REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Combined
spinal---epidural
analgesia
in
labour:
its
effects
on
delivery
outcome
Suneet
Kaur
Sra
Charanjit
Singh
a,
Nurlia
Yahya
a,∗,
Karis
Misiran
b,
Azlina
Masdar
a,
Nadia
Md
Nor
a,
Lee
Choon
Yee
aaDepartmentofAnaesthesiologyandIntensiveCare,UniversitiKebangsaanMalaysiaMedicalCentre,KualaLumpur,Malaysia bDepartmentofAnaesthesiologyandIntensiveCare,FacultyofMedicine,UniversitiTeknologiMARA,JalanHospital,Malaysia
Received5July2014;accepted3September2014 Availableonline28November2014
KEYWORDS
Combined spinal---epidural;
Labouranalgesia;
Foetaloutcome;
Durationoflabour
Abstract
Backgroundandobjectives: Combinedspinal---epidural(CSE)hasbecomeanincreasingly pop-ular alternative totraditional labour epidural dueto itsrapid onset andreliable analgesia provided.Thiswasaprospective,convenientsamplingstudytodeterminetheeffectsofCSE analgesiaonlabouroutcome.
Methods:Onehundredandtenhealthyprimigravidaparturientswithasingletonpregnancyof
≥37weeksgestationandintheactivephaseoflabourwerestudied.Theywereenrolledtothe CSE(n=55)orNon-CSE(n=55)groupbasedonwhethertheyconsentedtoCSEanalgesia. Non-CSEparturientswereofferedothermethodsoflabouranalgesia.Thedurationofthefirstand secondstageoflabour,rateofinstrumentalvaginaldeliveryandemergencycesareansection, andApgarscoreswerecompared.
Results:Themeandurationofthefirstandsecondstageoflabourwasnotsignificantlydifferent betweenbothgroups.Instrumentaldeliveryratesbetweenthegroups werenotsignificantly different(CSEgroup,11%versusNon-CSEgroup,16%).Theslightlyhigherincidenceofcesarean sectionintheCSEgroup(16%versus15%intheNon-CSEgroup)wasnotstatisticallysignificant. Neonataloutcome intermsofApgarscoreoflessthan7at1and5minwas similarinboth groups.
Conclusion: Therewerenosignificantdifferencesinthedurationoflabour,rateofinstrumental vaginal deliveryandemergency cesareansection, andneonataloutcomeinparturientswho receivedcomparedtothosewhodidnotreceiveCSEforlabouranalgesia.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](N.Yahya). http://dx.doi.org/10.1016/j.bjane.2014.09.006
PALAVRAS-CHAVE
Combinac¸ão
raqui-peridural;
Analgesiadeparto;
Resultadofetal;
Durac¸ãodoparto
Analgesiacombinadaraquiperiduralemtrabalhodeparto:seusefeitossobreo
desfechodoparto
Resumo
Justificativaeobjetivos: Aanalgesiacombinadaraquiperidural(RP)tornou-seumaalternativa cadavez mais popular para o trabalhode partotradicional devido ao seurápido início de ac¸ãoeanalgesiaconfiável.Estefoium estudoprospectivodeamostragemconvenientepara determinarosefeitosdaRPsobreodesfechodoparto.
Métodos: Centoedezparturientesprimigestassaudáveis,comgestac¸ãoúnicade≥37semanas degestac¸ãoenafaseativadotrabalhodepartoforamincluídas.Aspacientesforamdesignadas paraosgruposRP(n=55)ounão-RP(n=55)combaseemseusconsentimentosparaaanalgesia combinadaRP.Asparturientesdogruponão-RPreceberamoutrosmétodosdeanalgesiapara oparto.Asdurac¸õesdoprimeiro esegundo estágiodotrabalhodeparto,astaxasdeparto vaginalinstrumentalecesarianadeemergênciaeosescoresdeApgarforamcomparados. Resultados: Amédiadedurac¸ãodoprimeiroesegundoestágiodotrabalhodepartonãofoi significativamentediferenteentreosdoisgrupos.Astaxasdepartoinstrumental nãoforam significativamentediferentes entreosgrupos, grupoRP (11%) versus gruponão-RP(16%). A incidêncialigeiramentemaiordecesariananogrupoRP(16%versus15%nogruponãoRP)não foiestatisticamentesignificativa.OdesfechoneonatalemtermosdeíndicedeApgarinferior a7.
Conclusão:Nãohouvediferenc¸assignificativasemrelac¸ãoàdurac¸ãodotrabalho,àstaxasde partovaginalinstrumentalecesarianadeemergênciaeaodesfechoneonatalemparturientes quereceberamRPparaanalgesiadepartoemcomparac¸ãocomaquelasquenãoreceberam. ©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Labourpainis oneofthe mostdistressing types ofpaina
personmayhavetoendure.TheAmericanCollegeof
Obste-tricians and Gynaecologists has suggested that: ‘‘Labour
resultsinseverepainfor manywomen.Thereisnoother circumstancewhereitisconsideredacceptableforaperson toexperienceseverepain,amenabletosafeintervention, whileunderaphysician’scare’’.1Morewomennowadaysare optingforpainreliefmethodsduringlabour.Epidural anal-gesiahasgainedincreasingpopularityworldwideasaresult ofitsabilitytoprovideanalgesiawhichismoresuperiorto othermethodsofpainrelief.
Controversyexistshowever,concerningitseffectonthe courseand outcomeof labour. As aresultof this, consid-erableresearchhasbeenperformed andfindingshaveled tochanges inpractice.Epiduralanalgesiahasbeen previ-ouslyimplicated in prolonging labour, increasing oxytocin requirements,aswellasincreasinginstrumentaland oper-ativedeliveryrates.However,thereisincreasingevidence whichrefutessomeoftheseclaims.2
Combinedspinal---epidural(CSE)hasbecomean increas-ingly popular alternative to the traditional epidural. The local anaesthetic---opioid combination administered intrathecallyprovidesrapid-onset,potentandreliable anal-gesia,withminimalmotorblockadeduringthefirststageof labour,enablingmaternalmobility,andresultingingreater maternalsatisfaction.3,4ArecentstudycomparingtheCSE technique to traditional epidural analgesia showed that, althoughbothtechniqueswereexcellentanalgesicoptions,
CSEprovidedsignificantlyfasterandbetterpainreliefduring thefirststageoflabour.5
NumerousstudiescomparingepiduralandCSEor epidu-ralandnon-epiduralanalgesiahaveshownvariableresults, butnonehavecomparedCSEwithothermethodsoflabour analgesia.6---8IntheCochranedatabaseofsystematicreviews in2011comparingepiduralversusnon-epiduralorno anal-gesia in labour, CSE was included together with epidural analgesiaandnotasaseparateentity.Inviewoftheabove, wedecidedtolookattheeffectCSEhadonlabouroutcome comparedwithalternativemethodsoflabouranalgesia.Our endpointsweredurationoftheactivephaseofthefirstand secondstagesoflabour,rateofinstrumentalvaginaldelivery andemergencycesareansection,andneonataloutcome.
Methods
Thisprospective,convenientsamplingstudywasconducted afterobtaininginstitutionalethicsapproval.Atotalof110 parturients of American Society of Anesthesiology (ASA) I physical status was enrolled in this study after informed consent was obtained. The parturients were primigravid, agedbetween20and40 yearswithasingletonpregnancy of ≥37 weeksgestationandin theactive phaseoflabour withcervicaldilatationof3---4cm.Anyparturientwith preg-nancyrelatedillness orcontraindicationstoCSEanalgesia wasexcludedfromthisstudy.
parturientswereconfirmedbytheobstetricteamtobein theactivephaseoflabour(cervicaldilatationof3---4cmwith regularcontractions),theyweretransferred tothelabour room.ThosewhoconsentedtoCSEanalgesiawereenrolled intotheCSEgroup,whereasparturientswhodeclined CSE analgesiawereofferedotherformsofanalgesiaandenrolled intothe Non-CSEgroup. Parturients in theNon-CSE group wereofferedeitherentonox(N2O/O2;50%/50%)or
intramus-cular(IM)pethidine50mgwithIMpromethazine(Phenergan) 12.5mg.Theparturient’sbloodpressureandpulseratewere monitoredathourlyintervals.Foetalheartrateandthe fre-quencyanddurationofuterinecontractionswereassessed withcontinuouscardiotocographicmonitoring.
In theCSEgroup, infusion oflactated Ringer’ssolution was commenced and the parturients were placed in the sittingposition.Theprocedurewasperformedunder asep-tic precautions at L3---L4 or L4---L5using a pre-packed set containingan18-gaugeepiduralneedle,20-gaugeepidural catheterand27-gauge spinalneedle(BDDurasafeTMPlus).
The epiduralspace was identified using the loss of resis-tance to saline technique, after which the spinal needle wasinserted throughthe epiduralneedle.Upon visualiza-tionofbackflowofcerebrospinalfluid,anintrathecaldose of0.5mLof0.2%ropivacainewith0.5mLoffentanyl(25g)
wasadministered.Theepiduralcatheterwastheninserted 3---5cmintotheepiduralspaceandsecured.Theparturient wasthen positionedsupinewithleftuterinedisplacement andtheheadendofthebedelevatedto20---30◦.Thelevel
ofsensoryblockadewascheckedtoensurethesensorylevel was≥T10,afterwhichanepiduralinfusionof0.0625% ropi-vacainewithfentanyl2g/mLwasstartedat 8mL/h.The
parturients’ hemodynamic parameters were monitored at 5minintervalsduringandaftertheprocedureforthefirst 15min,thenevery15minforthefirsthour,thenhalf-hourly afterthat.Hypotension,definedasa20%reductionin sys-tolicbloodpressurefrombaseline,wastreatedbyturning theparturienttotheleftlateralpositionandadministering maternal oxygen, intravenous fluid infusion, or vasopres-sor (ephedrine 6mg or phenylephrine 50g per bolus) as
indicated.
Throughoutlabour, sensorylevel, motorblockandpain scorewereassessedathourlyintervals.Thedegreeofmotor blockwasassessedusingtheModifiedBromageScore(MBS) where1,completeblock,unabletomovefeetorknee;2, almostcomplete block,able tomove feetonly;3, partial block,justabletomovetheknees;4,detectableweakness ofhipflexionwhilesupine;5,nodetectableweaknessofhip flexionwhilesupine.ParturientswithMBS≤2and/orsensory level≥T6wasregarded ashaving anexcessively denseor highepiduralblockrespectively,andmanagedaccordingly. PainwasassessedusingtheNumericRatingScale(NRS) withscoresrangingfrom0,indicatingnopainto10,being theworstpainimaginable.Breakthroughpainwasmanaged by administering additional epidural bolus doses and/or increasingtheepiduralinfusionrate,dependingontheNRS score.Forparturientswithpainscores of3---5, the epidu-ralinfusionratewasincreasedincrementallytoamaximum of12mL/h.Those withpainscores ≥6weregiven2---3mL bolusdosesofepidurallignocaine2%toamaximumof8mL. The epidural wasassumed tobe ineffective if significant pain(NRSscore>5)persisteddespitethemaximumtopup dose.Theseparturientswereofferedtohavetheepidural
re-sited. If they were not keen to do so, an alternative meansofanalgesiawouldbeadministered.Parturientswho requiredre-sitingoftheepiduraloranalternativemeansof analgesiawereexcludedfromthisstudy.Theepidural infu-sionwascontinued until delivery of the babyand ceased onlyaftertheepisiotomywoundwassutured.
Obstetric management was similar in both groups. Amniotomywasperformed ifthe foetal membraneswere intact.Pelvicexaminationtoevaluatetheprogressoflabour wasperformed at regularintervals asper labour manage-ment protocol. Oxytocin augmentation was prescribed as necessary toachieve a cervical dilation rateof ≥1cm/h. The decision to proceed to vaginalinstrumental or oper-ative delivery was made according to maternal or foetal indications.
Datacollectedincludeddurationofthefirstandsecond stages of labour, oxytocin augmentation, labour outcome (spontaneousvaginaldelivery,instrumentalvaginaldelivery orcesareansection)aswellas1-and5-minApgar scores. Theindicationforemergencylowersegmentcesarean sec-tion (EMLSCS) was also recorded. Foetal outcome was assessedbasedonpreviousstudies wherescores lessthan 7wereconsideredaspoorApgarscores.4,9Inaddition,any incidence of post-partum haemorrhage was recorded and forthepatientsintheCSEgroup,anyside-effects experi-enced(e.g.nausea,vomiting,pruritus,post-duralpuncture headache)weredocumentedandmanagedaccordingly.For patients in the Non-CSE group, reasons for decliningCSE analgesiawerealsodocumented.
Statistical
analysis
SamplesizewascalculatedusingtheformulabySnedecor andCochran(1989)forcontinuousvariables.Theconstant valueof10.51wasbasedonan˛-valueof0.05andapower of90%.Usingthisformula,asamplesizeof45patientsfor eachgroupwasobtained.Consideringadropoutrateof20%, 55patientswererequiredoneacharm.SPSS(version20;IBM SPSSInc.)wasusedforstatisticalanalysis.Dataanalysiswas doneusingtheindependentt-testforparametricdataand thechi-squaretest for non-parametric data.A p-value of lessthan0.05wasconsideredasstatisticallysignificant.
Results
Table1 Parturientcharacteristics(valuesexpressedasmean±standarddeviation).
CSEgroup(n=55) Non-CSEgroup(n=55) p
Age 28.8±3.6 28.6±3.8 0.755
Weight(kg) 67.2±13.6 66.2±14.4 0.717
Height(m) 1.6±0.1 1.6±0.1 0.642
BMI(kg/m2) 26.7±5.0 26.6±5.3 0.857
Gestationalage(weeks) 38.6±0.9 38.7±0.7 0.427
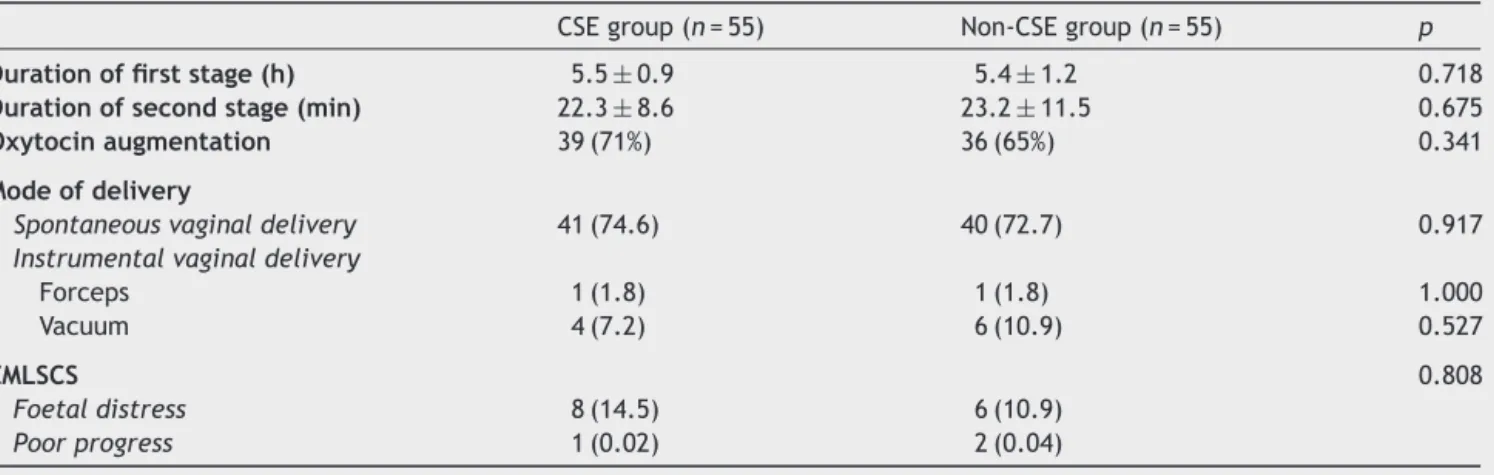
ThemainindicationforEMLSCSwasfoetaldistress,
account-ingfor14.5%and10.9%ofthecasesintheCSEandNon-CSE
grouprespectively.EMLSCSwasindicatedforpoorprogress
intheremainingcasesofbothgroups.
At 1min, threeand twoneonates in theCSE and
Non-CSEgroupsrespectivelyhadApgarscoresoflessthan7,but
thedifferencewasnotstatisticallysignificant.Noneofthe
neonateshadanApgarscoreoflessthan7at5min.
Prurituswasbyfarthemostcommoncomplicationinthe
CSEgroup.Thiswaspresentin24parturients(44%)butwas
short-livedand did notrequire intervention. Two
parturi-ents(3.6%)intheCSEgroupcomplainedofnauseawithout
vomiting.There were no other CSErelated complications
suchaspost-duralpunctureheadacheandhypotension, or
othercomplicationssuchaspost-partumhaemorrhage.
Par-turientswhodeclinedCSEanalgesiagavereasonsoffearof
backache,numbnessortheinabilitytobeardownduringthe
secondstageoflabour.
Discussion
Theeffectofneuraxialanalgesiainlabourandobstetric
out-comeshasbeenstudiedextensivelyovertheyears.Among
the endpoints studied were duration of first and second
stages of labour, oxytocin augmentation, rate of
instru-mentalandcesarean deliveries, maternal satisfactionand
neonataloutcome.10---13
Thepresentstudyshowedthatthedurationoffirststage oflabourwasnotprolongedinparturientswhoreceivedCSE analgesia.The slightincreaseinthemeandurationofthe active phase labour in the CSE group (352.3min as com-pared to 347.2min in the Non CSE group) did not reach
statistical significance. Previous studies comparing epidu-ralanalgesiawithsystemicopioidshaveshowninconsistent results.Epiduralanalgesiawaseitherimplicatedin prolong-ing or showed no effect on the first stage of labour.13---17 Interestingly,Tsenetal.demonstratedthatCSEwas associ-atedwithanincreasedcervicaldilatationrateinnulliparous patients.18 The authors postulated that the spinal anal-gesia of a CSE technique allowed, at least initially and potentially during the course of labour, for a reduction in local anaesthetic dosage when compared with conven-tionalepiduralanalgesia.Anotherpostulatewasthatpainful labourresultedinanincreaseinmaternaladrenalinelevel, whichmaybetocolyticinitself.Thereisevidenceto demon-strate that epidural analgesia may accelerate labour as theprovision ofeffective analgesiareducesmaternal cat-echolamines,andhenceminimizingitsinhibitoryeffecton uterine contractility.19 The use of CSE analgesia with its rapid onset and similar analgesic efficacy would thus be expectedtohaveasimilareffectonthedurationoflabour. Epiduralanalgesiahasbeenthoughttoprolongthe sec-ondstageoflabourbyremovingtheparturient’sinvoluntary bearingdownreflex,orbyinterferingwithmotorfunction.15 Poor maternal effort at expulsion may cause foetal mal-position during descent, which may lead to intervention in the form of instrumental delivery or cesarean section. However,inmodern-daypracticewhendilute local anaes-theticsolutionsareusedtoprovideepiduralanalgesia,the motorblockadeandhenceweaknessofpelvicfloormuscleis eitherminimalorabsent.Thiswasconfirmedbyarecently published meta-analysis on the effect of low concentra-tions versus high concentrations of local anaestheticsfor labour analgesiaonobstetricandanaestheticoutcomes.20
Table2 Labourcharacteristics(valuesexpressedmean±SD,orasnumberswithpercentageinparentheseswhereappropriate). CSEgroup(n=55) Non-CSEgroup(n=55) p
Durationoffirststage(h) 5.5±0.9 5.4±1.2 0.718
Durationofsecondstage(min) 22.3±8.6 23.2±11.5 0.675
Oxytocinaugmentation 39(71%) 36(65%) 0.341
Modeofdelivery
Spontaneousvaginaldelivery 41(74.6) 40(72.7) 0.917 Instrumentalvaginaldelivery
Forceps 1(1.8) 1(1.8) 1.000
Vacuum 4(7.2) 6(10.9) 0.527
EMLSCS 0.808
Foetaldistress 8(14.5) 6(10.9)
Theauthorsfoundthatlowconcentrationswereassociated
withareductionintheincidenceofassistedvaginaldelivery
andashortersecondstageoflabour. Weusedanepidural
infusion with a low concentration of 0.0625% ropivacaine
withfentanyl2g/mLinourstudyasperinstitutional
pro-tocol.Itisofnosurprisethatourstudyfoundnosignificant
differencebetweentheCSEandNon-CSEgroup,inthe
dura-tionofthesecond stageoflabour. Thisis similartoother
randomizedcontrolledtrialswhichcomparedCSEwith
con-ventionalepiduralanalgesia.21,22
The instrumental delivery rate is yet another impor-tantoutcomemeasure,astheprocedureincreasestherisk of maternal perineal trauma, and adverse neonatal out-comes in cases of difficult delivery.13 The 2011 Cochrane review onepidural versus non-epiduralor noanalgesiain labourshowedthatepiduralanalgesiawasassociatedwith an increased risk of assisted vaginal birth.8 However, we found thattheincidenceofinstrumentaldelivery wasnot significantly different (CSE, 9.0% versus Non-CSE, 12.7%). This was in contrast to earlier studies which reported higherratesofinstrumentaldeliveryinepiduralcompared to parenteral opioids or entonox.9,12 Studies which com-pared CSE with epidural have reported no differences in themodeofdelivery.21,22Itmustbenotedthatresultsare oftenaffectedbymultipleconfoundingfactors,suchasthe neuraxialanalgesictechnique,methodofepidural analge-sia maintenance, local anaesthetic concentration, degree of analgesia during second stage of labour and obstetric factors.13
Considerable data support the notion that neuraxial labour analgesia does not increase the risk of cesarean deliverycomparedwithsystemicanalgesia.13 Inthisstudy, we found nosignificant increase in the rates of cesarean delivery in parturients who received CSE analgesia. The Cochranereviewonepiduralversusnon-epiduralorno anal-gesia in labour showed that there was no evidence of a significantdifferenceintheriskofcesareansectionoverall eventhough therewasan increased riskof cesarean sec-tionfor foetaldistress.8 Similarly,Halpern etal.reported thattheriskofcesareandeliverywasnodifferentbetween women who received systemic opioids versus neuraxial analgesia.17 It must also be emphasised that many fac-torsotherthanlabourprogressmaycontributetocesarean delivery,suchascephalo-pelvicdisproportion,amacrosomic baby,maternalinfectionandparity.13 The resultsofthese studies,includingour own,implythatneuraxial analgesia perseis unlikelytoaffectthe chancesofanormal deliv-ery.
NeonataloutcomeassessedbyApgarscores,wassimilar inbothgroups.AllfiveneonatesinbothgroupswithApgar scores less than 7 at 1min recovered at 5min. This is in accordancewithotherstudieswhichshowednodifference inApgarscoresorcordpHinpatientsreceivingepiduralor CSEanalgesia.6,9,12,23
Themostcommonsideeffectinparturientswhoreceived CSE analgesiawas pruritus, which occurred in 44% of our parturients.Thiswastransientandtolerable,requiringno treatment.Feedbackfrompatientshaverevealedpruritus asthemostcommonsideeffectofintrathecalopioids.24Miro etal.intheirstudyconcludedthatalthoughCSEanalgesia wasmorecommonlyassociatedwithpruritusandbackpain, neverthelessitaffordedanalgesiaofsuperiorquality.23
There were some limitations in this study. Blinding of clinicians was difficult since parturients were easily differentiatedbetween the CSE andNon-CSE group. Even thoughthismaylowerthethresholdforinstrumental deliv-eryintheCSEgroup,thiswasreducedbystrictadherenceto institutionalobstetricmanagementprotocols.Secondly, as thisstudyincludedonlyASAIparturients,itsresultscannot beextrapolatedtopatientswithsignificantmedicalor preg-nancyrelated illness. These co-morbidities may influence obstetric management, thus affecting the rate of instru-mentalorcesareandeliveryandpossiblyneonataloutcome. Thirdly,thesubjectiveassessmentofcervicaldilatationmay vary among doctors of differing experience, thus affect-ingthe actual assessment of duration of labour. Oxytocin augmentationposes another confoundingfactor to labour duration.As itwaspart ofourinstitutional obstetric pro-tocol,mostofourparturientsreceivedoxytocinbutwedid notkeeprecordwhetheritwasadministeredbeforeorafter commencementof labour analgesia.Oxytocin per semay acceleratelabourprogression.Ontheotherhand,the provi-sionofeffectivelabouranalgesiacouldbepartlyresponsible forhasteningtheprocessoflabour.Howevertheremayhave beensomeparturientswhodespitebeinggivenlabour anal-gesia,hadnoalleviationofpain.Suboptimalpainreliefmay retardlabourprogressionthuspromptingadministrationof oxytocin.Finally,withregardsneonataloutcome, weonly comparedtheApgarscoresbetweenthetwogroups.Other indicesforneonatalwellbeing,suchasumbilicalcordpH, theneedfornaloxone,mechanicalventilationoradmission toNeonatalIntensive Care Unit,were not investigatedin ourstudy.
Overall, this study supports other studies which found thatCSEanalgesiadidnotadverselyaffecttheoutcomeof labour.17,18Labouringwomencanbereassuredthat,in addi-tiontoobtainingsuperioranalgesiawithCSE,theywouldbe ableto experiencea safe andnormal vaginal delivery.In conclusion,thepresentstudydemonstratedthattherewas nosignificant differenceinthe durationoflabour, rateof instrumentalvaginaldeliveryandemergencycesarean sec-tion,and neonataloutcome in parturients whoreceived, comparedtothosewhodidnotreceiveCSEforlabour anal-gesia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Pain reliefduringlabour.ACOG Committee OpinionNo. 295. AmericanCollegeofObstetriciansandGynaecologists.Obstet Gynecol.2004;104:213.
2.McGradyE.Epiduralanalgesiainlabour.ContEducAnaesthCrit CarePain.2004;4:114---7.
3.Kuczkowski KM. Ambulation with combined spinal---epidural labor analgesia; the technique. Acta Anaesthesiol Belg. 2004;55:29---34.
4.Frikha N, Ellachtar M, Mebazaa M, et al. Combined spinal---epiduralinlabor-comparisonofsulfentanilvstramadol. MiddleEastJAnesth.2007;19:87---96.
spinal---epiduralanalgesia ina private setting. AnesthAnalg. 2013;116:636---43.
6.MousaWF,Al-MetwalliR,MostafaM.Epiduralanalgesiaduring laborvsnoanalgesia:acomparativestudy.SaudiJAnaesth. 2012;6:36---40.
7.Simmons SW, Taghizadeh N, Dennis AT, et al. Combined spinal---epiduralversusepidural analgesiainlabour.Cochrane DatabaseSystRev.2012;10:CD003401.
8.Anim-Somuah M, Smyth RMD, Jones L. Epidural versus non-epiduralornoanalgesiainlabour.CochraneDatabaseSystRev. 2011;12:CD000331.
9.LiuEHC,SiaATH.Ratesofcaesariansectionandinstrumental vaginal delivery in nulliparous women after low concen-tration epidural infusions or opioid analgesia. Br Med J. 2004;328:1410---5.
10.HalpernSH,LeightonBL,OhIssonA,etal.Effectofepidural vsparenteralopioidsanalgesicsonprogressoflabour:ameta analysis.JAmMedAssoc.1998;280:2105---10.
11.PhilipsenT,JensenNH.Epiduralblockorparenteralpethidine asanalgesicinlabour:arandomizedstudyconcerningprogress inlabour and instrumentaldeliveries. EurJObstetGynecol. 1989;30:27---33.
12.LeongEW,SivanesaratnamV,OhLL,etal.Epiduralanalgesia inprimigravidaeinspontaneouslabouratterm:aprospective study.JObstetGynaecolRes.2000;26:271---5.
13.CambicCR,WongCA.Labouranalgesiaandobstetricoutcomes. BrJAnaesth.2010;105:50---60.
14.WuCY,RenLR,WangZH.Effectsofepiduralropivacainelabor analgesiaondurationoflaborandmodeofdelivery.Zhonghua FuChanKeZaZhi.2005;40:369---71.
15.RojanskyN,TanosV,ShapiraS,etal.Effectofepidural analge-siaondurationandoutcomeofinducedlabour.IntJGynaecol Obstet.1997;56:237---44.
16.AlexanderJM,SharmaSK,McIntireDD,etal.Epiduralanalgesia lengthensthefriedmanactivephaseoflabor.ObstetGynecol. 2002;100:44---50.
17.HalpernSH,LeightonBL.Epiduralanalgesiaand theprogress ofLabor. Evidence-based obstetric anaesthesia. Oxford, UK: Blackwell;2005.p.10---22.
18.TsenLC,ThueB, DattaS,et al.Iscombinedspinal---epidural analgesiaassociatedwithmorerapidcervicaldilatationin nul-liparous patientswhen comparedwithconventional epidural analgesia.Anesthesiology.1999;91:920---5.
19.SchniderSM,AbboudTK,ArtalR,etal.Maternalcatecholamines decreaseduringlaborafterlumbarepiduralanesthesia.AmJ ObstetGynecol.1983;147:13---5.
20.SultanP,MurphyC,HalpernS,etal. Theeffectoflow con-centrationsversushighconcentrationsoflocalanestheticsfor labouranalgesiaonobstetricandanestheticoutcomes:a meta-analysis.CanJAnesth.2013;60:840---54.
21.NorrisMC,FogelST,ConwayC.Combinedspinal---epiduralversus epidurallaboranalgesia.Anesthesiology.2001;95:913---20. 22.Stacey RG, Poon A. Comparison of low dose epidural with
combinedspinal---epiduralanalgesiaforlabour.Br JAnaesth. 2000;84:695---8.
23.MiroM,GuaschE,GilsanzF.Comparisonofepiduralanalgesia withcombinedspinal---epiduralforlabor.IntJObstetAnesth. 2008;17:15---9.