REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Comparisons
of
the
effects
of
the
sevoflurane
and
propofol
on
acute
ischemia
reperfusion
and
DNA
damages
in
rabbits
Sema
Oncul
∗,
Lale
Karabiyik,
Erdem
Coskun,
Ela
Kadioglu,
Ozlem
Gulbahar
GaziUniversityFacultyofMedicine,DepartmentofAnesthesiologyandIntensiveCare,Ankara,Turkey
Received29May2015;accepted17August2015 Availableonline12April2016
KEYWORDS
Genotoxicity; Oxidativestress; Propofol; Sevoflurane;
Ischemiareperfusion injury
Abstract
Backgroundandobjectives: Theaimofthisstudywastocomparetheeffectsofsevoflurane
andpropofolanesthesiaonoxidativeDNAdamagethatoccursinlow-extremityischemiaandis
causedbytourniquetapplication.
Methods:FourteenNewZealandrabbitswererandomlyallocatedintotwoequalgroups.Group
S(n=7)receivedsevoflurane(2.5---4percent)inhalationandGroupP(n=7)receivedapropofol
infusion(1---2mg·kg−1·min−1),afterwhichapneumatictourniquetwasplacedontherightlower
extremity.Bloodsampleswerecollectedpriortotourniquetplacement(baseline),120minafter
ischemia,15minafterischemiaand120minutes(min)afterischemia.Malondialdehyde(MDA)
levelswereanalyzedtodeterminelipidperoxidation,andsinglecellgelelectrophoresis(SCGE)
wasusedtodetermineDNAdamage.
Results:At15minafterischemia,theMDAlevelsinGroupP(8.15±2.61M)werehigherthan
baseline(6.26±3.19M,p=0.026)andGroup S(4.98±0.77M,p=0.01).DNA damagewas
similarinbothgroups,althoughDNAdamagewashigherthanbaseline(tailmoment0.63±0.27,
tailintensity3.76±1.26)inGroupPatthe15thminuteofreperfusion(tailmoment1.05±0.45,
p=0.06; tail intensity5.33±1.56, p=0.01).The increase in tailmoment andtail intensity
returnedtonormallevelsinbothgroups2hoursaftertheterminationofischemia.
Conclusion: Giventhatoxidativestress andgenotoxiceffectdisappearinthelatestages of
reperfusion,weconcludethatneithersevofluranenorpropofolcanbeconsideredsuperiorto
theotherinanesthesiapracticesforextremitysurgeriesinvolvingtheuseofatourniquet.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeAnestesiologia.
ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](S.Oncul). http://dx.doi.org/10.1016/j.bjane.2015.08.013
36 S.Onculetal.
PALAVRAS-CHAVE
Genotoxicidade; Estresseoxidativo; Propofol;
Sevoflurano; Lesãodeisquemia reperfusão
Comparac¸õesdosefeitosdesevofluranoepropofolsobreisquemia-reperfusãoaguda edanosaoDNAemcoelhos
Resumo
Justificativaeobjetivos: Oobjetivodeste estudofoi compararos efeitos daanestesiacom
sevofluranoepropofolsobreodanooxidativoaoDNAqueocorrenaisquemiadeextremidade
inferioreécausadapelaaplicac¸ãodetorniquete.
Métodos: Quatorzecoelhosdarac¸aNovaZelândiaforamalocadosaleatoriamenteemdois
gru-posiguais.GrupoS(n=7)recebeuinalac¸ãodesevoflurano(2.5---4%)eGrupoP(n=7)recebeu
perfusãodepropofol(1---2mg·kg−1·min−1),logoapósumtorniquetepneumáticofoicolocadona
extremidadeinferiordireita.Amostrasdesangueforamcoletadasantesdacolocac¸ãodo
torni-quete(fasebasal),após120minutosdeisquemia,15minutosapósaisquemiae120minutosapós
aisquemia.Osníveisdemalondialdeído(MDA)foramanalisadosparadeterminaraperoxidac¸ão
delipídios,eelectroforeseemgeldecélulaúnica(EGCU)foiusadaparadeterminarodanoao
DNA.
Resultados: Aos 15minutos apósa isquemia, osníveis deMDA no Grupo P (8,15±2,61M)
foramsuperioresaosdafasebasal (6,26±3,19M,p=0,026)edpGrupo S(4,98±0,77M,
p=0,01).Odanocausadoao DNAfoi semelhantenosdoisgrupos,emboratenha sidomaior
quenafasebasal(momentodacauda0,63±0,27,intensidadedacauda3,76±1,26)noGrupo
Pno15minutodereperfusão(momentodacauda1,05±0,45,p=0,06;intensidadedacauda
5,33±1,56,p=0,01). Oaumentonomomentodacaudae intensidadedacaudavoltouaos
níveisnormaisnosdoisgruposduashorasapósotérminodaisquemia.
Conclusão:Comooestresseoxidativoeoefeitogenotóxicodesaparecemnosestágiosfinaisda
reperfusão,concluímosquenãohásuperioridadetantodesevofluranoquantodepropofolem
práticasdeanestesiaparaprocedimentoscirúrgicosdeextremidadesqueenvolvemousode
torniquete.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradeAnestesiologia.
Este ´e um artigo Open Access sobuma licenc¸a CC BY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
Proximal tourniquets are often used in limb surgeries to provideabloodlessoperatingfield.Whenoxygenis reintro-duced intoischemic tissueafter tourniquetdeflation,the existence of massive free oxygen radicals causes peroxi-dationofmembrane lipids.Thisprocesstriggersoxidation of the polyunsaturated fatty acids, destroying membrane structuresandproducingtoxicmetabolitessuchas malondi-aldehyde(MDA).1,2Thisprocessplaysasignificantroleinthe pathogenesisofreperfusioninjuries.MDAisalowmolecular weightaldehydeandanintermediateproductalipid perox-idation.Ithasoftenbeenusedasamarkeroffreeradical formation.
˙Ischemia---reperfusion (I/R) induced oxygen radical for-mationcausesoxidativeDNAdamageandplaysasignificant roleinthepathogenesisofreperfusioninjuries.3,4Alimited amount of information exists on oxidative DNA damage intourniquet-induced reperfusioninjuries, although anes-theticdrugsandsurgery-relatedstressareknowntocause cellulardamage.5
Sevoflurane and propofol are volatile and intravenous agentsthatareincommonuseinthefieldanesthesia.Some clinical andexperimental studies without I/R have shown thatsevofluranecausesreversibleDNAdamage,5,6although
differentinvivoandinvitrostudieshaveshownthat propo-foldecreasesDNAdamage,orcausesnoDNAdamage.7---9
Genotoxic assays are commonly used to monitor DNA damage.The SCGE(cometassay)hasbeenwidely usedin bothinvitroandinvivostudies,becauseitisasensitiveand simplemethodologyformeasuringsingle-strandand double-strandbreaks,alkalilabilesites,oxidativelesionsandDNA repair.10,11
Thisstudycomparestheeffectsofsevofluraneand propo-folonDNAdamageinatourniquet-inducedlowerextremity ischemiamodel.Forthepurposeofthestudy,thesurgical stressfactorwaseliminated,MDAlevelsweremeasuredto determinelipidperoxidation,andSCGEwasusedto deter-mineDNAdamage.
Methods
Figure1 Infusionofpropofol,intravenousandintraarterial catheterization.
Figure2 ApplyingthemaskofthegasmixtureandBIS probe.
Arterialandvenouslineswereinsertedthroughtheearin alltestsubjectsduringsamplingandforisotonicsaline infu-sion,respectively. Baselinebloodsamples weretakenand theinvasivearterialbloodpressurewasmonitored(Fig.1). Hemodynamicparametersofinvasivebloodpressure,heart rate,respiratoryrate,periphericoxygensaturation(SpO2) (NihonCohden,Life ScopeBSM-5135K, Japan)and Bispec-tralIndex(BIS)Monitoring(BispectralIndexMonitorModel 2000,AspectMedicalSystems,Inc.,Newton,MA,USA)were recorded at 15min intervals during the procedure. After hairremoval,pediatricprobeswereusedforBISmonitoring (AspectMedical Systems,Inc.,Norwood,USA).During the study,theBISwaskeptat50±10percentand5mL·kg−1·h−1 isotonicsalinewasinfusedduringtheprocedure.
The rabbitswere randomly allocated to twogroups of seven.Anesthesia wasinduced withthe inhalation of7---8 percent sevoflurane in Group S, and with the infusion of 1---2mg·kg−1·min−1 propofolin GroupP(Figs.1 and2).An adequate levelofinduction wasdeterminedbythe disap-pearanceofeyemovementsandcorneareflexinadditionto maintainingBIS<60percent.Theanesthesiawasmaintained inGroupSthroughtheinhalationof2.5---4percent sevoflu-raneandthroughtheinfusionof1---2mg·kg−1·min−1propofol inGroupP.Agasmixturewasadministeredbyusingaface
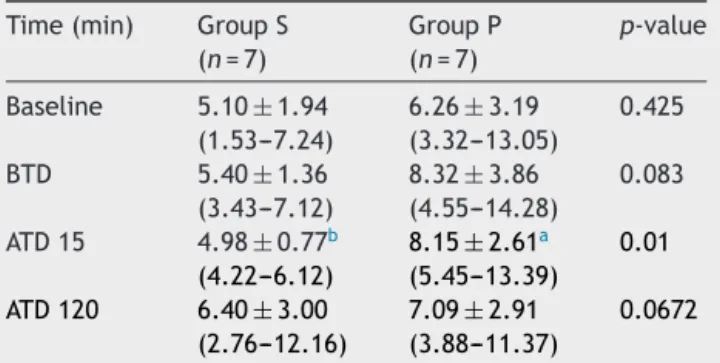
Table1 MDAlevels(M)[mean±SD(min---max)].
Time(min) GroupS
(n=7)
GroupP
(n=7)
p-value
Baseline 5.10±1.94
(1.53---7.24)
6.26±3.19
(3.32---13.05)
0.425
BTD 5.40±1.36
(3.43---7.12)
8.32±3.86
(4.55---14.28)
0.083
ATD15 4.98±0.77b
(4.22---6.12)
8.15±2.61a
(5.45---13.39)
0.01
ATD120 6.40±3.00 (2.76---12.16)
7.09±2.91 (3.88---11.37)
0.0672
BTD, beforetourniquetdeflation;ATD,aftertourniquet defla-tion.
a p=0.026,comparisonwiththebaseline. b p=0.01,comparisonwithGroupP.
mask at the flow rate of 4L·min−1 (Dameca, Denmark). Spontaneousrespiration wasmaintained toachieve an O2 saturation of ≥95 percent. Both groups were completely expressedbyrubberbandagefromtherightextremity,anda tourniquetwasplacedbyapplying200mmHgpressure (Pedi-atriccuffno2,DeRoyal,Powell,TN,USA).Tourniquetwas appliedfor120min.
Bloodsampleswerecollected asthebaselinesamples, 1minbeforetourniquetdeflation(BTD),and15and120min after tourniquet deflation (ATD 15 and ATD 120, respec-tively).
Malondialdehydedetermination
One of the most common methods used to indicate the presence of free oxygen radicals is the determination of MDA as an index of lipid peroxidation. During the study, thedecreaseinthe MDAlevelsassessedoverthe thiobar-bituric acid (TBA) reactions was found to be an indirect indicationofadecreaseoffreeoxygenradicals.Theplasma MDAlevelwasmeasuredbyimplementingthecolorimetric methodbasedontheTBAreactionwiththeMDA.14
SCGE(cometassay)method
ThecometassayfollowedtheprotocolsdescribedbySingh etal.andTiceetal.withsomemodifications.15,16TheSCGE methodexaminestheDNAdamageandrepairmechanisms under different experimental conditions. Normal lympho-cytes have around, bright-lookingnucleus in the middle, whichislessdenseonthesides.Itgainsanirregularlyedged appearancealongwiththebeginningofthemigrationofDNA fragmentsoutsidethenucleus.Lymphocytestaketheshape ofacometasthedamageincreases,hencethename‘comet assay’.Dependingontheseverityofthedamage,the micro-scopicappearanceofthecellextendsfromthecentertothe periphery.Thetailintensity,intermsoffluorescence,tail
38 S.Onculetal.
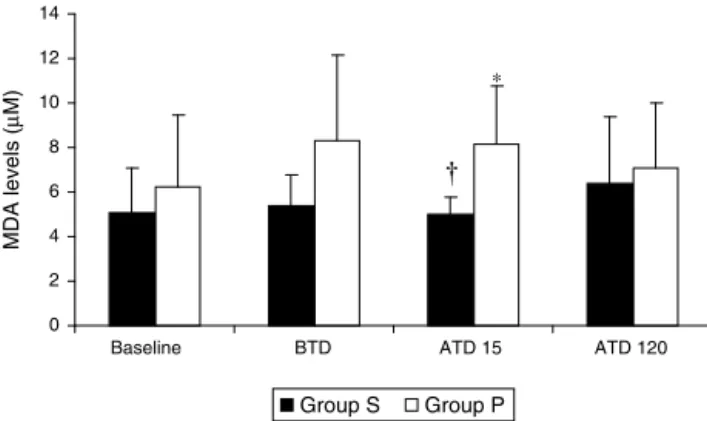
0 2 4 6 8 10 12 14
BTD
Baseline ATD 15 ATD 120
Group S Group P ∗
MDA
levels
(
µ
M)
Figure3 MDAlevels(mean±SD)(*p=0.026,comparisonwith thebaseline;†p=0.01,comparisonwithGroupP.BTD,before
tourniquetdeflation;ATD,aftertourniquetdeflation).
Statisticalevaluation
Data analysis was performed by using Statistical Package for the Social Sciences (SPSS) for Windows, version 15.0. Time-relatedchangeswithingroupsandinaccordancewith controlwerecomparedbyPairedttestandWilcoxon-Xtest, andcomparisonsbetweengroupswereperformedby imple-mentingtheStudent’sttestandtheMann---WhitneyUtest. Datawasexpressedasmean±SDandp<0.05wasaccepted assignificant.
Results
MDA
MDAlevelswerenotfoundtobestatisticallysignificant dif-ferent compared with baseline samples in Group S. The increase in the MDA levels in Group P at ATD 15 was foundtobehigherthanthebaselinevalues(8.15±2.61M; p=0.026). At the same time, this value was significantly higherthaninGroupS(4.98±0.77M)atATD15(p=0.01)
(Table1,Fig.3).
DNAdamageassessment
Therewasnosignificantdifferenceinthebaseline,BTD,ATD 15and ATD120 levelsbetween the groups (Table2). The increaseinthetailmoment(p=0.031)andthetailintensity (p=0.029)inGroupSatBTDwerefoundtobestatistically significantcomparedwithbaselinesamples(Table 2).The increasein thetailmoment(p=0.006)andthe tail inten-sity(p=0.01)inGroupPatATD15werefoundtobehigher thanthebaselinevalues(Table2).Therewasnosignificant differencebetweenGroupSandGroupPatalltimeperiods.
Discussion
Ourfindingsindicatethatneithersevofluranenorpropofol issuperiortotheotherintermsofpreventingtheoxidative stressandgenotoxicitythatemerge intourniquet-induced I/Rinjuries.
A proximaltourniquet is often used in limb surgery to provideabloodlessoperatingfield.Tourniquetapplication
causes metabolic changesthat depend ontheduration of tourniquet inflation and anesthetic technique.17 The safe rangeofinflationtimeisacceptedtobebetween1and3h. Forthisreasonweoptedforatourniquetperiodof2hinthe presentstudy.
˙Ischemia---reperfusionresults in thegenerationof toxic reactive oxygen species (ROS) in the organs. ˙Ischemia reduces the activity of cellular defence enzymes against ROS,andreperfusionortheintroductionofoxygenfurther disturbs the delicate balance of oxidants/antioxidants.18 MeasurementofMDAlevelsisthemostsensitivemarkerto determine thedegreeoflipidperoxidation.19,20 Sensitivity reaches its highest level between the fifth and twentieth minutes following tourniquet deflation.2 In our study the increase in the MDAlevels wasfound to behigher in the propofol group 15min following tourniquet deflation than in the sevoflurane group. It was observed that the lipid peroxidationcouldbebettersuppressedinthesevoflurane group duringthe early reperfusionperiodascomparedto thepropofolgroup.
Budic etal. have demonstrated that total intravenous anesthesia with propofol and regional anesthesia tech-niques provide better antioxidant defence and reduce endothelialdysfunctionthangeneralinhalationalanesthesia withsevofluraneduringtourniquetapplicationinpediatric extremity surgery.19,20 Arnaoutoglou et al. have reported thatpropofolmayhave antioxidantpropertiesin orthope-dic surgery requiring tourniquet application, but the use of sevoflurane needs further study.21 Some authors have demonstrated that plasma concentrations of propofol are abletoinhibitlipidperoxidationintherangethatis clini-callyusedinanesthesia.22Brazetal.,however,usedclinical doses of propofol (plasma concentration: 2---4g·mL−1) in elective surgeries without I/R,and showed that propofol does not decrease lipid peroxidation.7 These and several other authors believe that only higher concentrations of propofolcouldshowfreeradicalscavengingactivity.7,23 Sim-ilartothestudybyBrazetal.,wefoundthatpropofoldid notdecreaselipidperoxidation;contrarytoother studies, however, we did notperform any surgery, andperformed ischemiafor120min.Althoughplasmapropofollevelswere not measured in our study, increased MDA levels were found at the 15th minute of reperfusion in the propofol group.
˙Ischemia---reperfusioninduced oxygenradicalformation causes oxidativeDNAstrandbreaksand playsasignificant roleinthepathogenesisofreperfusioninjuries.Thesingle cellgelelectrophoresis(cometassay)isasimple,sensitive, andrapidmethodforestimatingDNAdamage.10 Numerous studies have shown that I/R-induced DNAdamage can be investigatedinhumanperipheralleucocytesusingthe mod-ifiedalkalinecometassay.3,24Afterischemia,thegenotoxic damagewasdetectedinhumanperipheralleucocytes,and itleadsespeciallytothereleaseofsubstantialamountsof oxygen radicalsand other reactive agents.10 In ourstudy, weusedthismethodtoanalyzetheDNAdamagecausedby anestheticagents.
reperfusion
and
DNA
damage
during
anesthesia
39
Table2 Tailmoment,taillengthandtailmoment,in50cells[mean±SD(min---max)].
Time(min) GroupS(n=7) GroupP(n=7) p-value
Tailmoment Taillength Tail
intensity
Tailmoment Taillength Tail
intensity
Tail moment
Tail length
Tail intensity
Baseline 0.75±0.27
(0.36---1.17)
25.19±1.88
(22.93---28.81)
4.55±1.37
(2.43---6.76)
0.63±0.27
(0.29---1.17)
25.25±3.55
(22.10---32.87)
3.76±1.26
(1.73---6.07)
0.422 0.971 0.285
BTD 1.12±0.38a
(0.77---1.86)
30.34±9.79 (24.98---52.23)
6.14±1.48a
(4.41---8.62)
1.80±1.72 (0.58---5.32)
35.10±18.05 (23.66---71.39)
7.53±4.23 (3.53---14.43)
0.328 0.551 0.427
ATD15 1.51±1.70 (0.51---5.34)
34.46±24.90 (23.61---90.89)
7.47±5.96 (3.52---20.76)
1.05±0.45a
(0.50---1.90)
27.69±7.73 (21.77---44.36)
5.33±1.56a
(3.33---8.42)
0.506 0.505 0.377
ATD120 1.12±0.68 (0.65---2.63)
29.13±9.51 (21.99---49.89)
6.15±3.35 (3.83---13.53)
1.06±0.56 (0.51---1.89)
26.22±5.28 (21.11---36.68)
5.45±2.09 (3.38---8.85)
0.881 0.492 0.646
BTD,beforetourniquetdeflation;ATD,aftertourniquetdeflation. Therewasnosignificantdifferencebetweenthegroups.
40 S.Onculetal.
5---30minaftertourniquetrelease,andthendeclined over a 2h period,but did not return to pre-ischemic baseline values; this suggests that I/R induces genotoxic effects inhuman leucocytes,presumablyin responsetooxidative stressduringreperfusion.3
Some studieshave demonstrated thatgeneticmaterial canbedamaged withthehalogenatedanesthetics, evalu-atedbysinglecellgelelectrophoresisassay.5,6,25 Karabiyik etal.usedthismethodtoevaluateDNAdamageinpatients who received sevoflurane and isoflurane anesthesia. The authorshave concludedthatboth agents causereversible DNA damage, but that there is no significant difference betweentheminthisregard.6Propofoldiffersfromvolatile anesthetics because it does not show mutagenic effects in vitro or in vivo.7,9 Braz et al. reported that propofol does notinduce DNA damagein white blood cells (WBCs) by using an alkaline version of the single cell gel elec-trophoresisassay.7Inaddition,propofoldidnotinducesister chromatidexchanges(SCEs)inchildren’slymphocytes8and didnotincreasechromosomalaberrationsincardiacsurgery patients.9
AccordingtoAllevaetal.itisdifficult toassessinvivo whetheranestheticsor surgicalstressisthemaincauseof thecell damage.These authors evaluatedgenotoxicity in patientssubjectedtosevofluraneanesthesiaanddidnotfind significantalterationsinDNAafter15minanesthesia induc-tionbeforesurgery.5Inarecentstudy,Brazetal.reported thatpatientswhounderwentminorsurgeryundergeneral anesthesiawithinhaledsevofluraneandisofluraneor with intravenouspropofol didnot induceDNAstrand breaks or alkali-labilesitesinhumanperipheral lymphocytes.26 Sim-ilarlyinourstudy,weeliminatedthesurgicalstressfactor andourresultsalsocontradictedthoseofotherstudies.In ourstudy,tailmomentandtailintensitylevels(indicators of DNAdamage) increasedgradually in both groups when comparedtothebaselinelevels.Inthesevofluranegroup, DNA damage increased at the 120th minute of ischemia; incontrastDNA damagewasmoreprominent in theearly periodofreperfusion,andthisincreasewasparalleltothe increase in MDA levels. These findings may indicate the inabilityofpropofoltosuppressoxidativestressefficiently. In the sevoflurane group, increased DNA damage prior to reperfusionsupportsthegenotoxicpropertyofsevoflurane. Thedifferencebetweenthegroupsdisappearedatthe120th minuteofreperfusion.
Conclusions
ThisexperimentalI/Rstudyhasshownthatsevofluranecan control lipidperoxidation better than propofol. Propofol, mayrequire higherdoses (compared tothe clinical dose) topreventlipidperoxidation.Giventhelack ofdifference betweenthetwoanestheticsinlatestagesofreperfusion, we believe that neither sevoflurane nor propofol can be consideredsuperiorintermsofpreventingoxidative stress-relatedgenotoxicityinextremitysurgeriesinvolvingtheuse ofatourniquet.Itisknownthatallanestheticshaveharmful side-effects,andsowhatisimportantistochoosethe appro-priateagentwiththeleasttoxicside-effect.Inthisregard, it canbe said thatthere is a need for more genotoxicity studiesonoxidativestress.
Limitations
The evaluationof DNAdamagefromthe localtissue sam-ple(muscle,etc.)andthemeasurementofplasmapropofol levelswouldallowmoreinformativestudies.Thismightbe consideredasthelimitationsofourstudy.
Funding
GaziUniversity---ScienceResearchProjects.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GogusN, Akan B,Bayrakci S, et al. The effects ofa small-dose ketamine-propofol combination on tourniquet-induced ischemia---reperfusioninjuryduringarthroscopickneesurgery. JClinAnesth.2014;26:46---51.
2.ChengYJ,ChienCT,ChenCF.Oxidativestressinbilateraltotal kneereplacement, underischaemictourniquet.JBoneJoint SurgBr.2003;85:679---82.
3.WillyC,DahoukS,StarckC,etal.DNAdamageinhuman leuko-cytesafterischemia/reperfusioninjury. FreeRadic BiolMed. 2000;28:1---12.
4.Cordis GA, Maulik G, Bagchi D, et al. Detection of oxida-tive DNA damage to ischemic reperfused rat hearts by 8-hydroxydeoxyguanosine formation. J Mol Cell Cardiol. 1998;30:1939---44.
5.AllevaR,TomasettiM,SolenghiMD,etal.LymphocyteDNA dam-ageprecedesDNArepairorcelldeathafterorthopaedicsurgery undergeneralanaesthesia.Mutagenesis.2003;18:423---8. 6.KarabiyikL,Sardas¸S,PolatU,etal.Comparisonof
genotoxic-ityofsevofluraneandisofluraneinhumanlymphocytesstudied invivousingthecometassay.MutatRes.2001;492:99---107. 7.BrazMG,MagalhãesMR,SalvadoriDM,etal.EvaluationofDNA
damageandlipoperoxidationofpropofolinpatientsundergoing electivesurgery.EurJAnaesthesiol.2009;26:654---60. 8.KrauseTK, Jansen L, ScholzJ, et al. Propofolanesthesia in
childrendoes notinducesisterchromatidexchanges in lym-phocytes.MutatRes.2003;542:59---64.
9.Karahalil B,Ya˘garS, BahadirG, et al.Diazepam and propo-folusedasanestheticsduringopen-heartsurgerydonotcause chromosomal aberrations in peripheral blood lymphocytes. MutatRes.2005;581:181---6.
10.Collins AR. The comet assay for DNA damage and repair: principles, applications, and limitations. Mol Biotechnol. 2004;26:249---61.
11.TiceRR, AgurellE, AndersonD, etal. Singlecell gel/comet assay:guidelinesforinvitroandinvivogenetictoxicology test-ing.EnvironMolMutagen.2000;35:206---21.
12.HardySC,Homer-VanniasinkamS,GoughMJ.Thetriphasic pat-tern of skeletal muscle bloodflow inreperfusion injury: an experimentalmodelwithimplicationsforsurgeryontheacutely ischaemiclowerlimb.EurJVascSurg.1990;4:587---90. 13.Instituteof LaboratoryAnimalResearch, CommissiononLife
Sciences,NationalResearchCouncil.Guideforthecareanduse oflaboratoryanimals.Washington,DC:TheNationalAcademies Press;1996.
bya fully validated HPLC method. Nephrol Dial Transplant. 1999;14:946---51.
15.SinghNP,McCoyMT,TiceRR,etal.Asimpletechniquefor quan-titationoflowlevelsofDNAdamageinindividualcells.ExpCell Res.1988;175:184---91.
16.Tice RR, Andrews PW, Hirai O, et al. The single cell gel (SCG)assay:anelectrophoretictechniqueforthedetectionof DNAdamageinindividualcells.AdvExpMedBiol.1991;283: 157---64.
17.Kam PC, Kavanagh R, Yoong FF. The arterial tourniquet: pathophysiologicalconsequencesandanaestheticimplications. Anaesthesia.2001;56:534---45.
18.McCordJM.Freeradicalsand myocardialischemia:overview andoutlook.FreeRadicBiolMed.1988;4:9---14.
19.Budic I,Pavlovic D,Kocic G, et al. Biomarkers ofoxidative stressandendothelialdysfunctionaftertourniquetreleasein children.PhysiolRes.2011;60Suppl.1:S137---45.
20.Budic I, Pavlovic D, Kitic D, et al. Tourniquet-induced ischemia---reperfusioninjuriesduringextremitysurgeryat chil-dren’sage:impactofanestheticchemicalstructure.RedoxRep. 2013;18:20---6.
21.Arnaoutoglou H, Vretzakis G, Souliotis D, et al. The effects of propofol or sevoflurane on free radical production after tourniquet induced ischemia---reperfusion injury during knee arthroplasty.ActaAnaesthesiolBelg.2007;58:3---6.
22.Aarts L, van der Hee R, Dekker I, et al. The widely used anestheticagentpropofolcanreplacealpha-tocopherolasan antioxidant.FEBSLett.1995;357:83---5.
23.GreenTR,BennettSR,NelsonVM.Specificityandpropertiesof propofolasanantioxidantfreeradicalscavenger.ToxicolAppl Pharmacol.1994;129:163---9.
24.KarahalilB,PolatS,SenkoyluA,etal.EvaluationofDNAdamage aftertourniquet-induced ischaemia/reperfusion injuryduring lowerextremitysurgery.Injury.2010;41:758---62.
25.Sardas¸S,KarabiyikL,AygünN,etal.DNAdamageevaluated bythealkalinecometassayinlymphocytesofhumans anaes-thetizedwithisoflurane.MutatRes.1998;418:1---6.
![Table 2 Tail moment, tail length and tail moment, in 50 cells [mean ± SD (min---max)].](https://thumb-eu.123doks.com/thumbv2/123dok_br/14960225.506543/5.1216.98.1152.329.541/table-tail-moment-tail-length-tail-moment-cells.webp)
