REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Comparing
insertion
characteristics
on
nasogastric
tube
placement
by
using
GlideScope
TM
visualization
vs.
MacIntosh
laryngoscope
assistance
in
anaesthetized
and
intubated
patients
Wan
Hafsah
Wan
Ibadullah
a,
Nurlia
Yahya
a,∗,
Siti
Salmah
Ghazali
b,
Esa
Kamaruzaman
a,
Liu
Chian
Yong
a,
Adnan
Dan
a,
Jaafar
Md
Zain
aaDepartmentofAnaesthesiologyandIntensiveCare,UniversitiKebangsaanMalaysiaMedicalCentre,KualaLumpur,Malaysia
bDepartmentofAnaesthesiologyandIntensiveCare,HospitalKualaLumpur,KualaLumpur,Malaysia
Received10July2014;accepted11November2014 Availableonline20October2015
KEYWORDS
Nasogastrictube; Videolaryngoscope; Directlaryngoscope; Complications
Abstract
Backgroundandobjective: Thiswasaprospective,randomizedclinicalstudytocomparethe success rateof nasogastrictube insertionby using GlideScopeTM visualizationversus direct MacIntoshlaryngoscopeassistanceinanesthetizedandintubatedpatients.
Methods:Ninety-sixASAIorIIpatients,aged18---70yearswererecruitedandrandomizedinto twogroupsusingeithertechnique.Thetimetakenfrominsertionofthenasogastrictubefrom thenostriluntilthecalculatedlengthoftubehadbeeninsertedwasrecorded.Thesuccessrate ofnasogastrictubeinsertionwasevaluatedintermsofsuccessfulinsertioninthefirstattempt. Complicationsassociatedwiththeinsertiontechniqueswererecorded.
Results:Theresultsshowedsuccessratesof74.5%intheGlideScopeTMGroupascomparedto 58.3%intheMacIntoshGroup(p=0.10).Forthefailedattempts,thenasogastrictubewas suc-cessfullyinsertedinallcasesusingrescuetechniques.Thedurationtakeninthefirstattemptfor bothtechniqueswasnotstatisticallysignificant;GroupAwas17.2±9.3sascomparedtoGroup B,withadurationof18.9±13.0s(p=0.57).Atotalof33patientsdevelopedcomplications dur-inginsertionofthenasogastrictube,39.4%inGroupAand60.6%inGroupB(p=0.15).Themost commoncomplications,whichoccurred,werecoiling,followedbybleedingandkinking.
Conclusion: ThisstudyshowedthatusingtheGlideScopeTMtofacilitatenasogastrictube inser-tionwascomparabletotheuseoftheMacIntoshlaryngoscopeintermsofsuccessfulrateof insertionandcomplications.
©2015SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](N.Yahya).
http://dx.doi.org/10.1016/j.bjane.2014.11.013
PALAVRAS-CHAVE
Sondanasogástrica; Videolaringoscópio; Laringoscopiadireta; Complicac¸ões
Comparac¸ãodascaracterísticasdeinserc¸ãodesondanasogástrica,usando
visibilizac¸ãopelolaringoscópioGlideScope®vs.guiadapelolaringoscópioMacIntosh
empacientesanestesiadoseintubados
Resumo
Justificativaeobjetivo:Estefoiumestudoclínicoprospectivoerandômicoparacomparara taxadesucessodainserc¸ãodesondanasogástrica(NG)usandoastécnicasdevisibilizac¸ãopelo GlideScope®versusguiadapelolaringoscópioMacIntoshempacientesanestesiadoseintubados.
Métodos: Foramrecrutados96pacientes,ASAIouII,entre18-70anos,edivididos randomi-camente em dois grupos, com uma ou outra técnica. Foi calculado o tempo transcorrido desde a inserc¸ão da sonda NG, da narina até a inserc¸ão do comprimento calculado da sonda. A taxa de sucesso de inserc¸ão da sonda NG foi avaliada quanto à inserc¸ão bem-sucedida na primeira tentativa. As complicac¸ões associadas às técnicas de inserc¸ão foram registradas.
Resultados: Osresultadosmostraramtaxasdesucessode74,5%paraogrupoGlideScope®,me comparac¸ãocom58,3%paraogrupoMacIntosh(p=0,10).Paraastentativasquefalharam,a sondaNGfoiinseridacomsucessoemtodososcasos,usandoastécnicasderesgate.Adurac¸ão daprimeiratentativaparaambasastécnicasnãofoiestatisticamentesignificativa:17,2±9,3 segundosnoGrupo Ae18,9±13,0segundosnoGrupoB(p=0,57).Nototal,33pacientes desenvolveramcomplicac¸õesduranteainserc¸ãodasondaNG:39,4% noGrupo Ae60,6%no GrupoB (p =0,15). Ascomplicac¸ões maiscomunsocorridasforamenrolamento,seguidode sangramentoedobradura.
Conclusão:EsteestudomostrouqueousodoGlideScope® parafacilitarainserc¸ãodesonda nasogástrica foicomparávelao usodolaringoscópioMacIntosh quantoàtaxadesucesso de inserc¸ãoecomplicac¸ões.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Evenforthemostexperiencedanesthesiologist,the inser-tion of a nasogastric (NG) tube in anesthetized and tracheallyintubatedpatientscanbeverychallenging.1The
usual methodof insertion is by ‘blindly’inserting the NG tubewiththepatient’sheadinaneutralposition,whereby success rates have been reported to vary from 40% to 58%.2---4Varioustechniquesof NGtube insertionhave been
described, emphasizing the fact that as yet, there is no easy,simpleand safemethod.5Common methods usedto
facilitateNGtubeinsertionincludetheuseofa‘slit’ endo-tracheal tube as an introducer, forward displacement of thelarynx, useof a ureteralguide wire asastylet, head flexion, lateral neck pressure, placing the patient’s head inthelateralposition,freezingtheNGtube withdistilled water and the use of a gloved finger to steer the NG tube after impaction.2---4,6 It alsohas been suggested that
deflating the endotracheal tube (ETT) cuff will decrease esophageal compression and therefore facilitate insertion oftheNGtube.1However,none ofthesetechniques have
beenreportedtobeuniversallysuccessful.
Inadditiontothesemaneuvers,theuseof visualization-aidedmodalitieshasalsobeen advocatedtofacilitate NG tube insertion. The GlideScopeTM videolaryngoscope is a
reusable device that consists of a handle and a blade. Althoughthehandleissimilartothatofastandard laryngo-scope,theblade isdifferentbecauseitisnotdetachable,
hasamaximumwidthof26mmatanypoint,andhasa60◦
curvature in the midline. It includes an integrated CMOS camera;anLEDlightsource,apatentedantifogging mech-anismandreusable,medical-graderobustplasticshell.The image capturedby thecamerais displayedona7-in. liq-uidcrystaldisplaycolormonitor.Althoughacknowledgedas an effective device used for tracheal intubation,7,8 there
are few studies done to assess the effectiveness of the GlideScopeTM in facilitating NG tube insertion and only a
fewreportsmentioning itsusefulnessindoingso.5,9,10 The
GlideScopeTMalsohasbeenreportedtoaidintheinsertion
ofatransesophagealechocardiographyprobewhenallother placementmethodshavefailed.11
Studies have shown that the GlideScopeTM provides
an improved view of the larynx as compared to direct laryngoscopy.7,8Oesophagealopeningvisualizationbyusing
theMacIntoshlaryngoscopeisalsonotoptimumascompared totheuseoftheGlideScopeTM.Hence,insertionoftheNG
tubeunderdirectvisionusingavideolaryngoscopemay pro-videreal-timeview,shouldhelpimprovespeedofinsertion andpotentiallyreducecomplications.
AstudybyMohararietal.1showedthattheGlideScopeTM
could be a safe and effective aid for NG tube insertion in anesthetized and intubated patients by improving the easeofinsertionwithasuccess rateof85%.However,the study comparedtheconventional ‘blindtechnique’versus GlideScopeTMassistance,whichprovidesadirectview
NasogastrictubeinsertionusingGlideScope vs.MacIntoshlaryngoscopy 365
insertioncharacteristicsonnasogastrictube placementby usingGlideScopeTM visualization versusMacIntosh
laryngo-scope assistance withregards tofirst successful attempt, rescueattemptsandcomplicationsinanesthetizedand intu-batedpatients.
Materials
and
methods
Thisprospective,randomized,single-blindedclinicalstudy wasconductedafterobtaininginstitutionalethicsapproval fromtheMedicalResearchand EthicsCommittee, Univer-siti KebangsaanMalaysiaMedicalCentre(UKMMC) (Project code: FF-199-2012) and the Clinical Research Committee ofMinistryofHealthMalaysia(NMRR-12-1010-12540).After obtaining written informed consent,a total of 96 Ameri-canSociety ofAnesthesiologists(ASA)IorII patientsaged between18and70years,scheduledforsurgeryunder gen-eralanesthesiarequiring trachealintubation andNGtube insertion were recruited into this study. Those excluded fromthestudywerepatientswithknownbasalskull frac-ture, hemorrhagic disorders, esophageal diseases such as stricture,varicesorstenosis,historyofradiotherapytothe headandneckandobesitywithabodymassindex(BMI)of morethan35kg/m2.Preoperatively,patientswere
random-ized using computer-generated randomized numbers into twogroups.Themorepatentnostrilwasselectedbasedon twocriteria, theamount of foggingproduced on a metal tonguedepressorduringexhalationandtherelativesizeof thenostril.Thenostrilthatwasbiggerandproducedmore fogwaschosen. Allpatientswerepremedicatedwithoral midazolam7.5mgonthenightbeforesurgery.
Intravenousaccess(IV)wasestablishedintheoperating theater. Standard monitoring with continuous electrocar-diography, non-invasive blood pressure monitoring, pulse oximetry and capnographwere usedfor all patients. Fol-lowingpreoxygenation,inductionofanesthesiawascarried outusingIVpropofol2mg/kg,IVfentanyl2mcg/kgandIV rocuronium 0.9mg/kg. Patients were given assisted ven-tilation via facemask for 3min following which direct laryngoscopyperformed.Thepatientswereintubatedwith a size 7.5mm (for female) or 8.0mm (for male) internal diameter,polyvinylchlorideendotracheal tube(ETT).The ETTcuffwasinflatedandthepressurekeptbetween15and 25cm H2O using apressure gauge manometer. Anesthesia
wasmaintainedbyoxygen/air(50%/50%)andsevofluraneat aminimumalveolarconcentrationof1.
Multiple operators consisting of anesthesia medical officers, who were proficient in both techniques, were responsiblefortheNGtubeinsertions.InGroupApatients, thebladeoftheGlideScopeTMwasinsertedintothepatient’s
mouth, the tracheal tube and tongue were lifted to pro-videtheanesthetistwiththebestviewofthelaryngealarea whichwasvisualizedonthedisplaycolormonitor andthe NGtube wasadvanced.In Group Bpatients,the bladeof theMacIntoshlaryngoscopewasinsertedintothepatient’s mouth, the tracheal tube and tongue were lifted to pro-vide the anesthetist with the best view of the laryngeal area,visualized orally and theNG tube wasadvanced. In bothgroups,thepatient’sheadwasmaintainedinthe neu-tralpositionand thebladeswere liftedgently toprevent excessiveextensionoftheneck.
Inallpatientgroups,a14Frenchgauge(FG),125cmNG tube(ForesightIndustriesSdnBhd,Selangor,Malaysia)with leadwasused.The length ofNGtube necessary to reach thestomachwasassessedbeforeinsertionandmeasuredby placingthetipoftheNGtubeonthepatient’sxiphoid pro-cessandextendingittothetipofhis/hernoseandoverthe earlobe.Immediatelybeforeinsertion,KYjellywasapplied ontheselectedpatient’snostril.Ineachgroup,theNGtube waspassed via the patient’s nostril posteriorly along the floorofthenoseandtubewasadvancedtoreachthe mea-suredlength.AsuccessfulNGtubeinsertionwasdefinedas thesuccessfulpassageoftheNGtubeinthefirstattempt andconfirmed whenthe tubepassed smoothly anda gur-glingsoundwasheardonauscultationovertheepigastrium wheninjecting10mLofairthroughtheNGtube.Inthefirst attempt,noassistingdevicewasusedinbothgroups.Ifthe NGtubewasnotsuccessfullyinserted,itwasdeemedasa proceduralfailureandrecordedasafailedattempt.TheNG tube waswithdrawn fully and cleaned. Subsequently res-cue techniques were implemented to insert the NG tube untilitwassuccessfullyinserted. Rescuetechniques com-prisedof second attempt andswitch-over technique. The sameNGtube wasusedin thesecond attempt, this time withtheassistanceofaMagill’sforceps.Ifthattoofailed, theNGtubewasreinsertedswitchingoverthe2techniques whileusingtheassistanceofaMagill’sforceps.InGroupA, theMacIntoshlaryngoscope wasusedandinGroup B,the GlideScopeTMwasusedinsteadtoinserttheNGtube(refer
toFig.1forthestudyflowchart).
No assisting device
Success xx
Fail Success
Success
Fail
Fail Fail
Group A Use GlideScopeTM
Group B
Use macintosh laryngoscope Randomization
No assisting device
Success
Use magill forcep
Use macintosh laryngoscope
Use magill forcep
Success Fail Success Fail
Failed use rescue technique
Switch-over technique
Inclusion
Use GlideScopeTM
Thedurationrequiredforplacementwastakenfromthe timewhenthetubewasadvancedintothenostriluntilthe measuredlengthofthetubehadbeeninserted.Ageneral anesthesiaassistant measured the timetaken using stop-watch.The occurrenceof complicationssuchasbleeding, kinking and coiling during the procedure was noted. The rateofsuccessfulNGtubeinsertionandthedurationneeded forsuccessfulinsertiononthefirstattemptwascompared betweenthe2groups.
All data were recorded and analyzed using SPSS ver-sion 21.0 software. Normal distribution of continuous data was tested by the Kolmogorov---Smirnov test. Non-parametricdata(gender,race,ASA,intubationattemptand complications) were analyzed using the Chi-square test. Independent T-test was used to analyze parametric data (age,height, weight,BMIand durationof insertion).A p -value of less than 0.05 was considered to bestatistically significant.
Results
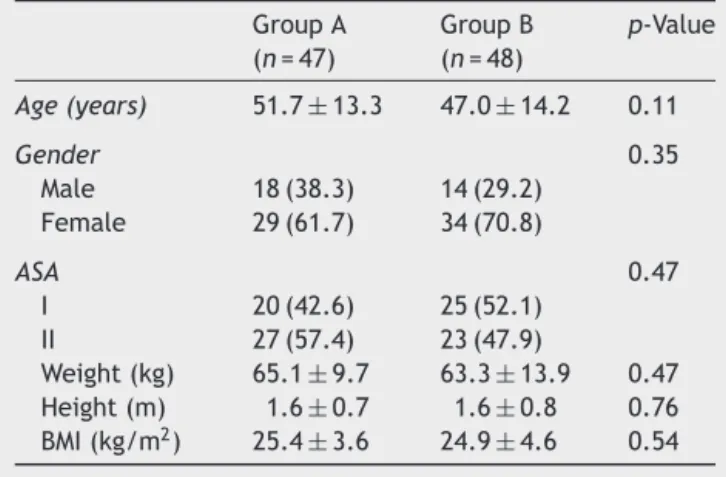
Atotal of 96 patients were enrolledbut only 95 patients wereincluded,asonepatientfromGroup A,whoinitially consented to participatein the study, refused surgery on thedayofoperation.Forty-sevenpatientswereenrolledin GroupAand48patientsinGroupB.Thedemographicdata isshowninTable1.Thedemographicdatawascomparable betweenbothgroups.
Table2showssuccessfulinsertionsoftheNGtubeduring thefirstattemptandrescuetechniques.The NGtube was ultimatelyinsertedinallpatients.
The mean time for duration of insertion in the first attempt for Group A was 17.2±9.3s and for Group B
Table1 Demographicdata,valuesexpressedasmean±SD
ornumbern(%)whereappropriate. GroupA (n=47)
GroupB (n=48)
p-Value
Age(years) 51.7±13.3 47.0±14.2 0.11
Gender 0.35
Male 18(38.3) 14(29.2) Female 29(61.7) 34(70.8)
ASA 0.47
I 20(42.6) 25(52.1)
II 27(57.4) 23(47.9)
Weight(kg) 65.1±9.7 63.3±13.9 0.47 Height(m) 1.6±0.7 1.6±0.8 0.76 BMI(kg/m2) 25.4±3.6 24.9±4.6 0.54
Table 2 Success rates of NG tube insertion, values
expressedasnumbern(%). Attempts GroupA
(n=47)
GroupB (n=48)
p-Value
1stattempt 35(74.5) 28(58.3) 0.10 Secondattempt 11(23.4) 18(37.5) 0.55 Switch-over 1(2.1) 2(4.2) 1.00
was18.9±13.0s(p=0.57).Thirty-threepatientsdeveloped complicationsduringinsertionoftheNGtube, 13patients (39.4%) in Group A and 20 patients (60.6%) in Group B (p=0.15).
The complications werefurther categorizedtocoiling, kinkingandbleeding.Elevenpatients(23.4%)inGroupAand 17patients(35.4%)inGroupBdevelopedcoiling(p=1.00). Bleeding occurred in 4 patients (8.5%) in Group A and 5 patients (10.4%)in GroupB(p=1.00). Kinkingoccurred in 2patients(4.3%)inGroupAand1patient(2.1%)inGroupB (p=0.55).OnepatientinGroupAhadaccidentalmalposition oftheNGtubeintothetrachea.Percentageofcomplications thatwascalculatedreflectstheoccurrenceofcomplications inallattemptscollectively.Onepatientmayalsohavehad morethanonecomplicationoccurringduringtheinsertion procedure.
Discussion
Ourstudywasdesignedtocomparedirectvisualization tech-niques using two different intubation devices to assist in nasogastric tube insertion. Wefound that thereappeared tobeahighersuccessrateinGroupAcomparedtoGroup B,74.5%vs.58.3%,althoughthiswasnotstatistically signif-icant.Alargersamplesizewouldmostprobablyberequired tolookforasignificantstatisticaldifferenceinthesuccess rateofinsertion.
Ourstudyshowedthattherewasnosignificantdifference inthedurationofinsertionbetweenthese2groups.Astudy donebyMohararietal.1showedashorterdurationof
inser-tionintheGlideScopeTMgroup(10.9
±9.0s)ascomparedto the‘blind’insertiontechniquegroup(38.6±29.0s).Afew previous studies comparing the conventional‘blind’ tech-niqueandvariousothertechniquesofinsertionshowedthat thedurationofNGtubeinsertionusingthe‘blind’technique tookbetween39.5sand124sforsuccessfulinsertion.2,4,12
Hence,directvisualizationtechniquesmayimproveNGtube insertionspeed.Infuturestudieshowever,itwouldperhaps bebettertoincludea‘blind’techniquegrouptoallow bet-tercomparison betweennewtechniques of insertionwith theconventionalmethod,toassessspeedofNGtube inser-tion.
However,in the rescue second attempt, there were a higherpercentageofpatientsinGroupBwhohadsuccessful insertionoftheNGtubealthoughthiswasnotstatistically significant.Thiscanbeexplainedbythedifficultyin manip-ulatingtheMagill’sforcepsinGroup Apatientsduetothe bulkinessoftheGlideScopeTMbladeallowinglimitedspace
tomovetheMagill’sforcepsorallyascomparedtotheuse oftheMacIntoshblade.
Themostcommoncomplicationinthisstudywascoiling. Elevenpatients(23.4%)inGroupAand17patients(35.4%) inGroupBdevelopedcoiling.Thepiriformsinusesandthe arytenoidcartilagesarethemostcommonsitesofimpaction ofaNGtube duringinsertion.2Ithasbeen suggestedthat
compressionoftheipsilateralneckatthelevelandlateral border of the thyrohyoid membrane canbe performed to collapsetheipsilateralpiriformfossaandslightlymovethe arytenoids cartilagesothat NGtube canpass throughvia thelateralorposteriorhypopharynx.13Other
NasogastrictubeinsertionusingGlideScope vs.MacIntoshlaryngoscopy 367
flexionwithlateralpressure (82%success rate inthe first attempt),2usingneckflexion(80%successrateinthefirst
attempt),3headturnedtothelateralposition(80%success
rateinthefirstattempt),5andliftingthethyroidcartilage
(68.8% success rate in the first attempt).14 However, for
patients withcervicalinstability, these techniques cannot beused.Agroetal.15demonstratedthattheGlideScopeTM
provided a better vision of the glottis compared to the MacIntoshlaryngoscopeincervicalspineimmobilization.In anotherstudy,Maliketal.12 alsoshowedthatalthoughthe
GlideScopeTMrequiredmoretimefortrachealintubation,it
reducedintubationdifficultyandimprovedglotticviewover theMacIntoshlaryngoscopeinpatientswithcervicalspine immobilization. Thus using the GlideScopeTM for NG tube
insertionwouldalsobebeneficialincaseswhere manipula-tionoftheneckislimited.
Another complication observed was bleeding from mucosalsurface. However,therewasnostatistical differ-enceinbothgroups.Noneofthesepatientsneededfurther medicaltreatment. Itwasobserved thatthebleedingwas mostly fromthe nostril and nasopharynx areaand proba-blyoccurredduetotraumafromthetipofNGtubeduring insertionratherthantraumacausedfromthevarious tech-niquesitself.Inordertolessentheoccurrenceofbleeding, some studies preparedthe patient’s nostril with vasocon-strictors(suchasphenylephrineoroxymetazoline)priorto NGtubeinsertion.1,3Inourstudy,wedidnotuseany
vaso-constrictorstopreparethepatient’snostril.Appukuttyand Shroff2usedaslitETTorallytoassistininsertionoftheNG
tubeandreportedahighsuccessrateinthefirstinsertion attemptusingthistechnique.However,therewasincreased risk ofbleeding(22%) withthis techniqueascomparedto othertechniquesusedinthestudy.
AlthoughNGtubeinsertionisconsideredacommon clini-calprocedure,itcanproduceunexpectedcomplications.In ourstudy,therewasaninadvertent,accidentalplacement oftheNGtubeintothetracheaofonepatientinGroupA. This wasevidenced by bubblingof waterwhen the proxi-maltipoftheNGtubewasimmersedinagallipotofwater. The NGtube washowever,successfully inserted usingthe rescuetechnique.Rassias etal.16 reporteda 2%incidence
oftracheopulmonarycomplicationssuchaspneumothorax, hydrothoraxor hemorrhageamong740NGtube insertions whereby 0.3% of patients died from thesecomplications. Pillaietal.17suggestedthatthepresenceoftheETTmight
actuallyincreasetheriskofpulmonaryentryoftheNGtube duetopreventionofglotticclosure.ApreexistingETTmay distort the anatomy of the laryngeal opening due to the presenceoftheETTcuffexpandingtheglotticopening lead-ingtoanincreasedriskofnasoenteraltubemalpositionand complications.17ThetechniqueofdeflatingETTcuffbefore
insertionoftheNGtubewouldbehelpfulinincreasingthe success rate of insertion asshown in studies by Moharari etal.1andLaietal.5althoughbydoingso,mayleadtothe
potentialrisk ofaspirationwhenthe ETTcuffis deflated. However,none ofthesestudiesreportedaspirationasone ofthecomplications.
TheuseoftheMacIntoshlaryngoscopewithassistanceof theMagill forcepsis theconventional rescuetechniquein theinstitutionwherethisstudywascarriedout.This tech-niquealsohasbeenusedastherescuetechniqueinmostof thestudies involvingNGtube insertion.1---3,14 However,the
GlideScopeTMassistancetechniquemaybeusedasthe
res-cuetechniqueofchoicewhenothermethodshavefailedas evidenced by the high success rate of insertion usingthe GlideScopeTMasshowninthestudybyMohararietal.1and
otherpreviouscasereports.5,9,10
There werea few limitations in thisstudy. Firstly,the potential for investigator bias exist asit is impossible to blind the anesthetists tothe device being used. Further-more,multipleoperatorswereinvolvedininsertingNGtube. Therefore,therewillalsobeskillbiasinthisstudy.Astudy byMatheison18whichincludedattendinganesthesiologists,
anesthesiologistfellowsand respiratorytherapistsshowed thatafter30 intubationattempts usingthe GlideScopeTM,
success rates of intubation were high (94.2%).Therefore, to reduce skill bias in future studies; it can be recom-mendedthatatleast30previous NGtubeinsertionsusing theGlideScopeTMbytheinvestigatorswouldberequiredto
gainexpertisewithitsuse.
TheGlideScopeTMhasbeenusedwidelyindifficult
intu-bationcases.Howeverforethicalreasons,casesofdifficult NGtubeinsertionduetodifficultairwaysandobesepatients were excluded from this study. Therefore, results in our study would not reflect the outcome in these groups of patients.TheadvantageofusingtheGlideScopeTMcompared
tousingtheMacIntoshbladeisthatitdoesnotrequirea line-of-sightviewfromtheoperatortotheesophagealopening. As it has been shown to beadvantageous in difficult air-waysituations,furtherstudiesusingtheGlideScopeTMmay
berecommended tofacilitate NGtube insertionin obese patientsandthosewithpotentialdifficultairwaysand cer-vicalinstability.Inconclusion,thisstudyshowedthatusing theGlideScopeTMtofacilitatenasogastrictubeinsertionwas
comparable to the use of the MacIntosh laryngoscope in termsofsuccessfulrateofinsertionandcomplications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MoharariRZ, FallahAH, KhavajiMR, etal. TheGlideScope®
facilitates nasogastric tube insertion: a randomized clinical trial.AnesthAnalg.2010;110:115---8.
2.Appukutty J,Shroff PP. Nasogastrictube insertion using dif-ferent techniques in anaesthetized patients: a prospective, randomizedstudy.AnesthAnalg.2009;109:832---5.
3.MahajanR,GuptaR,SharmaA.Roleofneckflexionin facilitat-ingnasogastrictubeinsertion.Anesthesiology.2005;103:446---7.
4.BongCL,MacachorJD,HwangNC.Insertionofthenasogastric madeeasy.Anesthesiology.2004;101:266.
5.LaiHY,WangK,YangYL,etal.Facilitatedinsertionofa nasogas-trictubeintrachealintubatedpatientsusingtheGlideScope®.
BrJAnaesth.2006;97:749---50.
6.Fakhari S, Bilehjani E, NegargarS, et al. Split endotracheal tube as a guide for gastric tube insertion in anaesthetized patients:arandomizedclinicaltrial.JCardiovascThoracRes. 2009;1:17---22.
7.RaiMR,DeringA,VergheseC.TheGlideScope®system:a
clini-calassessmentofperformance.Anaesthesia.2005;60:60---4.
8.CooperRM,PaceyJA,BishopMJ,etal.Earlyclinicalexperience withanewvideolaryngoscope(GlideScope®) in728patients.
9.HunterCW,CohenS.AnewusefortheGlideScope®.Anesth
Analg.2006;103:509.
10.PandianA,RavalM,BaileyCR.Anonairwaymanagementuse ofthevideolaryngoscope(GlideScope®).EurJAnaesthesiol.
2008;25:511.
11.St.LaurentC,WongD,KudrickN,etal.TheGlideScope®:also
helpfulwithdifficulttransesophagealechocardiographyprobe placement.AnesthAnalg.2007;104:1004---5.
12.Malik MA, Maharaj CH, Haste BH, et al. Comparison with Macintosh, Truview EVO2®, Glidescope® and Airwayscope®
laryngoscopeuseinpatientswithcervicalspineimmobilization. BrJAnaesth.2008;10:723---30.
13.TsaiYF,LuoCF,IlliasA,etal.Nasogastrictubeinsertionin anes-thetizedandintubatedpatients;anewandreliablemethod. BMCGastroenterol.2012;12:99.
14.Kirtania J, Ghose T, Garai D, et al. Esophageal guidewire assistednasogastrictubeinsertioninanaesthetizedand intu-bated patients: a prospective randomized controlled study. AnesthAnalg.2012;114:343---8.
15.Agro F, Barzoi G, Montecchia F.Tracheal intubation using a MacIntoshlaryngoscopeoraGlideScope® in15patientswith
cervicalspineimmobilization.BrJAnaesth.2003;90:705---6.
16.Rassias AJ, Ball PA, Corwin HL. A prospective study of tra-cheopulmonarycomplicationsassociatedwiththeplacementof narrow-boreenteralfeedingtubes.CritCare.1998;2:25---8.
17.PillaiJB,VegasA,BristerS.Thoraciccomplicationsof nasogas-trictube:reviewofsafepractice.InteractCardiovascThorac Surg.2005;4:429---33.