1 81.3±3.8 82.8±4.0 0.8 HR(bpm) 82.7±4.0 85.8±4.7 84.7±4.2 0.4 SpO2 97.4±0.3 96.3±0.8 97.2±0.3 0.2
SBP,systolicbloodpressure;DBP,diastolicbloodpressure;MBP,meanbloodpressure;HR,heartrate;SpO2,peripheraloxygensaturation.
Datawererepresentedasmean±standarderrorofmean.
a p≥0.05(onewayANOVAforrepeatedmeasures).
the investigators for facial expression items during these moments(ICC≥0.8).
Responsiveness
The coefficient calculated resulted in a good capacity to detectpainintensitychangesovertime.Thevalueobtained was3.22,consideredahigheffectforascale.38
Validity
ChangeinphysiologicalvariablesisshowninTable2.There wasnotasignificant increaseinallphysiological variables whenthesevalueswerecomparedatrest,ECandETS. Con-structvaliditywasevaluatedbycorrelationsbetweenpain scoresandphysiologicalparameters,sedationandseverity of disease levels.These correlations were non-significant (Table3).
Forcriterionvalidity,thecomparisonofpainscoresover timewasdone.Fig.2shows thatBrazilian BPSfinal score wassignificantlyhigherduringpainfulprocedure (TS)than atrest(p≤0.0001).
Table3 CorrelationbetweenBehavioralPainScalescores during painful procedures and physiological parameters, sedationandseverityofdiseaselevels.
Trachealsuctioning
BPSscore
CC p-Value
SBP 0.35 0.86
DBP −0.83 0.69
MBP −0.17 0.93
HR −0.30 0.89
SpO2 0.11 0.61
RAMSAY −0.34 0.10
RASS 0.32 0.12
APACHEII −0.03 0.89
CC,Spearmancorrelationcoefficient;SPB,systolicblood pres-sure;DBP,diastolicbloodpressure;MBP,meanbloodpressure; HR, heart rate; SpO2, peripheral oxygen saturation; RASS, RichmondSedation-Agitation Scale;APACHE, AcutePhysiology HealthChronicEvaluation.
10
***
5
Beha
vior
al pain score
0
Rest Eye cleaning ETS
Figure 2 Behavioral Pain Scale score changes over time: at rest, during eye cleaning and during endotracheal suc-tioning. Values were represented as median, 25th and 75th percentile.*p≤0.0001betweenrestandendotracheal suction-ing(Friedman’stestandDunnposthoctest).ETS,endotracheal suctioning.
Discussion
This pioneer validation study of Brazilian Behavioral Pain Scale exhibits satisfactory index of internal consistency, interrater reliability,responsiveness and validity. Further-more, non-significant correlations between pain intensity andphysiologicalparameters,sedationandseverityof dis-ease levels suggest that this pain assessment tool is a powerfulinstrumenttodetectpaininBrazilianICUpatients. Validityof BrazilianBPSwasdemonstratedbya signifi-cantincreaseofthescoresduringpainfulprocedure(ETS).It wasevidencedhigherpainintensityduringETScomparedto rest,whichprovestheinstrumentcapacitytodiscriminate pain.18 Thesechangesoverthethreeassessmenttimesisa
parameterthatindicatescriterionvalidityandwasusedon previousstudiesofthisscaleinotherlanguages.10,14,15,17---25,39
Theabilitytodetectimportantchangesonpainintensity overtimecorresponds toresponsiveness.This psychomet-rical property was considered excellent for Brazilian BPS version with high and representative coefficient for this sample.In thesame way,Aïssaoui etal.18 evidenced high
theobservationof non-significantincreasesof painscores measuredwithBPSduringcatheterdressingchange,6body
temperature measurement15 and eye care24,39 when
com-pared to rest. Contrarily, Rijkenberg et al.22 observed a
significantincreaseoftotalscorebetweenrestandthe non-painfulprocedure(oral care) aswell aspainfulprocedure (turning)inacriticallyillsubjects.22
The correlation of BPS scores with physiological data, sedation and severity of disease were not observed in the present study. Values of heart rate, blood pressure and saturation were not significantly higher during ETS as hypothesized. Oppositively, Payen et al.6 and Aïssaoui
etal.18 indicatedan increaseonbloodpressureandheart
rateduringpainfulprocedure.Farthertheseauthorsfound an inversely correlation between sedation level and pain scoresrecordedbytheoriginalBPSversion.Inthiscontext, Youngetal.24affirmedthatinadditiontosedativeand
anal-gesicdrugs,tracheostomyandsurgeryprocedureinfluenced onpainintensitymeasuredbyBPS.
Itis recommendedtorecord hemodynamic parameters onlyasacomplementforpainassessmentor when behav-ioralindicatorsarenotpresentonthebedside.11Thefailure
toprove criterion validityof these variables measured in ICUssustains thisrecommendation.12 Thus, inthe current
study was not observed a significant correlation between painscoreandvitalparametersprobablyduetothelower specificityofthesevariables.
ReliabilityresultswereconsideredsatisfactoryduringEC andETSasshowedinotherBPSvalidationstudies.6,15,18,20,24
HigherICCvalues(interraterreliability)wereobserved on thesub-item‘‘FacialExpression’’.The highestagreement between the investigators in this item may be linked to the familiarity for them to analyze facial changes (spe-cificmovements of the eyes,eyebrows,cheeks and lips), acommonactivity for humansubjects whoobservefacial expressions daily.40 Recently published evidence supports
thefindingsofourstudywhenaffirmsthatfacialexpressions areaccentuatedduringendotrachealsuctioning.19Eyebrows
raised, nose wrinkling and head turned right and up are movementsthat indicates painin non-verbally patients.19
Thisresultencouragesthefacialexpressionanalysisto quan-tifypain.
Therelevanceofthisstudyforclinicalpracticeconsists onthe applicability of a validated scale to measure pain inBrazilianICUs.Theease ofuse,lowcostandfeasibility inPortuguese cancontributetotheestablishment of pain assessmentandmanagementprotocolsbyICUprofessionals fromBrazil.
Insummary, thisstudyprovidesevidencethatBrazilian BPSpresentsgoodinterraterreliability,internalconsistency, validity and responsiveness. Non-significant correlation betweenBPSscoresandtheothervariablesreinforcestheno abilityofthevitalparameterstomeasurepain.Therefore, painassessmentandmanagementinBrazilianICUsis encour-aged,byusingvalidscales,improvingcriticallyillcareand consequentlypromotingphysicalandsocialwell-being.
Further studies involving different ICU samples are requiredtoprovereproducibilityofBrazilianBPS.Moreover, these studies can contribute to reinforce the importance ofadequateassessmentforagoodmanagementofpainby healthcareprofessionalsresponsibleforcriticallyilladults inBrazil.
Summary
Brazilian BPSpresents good interrater reliability, internal consistency,validityand responsiveness.It consistsin the firstvalidatedinstrumenttoassesspaininBrazilianICUs.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
AuthorsthankthesupportprovidedbyHospitaldeCirurgia (Aracaju,SE,Brazil)toperformthisstudy.
References
1.Arroyo-NovoaCM,Figueroa-RamosMI,PuntilloKA,etal.Pain related to tracheal suctioning in awake acutely and criti-callyill adults:adescriptive study.Intensive CritCareNurs. 2008;24:20---7.
2.GélinasC,HarelF,FillionL, etal. Sensitivityand specificity ofthecritical-carepainobservationtoolforthedetectionof paininintubatedadultsaftercardiacsurgery.JPainSymptom Manage.2009;37:58---67.
3.Puntillo KA, Morris AB, Thompson CL, et al. Pain behaviors observedduringsixcommonprocedures:resultsfromThunder ProjectII.CritCareMed.2004;32:421---7.
4.Puntillo KA,Pasero C,Li D,et al. Evaluationof painin ICU patients.Chest.2009;135:1069---74.
5.PuntilloKA,MaxA,TimsitJF,etal.Determinantsofprocedural painintensityintheintensivecareunit.TheEuropain®study.
AmJRespirCritCareMed.2014;189:39---47.
6.PayenJF,BruO,BossonJL,etal.Assessingpainincriticallyill sedatedpatientsbyusingabehaviouralpainscale.CritCare Med.2001;29:2258---63.
7.RotondiAJ, ChelluriL, SirioC,et al. Patients’recollections of stressful experiences while receiving prolonged mechan-ical ventilation in an intensive care unit. Crit Care Med. 2002;30:746---52.
8.BarrJ,Fraser GL,PuntilloKA, etal.Clinicalpractice guide-lines for the management of pain, agitation, and delirium in adultpatients in the intensive care unit.Crit Care Med. 2013;41:263---306.
9.Hamill-RuthRJ,MarohnML.Evaluationofpaininthecritically illpatient.CritCareClin.1999;15:35---54,v---vi.
10.RikerRR, Fugate JE. Participantsin theInternational Multi-disciplinaryConsensusConferenceonMultimodalityMonitoring. Clinicalmonitoringscalesinacutebraininjury:assessmentof coma,pain, agitationand delirium.Neurocrit Care. 2014;21 Suppl.2:27---37.
11.Arbour C,Gélinas C. Are vital signsvalid indicators for the assessmentofpaininpostoperativecardiacsurgeryICUadults? IntensiveCritCareNurs.2010;26:83---90.
12.ChenHJ,ChenYM.Painassessment:validationofthe physio-logicalindicatorsintheventilatedadultpatient.PainManag Nurs.2014;16:105---11.
13.PuntilloKA,MiaskowskiC,KehrleK,etal.Relationshipbetween behavioral and physiologicalindicators of pain, criticalcare patients’self-reportsofpain, andopioidadministration.Crit CareMed.1997;25:1159---66.
15.ChenYY,LaiYH,ShunSC,etal.TheChinesebehaviorpainscale forcriticallyillpatients:translationandpsychometrictesting. IntJNursStud.2011;48:438---48.
16.Pudas-TähkäSM,AxelinA,AantaaR,etal.Translationand cul-turaladaptationofanobjectivepainassessmenttoolforFinnish ICUpatients.ScandJCaringSci.2013;28:885---94.
17.AhlersSJ,vanGulikL,vanderVeenAM,etal.Comparisonof dif-ferentpainscoringsystemsincriticallyillpatientsinageneral ICU.CritCare.2008;12:R15.
18.AïssaouiY, ZeggwaghAA, Zekraoui A, et al. Validation of a behavioralpainscaleincriticallyill,sedated,andmechanically ventilatedpatients.AnesthAnalg.2005;101:1470---6.
19.RahuMA,GrapMJ,CohnJF,etal.Facialexpressionasan indica-torofpainincriticallyillintubatedadultsduringendotracheal suctioning.AmJCritCare.2013;22:412---22.
20.DehghaniH,TavangarH,GhandehariA.Validityandreliabilityof behavioralpainscaleinpatientswithlowlevelofconsciousness dueto headtraumahospitalizedinintensivecare unit.Arch TraumaRes.2014;3:e18608.
21.LatorreMarcoI,SolísMu˜nozM,FaleroRuizT,etal.Validación delaEscala de ConductasIndicadorasde Dolor paravalorar eldolorenpacientescríticos,nocomunicativosysometidosa ventilaciónmecánica:resultadosdelproyecto ESCID.Enferm Intensiva.2011;22:3---12.
22.RijkenbergS,StilmaW,EndemanH,etal.Painmeasurementin mechanicallyventilatedcriticallyillpatients:behavioralpain scaleversus critical-care painobservation tool. J Crit Care. 2015;30:167---72.
23.AlSutariMM,AbdalrahimMS,Hamdan-MansourAM,etal.Pain amongmechanicallyventilatedpatientsincriticalcareunits.J ResMedSci.2014;19:726---32.
24.YoungJ,SiffleetJ,NikolettiS,etal.UseofaBehaviouralPain Scaletoassesspaininventilated,unconsciousand/orsedated patients.IntensiveCritCareNurs.2006;22:32---9.
25.YuA,TeitelbaumJ,ScottJ,etal.Evaluatingpain,sedation, anddeliriumintheneurologicallycriticallyIll----Feasibilityand reliabilityofstandardizedtools:amulti-institutionalstudy.Crit CareMed.2013;41:2002---7.
26.Azevedo-SantosIF,AlvesIGN,Badauê-PassosD,etal. Psycho-metric analysisof Behavioral Pain Scale Brazilianversion in
sedatedandmechanicallyventilatedadultpatients:a prelimi-narystudy.PainPract.2015[Epubaheadofprint].
27.BeatonDE,BombardierC,GuilleminF,etal.Guidelinesforthe processof cross-culturaladaptationof self-report measures. Spine.2000;25:3186---91.
28.PasqualiL.Instrumentac¸ãopsicológica:fundamentose práti-cas.PortoAlegre:Artmed;2010.
29.KnausWA,DraperEA,WagnerDP,etal.APACHEII:aseverityof diseaseclassificationsystem.CritCareMed.1985;13:818---29. 30.NassarJuniorAP,NetoRCP,FigueiredoWBD,etal.Validade,
confiabilidade eaplicabilidade das versõesem português de escalasdesedac¸ãoeagitac¸ãoempacientescríticos.SãoPaulo MedJ.2008;126:215---9.
31.RamsayMA,SavegeTM,SimpsonBR,etal.Controlledsedation withalphaxolone-alphadolone.BrMedJ.1974;2:656---9. 32.SesslerCN,GosnellMS,GrapMJ,etal.TheRichmond
Agitation-SedationScale:validityandreliabilityinadultintensivecare unitpatients.AmJRespirCritCareMed.2002;166:1338---44. 33.Puntillo KA. Dimensionsof proceduralpainand its analgesic
managementincriticallyillsurgicalpatients.AmJCritCare. 1994;3:116---22.
34.PuntilloKA,WhiteC,MorrisAB,etal.Patientsperceptionsand responsestoproceduralpain:resultsfromThunderProjectII. AmJCritCare.2001;10:238---51.
35.Vaghadia H, al-Ahdal OA, Nevin K. EMLA patch for venous cannulation in adult surgical outpatients. Can J Anaesth. 1997;44:798---802.
36.GeorgeD,MalleryP.SPSSforWindowsstepbystep:asimple guideandreference.4thedition11.0updateBoston:Allyn& Bacon;2003.
37.ShroutPE,FleissJL.Intraclasscorrelations: usesinassessing raterreliability.PsycholBull.1979;86:420---8.
38.Wright JG, Young NL. A comparison of different indices of responsiveness.JClinEpidemiol.1997;50:239---46.
39.Ahlers SJ, van der Veen AM, vanDijk M, et al. The use of theBehavioralPainScaletoassesspaininconscioussedated patients.AnesthAnalg.2010;110:127---33.