REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Rectal
dexmedetomidine
in
rats:
evaluation
of
sedative
and
mucosal
effects
Volkan
Hanci
a,∗,
Kanat
Gülle
b,
Kemal
Karakaya
c,
Serhan
Yurtlu
a,
Meryem
Akpolat
b,
Mehmet
Fatih
Yüce
d,
Fatma
Zehra
Yüce
b,
Is
¸ıl
Özkoc
¸ak
Turan
daDepartmentofAnesthesiologyandReanimation,DokuzEylulUniversity,SchoolofMedicine,Izmir,Turkey
bDepartmentofHistologyandEmbryology,ZonguldakBulentEcevitUniversity,SchoolofMedicine,Zonguldak,Turkey cDepartmentofGeneralSurgery,ZonguldakBulentEcevitUniversity,SchoolofMedicine,Zonguldak,Turkey
dDepartmentofAnesthesiologyandReanimation,ZonguldakBulentEcevitUniversity,SchoolofMedicine,Zonguldak,Turkey
Received1July2013;accepted9September2013 Availableonline5November2013
KEYWORDS Dexmedetomidine; Rectum;
Rat; Anesthesia; Mucosa
Abstract
Backgroundandobjectives: Inthisstudy,weinvestigatedtheanestheticandmucosaleffects oftherectalapplicationofdexmedetomidinetorats.
Methods:Male Wistar albino ratsweighing 250---300g were dividedinto four groups: Group S (n=8) wasa sham groupthat served asabaseline for the normalbasal values; Group C (n=8)consistedofratsthatreceivedtherectalapplicationofsalinealone;GroupIPDex(n=8) includedratsthatreceivedtheintraperitonealapplicationofdexmedetomidine(100gkg−1);
andGroupRecDex(n=8)includedratsthatreceivedtherectalapplicationofdexmedetomidine (100gkg−1).Fortherectaldrugadministration,weused22Gintravenouscannulaswiththe
styletsremoved.Weadministeredthedrugsbyadvancingthecannula1cmintotherectum,and therectaladministrationvolumewas1mLforalltherats.Thelatencyandanesthesiatime(min) weremeasured.Twohoursafterrectaladministration,75mgkg−1ketaminewasadministered forintraperitonealanesthesiainallthegroups,followedbytheremovaloftherats’rectums toadistaldistanceof3cmviaanabdominoperinealsurgicalprocedure.Wehistopathologically examinedandscoredtherectums.
Results:AnesthesiawasachievedinalltheratsintheGroupRecDexfollowingthe adminis-tration ofdexmedetomidine. TheonsetofanesthesiaintheGroup RecDexwassignificantly laterandofashorterdurationthanintheGroupIPDEx(p<0.05).IntheGroupRecDex,the administrationofdexmedetomidineinducedmild---moderatelossesofmucosalarchitecturein thecolonandrectum,2hafterrectalinoculation.
Conclusion: Although100gkg−1dexmedetomidine administeredrectallytoratsachieveda
significantlylongerdurationofanesthesiacomparedwiththerectaladministrationofsaline,our
∗Correspondingauthor.
E-mails:[email protected],[email protected](V.Hanci).
histopathologicalevaluationsshowedthattherectaladministrationof100gkg−1
dexmedeto-midineledtomild---moderatedamagetothemucosalstructureoftherectum.
©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
PALAVRAS-CHAVE Dexmedetomidina; Reto;
Rato; Anestesia; Mucosa
Dexmedetomidinaretalemratos:avaliac¸ãodosefeitossedativosesobreamucosa
Resumo
Justificativaeobjetivos: Nesteestudonósinvestigamososefeitosanestésicosesobreamucosa daaplicac¸ãoretaldedexmedetomidinaaratos.
Métodos: RatosmachosalbinosWistar,pesando250-300g,foramdivididosemquatrogrupos: GrupoS(n=8)foium gruposhamqueserviudebasepara osvaloresbasaisnormais; Grupo C(n=8)consistiuemratosquereceberamaaplicac¸ãoretalapenasdesorofisiológico;Grupo IPDex(n=8) consistiuem ratosquereceberamaplicac¸ãointraperitonealde dexmedetomid-ina(100gkg−1)eGrupoRecDex(n=8)consistiuemratosquereceberamaaplicac¸ãoretal
dedexmedetomidina(100gkg−1).Paraaadministrac¸ãodosfármacosporviaretal,usamos
cânulasintravenosasdecalibre22,comosestiletesremovidos.Aadministrac¸ãoconsistiuem avanc¸aracânula1cmnoreto,eovolumedeadministrac¸ãoretalfoide1mLparatodososratos. Ostempos(min)delatênciaedeanestesiaforamregistrados.Duashorasapósaadministrac¸ão porviaretal,75mgkg−1decetaminaforamadministradosatodososgrupospara anestesia intraperitoneal,seguidoporremoc¸ãodosretosdosratosaumadistância3cmdistalpormeio deprocedimentocirúrgicoabdominoperineal.Osretosforamhistopatologicamenteexaminados eclassificados.
Resultados: AanestesiafoirealizadaemtodososratosdogrupoRecDexapósaadministrac¸ão dedexmedetomidina.OtempodeiníciodaanestesianoGrupoRecDexfoisignificativamente maislongoecomumadurac¸ãomaiscurtaquenoGrupoIPDEx(p<0,05).NoGrupoRecDex,a administrac¸ãodedexmedetomidinainduziuperdaslevesamoderadasdaarquiteturadamucosa docólonereto2hapósainoculac¸ãoretal.
Conclusão:Emboraaadministrac¸ãode100gkg−1dedexmedetomidinaporviaretalemratos
tenharesultadoemumadurac¸ãosignificativamentemaiordaanestesia,emcomparac¸ãocom aadministrac¸ãoretaldesorofisiológico,nossasavaliac¸õeshistopatológicasmostraramquea administrac¸ãoretalde100gkg−1dedexmedetomidinaocasionoudanoslevesamoderadosà
estruturadamucosaretal.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Premedicationisthepreoperativenasal,oral,rectal, intra-muscularorintravenousadministrationofsedativedrugsto lower the patient’s fear of surgical intervention, achieve sedationandanxiolysis,anddecreasetheamountof anes-thetics needed.1---6 In addition tobenzodiazepines such as
midazolam,whicharecommonlyusedforthispurpose,the
useof alpha2 agonists suchasclonidine and
dexmedeto-midineisbecomingpopular.3---8Forpediatricpatients,itis
essentialthatpremedicationagentsareadministered
non-invasively,i.e.,transmucosally,nasallyororally.3---5,7,8Rectal
administrationis also preferred,particularly for the
pre-medicationof young children.2,3,9---11 Previousstudies have
shownthat,similartomidazolamandketamine,clonidine
canbeadministeredrectallyforpremedication.2,9---14
Dexmedetomidine is an alpha adrenergic agonist with
highlevels ofspecificity andselectivity toalpha 2
recep-tors.Dexmedetomidinecanbeusedforsedation,analgesia
and anesthesia in intensive care settings, as well as for
local and regional anesthesia applications.8,15---17 Research
has also shown that dexmedetomidine can be
adminis-teredorally,nasally,transmucosallyor intramuscularlyfor
premedication.4,8,18---24 However, there are no published
studiesconcerningtherectalapplicationof
dexmedetomi-dineforpremedication.
Ourhypothesiswasthatdexmedetomidineadministered
rectally to rats would produce a sedative effect with no
damagetotherectalmucosa.
To test this hypothesis, we compared the anesthetic
effects of equal doses of dexmedetomidine administered
rectally or intraperitoneallytorats. In addition,we
com-pared the histopathological effects on rectal mucosa of
rectallyadministereddexmedetomidine.
Materials
and
methods
This study wasapproved by the Animal EthicsCommittee
oftheBulentEcevitUniversity(formerlyZonguldak
Karael-masUniversity)MedicalSchool.Alltheanimalsweretreated
theuniversity’sanimalcarecommitteeandtheprinciplesof
laboratoryanimal care(NIHpublicationno.85-23,revised
in1985).Theratswerehousedinatemperature-controlled
room(24±1◦C)ona12-hlight---12-hdarkcycle,andthey
werefedstandardratchowandwateruntil12hbeforethe
experimentalprotocol.
Thirty-twomaleWistaralbinoratsweighingbetween250
and300gwererandomlydividedintofourgroups ofeight
rats. Group S (n=8) wasa sham group served asa
base-line forthenormal basalvalues;GroupC (n=8) consisted
of rats that received the rectal application of saline
alone;Group IPDex(n=8)included rats thatreceived the
intraperitonealapplicationofdexmedetomidine;andGroup
RecDex(n=8)includedratsthatreceivedtherectal
appli-cationofdexmedetomidine.
The rats’ weights were measured prior to the
exper-iment. For rectal drug administration, we used 22G
intravenouscannulaswiththestyletsremoved.We
admin-istered the drugs by advancing thecannula 1cm into the
rectum,andtherectaladministrationvolumewas1mLfor
alltherats.25
We identified the onset and duration of anesthesia in
allthe groupsby observingthe righting reflex.26 We
mea-suredthelatencyofanesthesia(thetimerequiredtolose
therighting reflex)and theanesthesiatime(the duration
of theloss of the righting reflex)in minutes(min).26 Two hours after rectal study drug’s administration; 75mgkg−1
ketaminewasusedinallthegroupsforintraperitoneal
anes-thesia, followed by the removal of the rats’ rectums to
adistal distanceof 3cmvia an abdominoperinealsurgical
procedure.25 We histopathologically examined and scored
therectums.27
Preliminarystudy
Before the experiment, we evaluated the effectiveness
of different dosesof rectally administered
dexmedetomi-dinefrompreviousstudies.16,17,28Weadministered1
gkg−1,
10gkg−1, 50gkg−1 and 100gkg−1 dexmedetomidine
rectallytothetworatsineachgroup.25Inthepreliminary
study,anesthesiawasnotachievedwiththerectal
admin-istration of 1 or 10gkg−1 dexmedetomidine; however,
anesthesia wasobtained in one of the rats that received
50gkg−1dexmedetomidine rectallyandinbothrats that
received100gkg−1dexmedetomidinerectally.Therefore,
100gkg−1waschosenasthedoseofdexmedetomidineto
beusedrectallyandintraperitoneally.
Groups
Theratsintheshamgroup(n=8)didnotreceive the
rec-taladministrationofanysubstances.Theseratswereused
as controls for the histopathological examination of the
rectum.Theywereadministered75mgkg−1i.p.ketamine,
followedbytheremovaloftherectumtoadistaldistanceof
3cmviaabdominoperinealsurgery.25Weexaminedtherats’
rectumsandscoredthemhistopathologically.27
The rats in the control group (n=8) received 1mL of
saline by the advancementof a 22G intravenous cannula
withnostylet1cmintotherectum.Afterthesaline
admin-istration,wemeasuredtheanesthesiadurationintherats.26
Weremovedtheirrectums toa distaldistanceof 3cmvia
abdominoperinealsurgery.26Weexaminedtherectumsand
scoredthemhistopathologically.27
We administered 100gkg−1 dexmedetomidine
intraperitoneally to the rats in group IPDex
(intraperi-tonealdexmedetomidine group,n=8).Weestablishedthe
proper dosage of dexmedetomidine with the help of the
preliminary study and previous research.16,17,28 After the
administration of dexmedetomidine, we measured the
anesthesiadurationintherats.26
In the rectal dexmedetomidine group (Group RecDex,
n=8),salinewasaddedto100gkg−1dexmedetomidineto
a total volume of 1mL and was administered rectally by
advancinga22Gintravenouscannulawithnostylet1cminto
therectum.Afteradministeringthedexmedetomidine,we
measuredtheanesthesiadurationintherats.26Therectums
ofthe ratswere removed toa distaldistance of 3cm via
abdominoperineal surgery.25 The rectums were examined
histopathologicallyandscored.27
Histologicassessmentofcolonicmucosaldamage
Forthe light microscopic observation, distal colon
speci-mens wereembedded in paraffin blocksafter being fixed
ina10%formalinsolution.Five-micrometer(5-m)sections
wereobtainedandstainedwithhematoxylin---eosinand
Mas-son’strichromeusingstandardmethods.Ahistologistgraded
thecolonicpathologicalchangesinablindedmannerusing
the histologicinjury scale previously developed by Leung
etal.27 Briefly, mucosal damage wasgraded from 0 to 4
accordingtothefollowingcriteria:grade0,normalmucosa;
grade1,damagetothe surfaceepitheliumonly; grade2,
damagetotheepithelium ofthe upperhalf ofthe gland;
grade3,damage tothe majorityof the glandular
epithe-liumthatdidnotextendtothebaseofthegland;andgrade
4,thedestructionoftheepitheliumoftheentiregland.
Statisticalanalysis
Weperformedthestatisticalanalysiswasusingthe
Statis-tical Package for the Social Sciences (SPSS) version 16.0
for Windows (SPSS,Chicago, IL). Forthe scores and
non-normally distributed variables, we compared the groups
using the Mann---Whitney U and Kruskal---Wallis tests. The
resultswereexpressedasmedians(25th---75thpercentiles). Apvalue<0.05wasconsideredstatisticallysignificant.
Results
Resultsconcerningthedurationofanesthesiaandtherectal
histopathologicalevaluationswereobtained.
Durationofanesthesia
Weachievedanesthesiainalltheratsintheintraperitoneal
andrectal dexmedetomidine groups following the
admin-istrationof dexmedetomidine (p<0.001).Inboth ofthese
groups,thedurationofanesthesiawassignificantlylonger
thanintheshamandcontrolgroups(p<0.001).IntheGroup
Table1 Latencyofanesthesiaandanesthesiatimevaluesaccordingtogroup(median[25th---75thpercentiles]). GroupS
(n=8)
Group C(n=8)
GroupRecDex(n=8) GroupIPDex(n=8) p
Latencyofanesthesia(min) 0(0-0) 0(0-0) 13.50(11.25---15.75)a,b,c 8.5(5---9.75)a,b 0.001
Anesthesiatime(min) 0(0-0) 0(0-0) 62.50(47.00---79.00)a,b,c 111.5(96---115.0)a,b 0.001
Min:minute.
ap<0.001comparedtoGroupS;Mann---WhitneyUtest. b p<0.001comparedtoGroupC;Mann---WhitneyUtest. c p<0.001comparedtoGroupIPDex;Mann---WhitneyUtest.
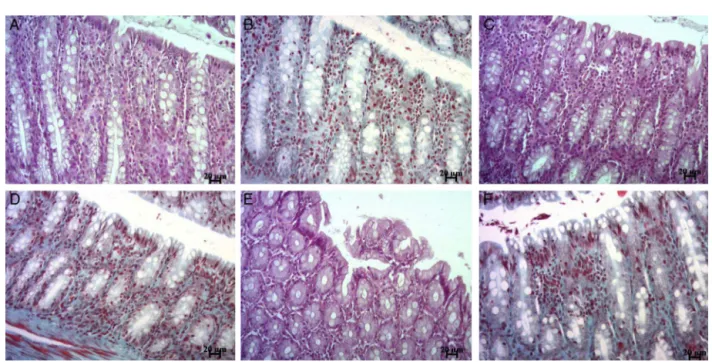
Figure1 Representativemicrographsofratcolonsectionsstainedwithhematoxylin---eosin(A,C,E)orMasson’strichrome(B, D,F).NormalcolonicmucosaofGroupSandGroupCrats(A---D).Ratstreatedwithrectaldexmedetomidine,showingthemildto moderatelossofsurfaceandglandularepithelialcells(E,F).Scalebar=20m.
rapidlythanintheGroupRecDex(p<0.001).Incontrast,the
durationofanesthesiaintheGroupIPDexwassignificantly
longerthanintheGroupRecDex(p<0.001)(Table1).
Histopathologicalfindings
The histologic featuresof the colonicand rectal walls of
theSham andControl groups weredeterminedtobe
nor-mal (Fig. 1A---D). In the Group RecDex, the drug induced
mildandmoderatelossesofthemucosalarchitectureinthe
colonandrectum,2h afterrectalinoculation(Fig.1E---F).
The histological examinationsdemonstrated the presence
ofmucosaldamagewiththe lossofsurface andglandular
epithelialcells.AsshowninTable1,themicroscopicscore
(2[2-2])of thecolonsfromtheGroupRecDexwas
signifi-cantlyhigherthanthat ofthecolonand rectumsegments
fromtheshamandcontrolrats(p<0.001)(Table2).
Discussion
In this study, rectaldexmedetomidine administrationwas
showntohaveanestheticactivity buttoalsocause
signif-icantmucosaldamagetoratrectalmucosacomparedwith
theshamandcontrolgroups.
Alpha2agonists constitutea groupof drugscommonly
used in anesthesia for the purposes of sedation,
analge-sia and anesthesia.11---14,18---24 Clonidine, a member of this
group, can also be used for premedication.11---14 Rectal
Table2 Histopathologicalevaluationscoresaccordingtogroup(median[25th---75thpercentiles]).
GroupS(n=8) GroupC(n=8) GroupRecDex(n=8) p
Microscopicscore 0(0-0) 0(0-0) 2(2-2)a,b 0.001
premedication administration is particularly preferredfor youngchildrenduetotheeaseofadministration.2,3,9---11
Previous studies have reported that clonidine can be
usedeffectively rectally.11---14 Comparing the effectiveness
of rectally administered clonidine to that of midazolam,
Bergendahletal.11foundthattheuseoftheformeras
pre-medication resulted in lowerpain scores than midazolam
intheearlypostoperativestage.Theauthorsalsoreported
thatchildrenwhowererectallyadministeredketaminewere
more sedated in first 24 postoperative hours than those
whoreceivedmidazolam.11 In a study comparingthe
rec-tal administrationof 2.5gkg−1 clonidine and300gkg−1
midazolamtopreventtheincreaseinneuropeptideYcaused
bytracheal intubationinchildren, Bergendaletal.13
con-cluded that there was no significant difference between
the two groups. A study that investigated the
pharma-cokineticcharacteristicsofrectallyadministeredclonidine
demonstratedthatitsmaximum plasmaconcentrationwas
0.77ngmL−1 and that the time required to reach this
concentrationwas51min.14 Thesamestudyfoundthatthe
half-lifeofrectalclonidinewas12.5handthebioavailability
was95%.Theauthorsreportedthattheplasma
concentra-tionof clonidinereached clinicallyeffective levels10min afterrectal administration.14 Theystated that2.5
gkg−1
clonidine rectally administered to children approximately
20minbeforeanesthesiainductioncouldachieveaclinically effectiveplasmaconcentration.14
Dexmedetomidine is a highly specific and sensitive
alpha adrenergic agonist, and it can be administered
orally, nasally, transmucosally or intramuscularly for
premedication.4,8,18---24
Özcengiz et al.20 showed that oral dexmedetomidine
could preventpost-sevolurane agitation in children. Yuen
etal.4reportedthat1
gkg−1intranasaldexmedetomidine
producedsignificantlyhighersedationinchildrenaged2---12
yearscomparedwithoral midazolam.Theauthors
empha-sizedthatdexmedetomidineandmidazolamcreatedsimilar
premedicationconditionsandthatbothwereacceptable.4
In anotherstudy, Yuenetal.29 found that sedation began
anaverageof25minafterintranasaldexmedetomidineand
that the mean duration of sedation was 85min. Sakurai
etal.21reportedthat3---4
gkg−1dexmedetomidine
admin-isteredtochildrenbuccally1hbeforesurgerywasreliable
andeffective.
In a comparison of the effects of 2gkg−1 intranasal
dexmedetomidine and 0.5mgkg−1 midazolam for
preme-dication in pediatric patients, Talon et al.22 found that
thetwodrugshadsimilaranesthesiainduction and
recov-ery characteristics. However, the authors reported that
dexmedetomidinewasmoreeffectiveininducingsleepand
thatitwasausefulalternativetooralmidazolam.22
Althoughtherectaluseofclonidineandtheoral,nasal
and transmucosal use of dexmedetomidine for
premedi-cationhavebeendefined,thereisnoliteratureontherectal
useofdexmedetomidine.
In our study, the rectal administration of 100gkg−1
dexmedetomidine achieved anesthesia in all the rats in
thatgroup. Thedurationof anesthesiainboth thegroups
thatreceivedintraperitonealandrectaldexmedetomidine
was significantly longer than in the sham and control
groups.However,theonsetofanesthesiawassignificantly
later in the rectal dexmedetomidine group than in the
intraperitonealdexmedetomidine group,and theduration
ofanesthesiawassignificantlyshorterthaninthe intraperi-tonealgroup.
Rectal administrationis an alternative method of
pre-medication,particularlyforyoungchildren.Theabsorption
mechanisms of rectally administered drugs resemble the
uppergastrointestinalsystem.Passivetransportisthemain
mechanismofrectaldrugabsorption.Theabsorptionspeed
ofrectallyadministereddrugsisinfluencedbyfactorssuch
as the molecular weight, lipid solubility and ionization
degreeof thedrug.However,therectaladministrationof
drugshasbeenreportedtocausesideeffectssuchaslocal
inflammation, rectal mucosal damage, rectal ulceration,
rectalbleedingandpain.30
Therectaladministrationofanestheticagentsmayalso
causerectalmucosaldamage.25Previousstudieshaveshown
thatrectallyadministered10%methohexitonecausesrectal
mucosaldamageinratsthatbeginswithinminutes,becomes
noticeableat60min,andcontinues24h.25
However,therehavebeenonlyafewstudiesofthe
rec-talmucosaleffectsofalpha2agonists.31,32Maxsonetal.31
reportedclonidineadministrationtoratstodecreasemucus
productioninanintestinalischemia/reperfusionmodel.In
acase study,thelong-termuse ofclonidine wasreported
tocause cicatricialpemphigoidin theanus,vulvamucosa
andperianalskin.32Inthatcase,thedirect immunofloures-centexaminationofthelesionsindicatedthepossibilityof
complement-mediated tissue damage between epidermal
basalcellsandthebasalmembrane.32
Inourliteraturereview,wewerenotabletofindastudy
thatevaluated the effectsof rectally administered
cloni-dine on rectal mucosa cells. We found in our study that
rectallyadministered100gkg−1dexmedetomidinecaused
themoderatelossoftherectalmucosalsurfaceand
glandu-larepithelialcells.Weareoftheopinionthatthemucosal
damage caused by dexmedetomidine may have a
mecha-nismsimilartothatofclonidine.31,32 However,wedidnot
investigatethemechanisms ofmucosal damageformation
inthepresentstudy.Thesepreliminaryfindingsinratsmay
not be observed in rectal mucosa of humans due to the
highdose andresultinghigh concentration appliedtothe
rectalmucosainthisstudy.Webelievethatfuturestudies
shouldinvestigatetheeffectsofdexmedetomidineonrectal
mucosaandthereversibilityofthedamage.
Thedexmedetomidinedosageusedinourstudywas
iden-tifiedasthemosteffectiveinrectaluseinthepreliminary
study.Severalother studies have demonstrated
neuropro-tectiveeffects of dexmedetomidine,albeit onlyat higher
doses(upto100gkg−1).33---35
In conclusion, although the rectal administration
of dexmedetomidine to rats achieved a significantly
longer duration of anesthesia compared with saline, our
histopathologicalevaluationshowedthattheformer
treat-ment led to moderate damage in the mucosal structure
of the rectum. Therefore, for the rectally safe use of
dexmedetomidineaspremedication,webelievethatfuture
studiesareneededtorevealtheeffectsofthedrugonrectal mucosa.
Conflicts
of
interest
References
1.YousafF,SeetE,VenkatraghavanL,etal.Efficacyandsafety ofmelatoninasananxiolyticandanalgesicintheperioperative period:aqualitativesystematic reviewofrandomizedtrials. Anesthesiology.2010;113:968---76.
2.ZanetteG,MicaglioM,ZanetteL,etal.Comparisonbetween ketamineandfentanyl---droperidolforrectalpremedicationin children: a randomized placebo controlled trial. J Anesth. 2010;2:197---203.
3.Bozkurt P. Premedication of the pediatric patient --- anes-thesia for the uncooperative child. Curr Opin Anaesthesiol. 2007;20:211---5.
4.YuenVM,HuiTW,IrwinMG,etal.Acomparisonofintranasal dexmedetomidine and oral midazolam for premedication in pediatricanesthesia:adouble-blindedrandomizedcontrolled trial.AnesthAnalg.2008;106:1715---21.
5.HoseyMT,AsburyAJ,BowmanAW,etal.Theeffectof transmu-cosal0.2mg/kg midazolampremedicationondental anxiety, anaestheticinductionandpsychologicalmorbidityinchildren undergoinggeneralanaesthesiafortoothextraction.BrDentJ. 2009;207:E2(discussion32---33).
6.Cruz JR, Cruz DF, Branco BC, et al. Clonidine as pre-anesthetic medication in cataract extraction: comparison between 100microg and 200microg. Rev Bras Anestesiol. 2009;59:694---703.
7.AlmenraderN,PassarielloM,CoccettiB,etal.Premedication inchildren:acomparisonoforalmidazolamandoralclonidine. PaediatrAnaesth.2007;17:1143---9.
8.YuenVM.Dexmedetomidine:perioperativeapplicationsin chil-dren.PaediatrAnaesth.2010;20:256---64.
9.WangX,ZhouZJ,ZhangXF,etal.Acomparisonoftwodifferent dosesofrectalketamineaddedto0.5mg×kg(−1)midazolam and 0.02mg×kg(−1)atropineininfantsand youngchildren. AnaesthIntensiveCare.2010;38:900---4.
10.SayinMM,Mercan A,TureH,et al.Theeffectof2different concentrationsofrectalketamineonitspremedicantfeatures inchildren.JSaudiMed.2008;29:683---7.
11.Bergendahl HT,Lönnqvist PA,Eksborg S, et al.Clonidine vs. midazolamaspremedicationinchildrenundergoing adenoton-sillectomy:aprospective,randomized,controlledclinicaltrial. ActaAnaesthesiolScand.2004;48:1292---300.
12.ConstantI,LeportY,RichardP,etal.Agitationandchangesof BispectralIndexandelectroencephalographic-derivedvariables during sevoflurane induction in children: clonidine preme-dication reduces agitation compared with midazolam. Br J Anaesth.2004;92:504---11.
13.Bergendahl HT, Eksborg S, Kogner P, et al. Neuropeptide Y response to tracheal intubation in anaesthetized children: effects of clonidine vs midazolam as premedication. Br J Anaesth.1999;82:391---4.
14.LönnqvistPA,Bergendahl HT,EksborgS. Pharmacokineticsof clonidineafterrectaladministrationinchildren. Anesthesiol-ogy.1994;81:1097---101.
15.Hanci V, Erdo˘gan G, Okyay RD, et al. Effects of fentanyl-lidocaine-propofolanddexmedetomidine-lidocaine-propofolon trachealintubationwithoutuseofmusclerelaxants.Kaohsiung JMedSci.2010;26:244---50.
16.Hanci V, Erol B, Bektas¸ S, et al. Effect of dexmedetomi-dineontesticulartorsion/detorsiondamageinrats.UrolInt. 2010;84:105---11.
17.HanciV,KarakayaK,YurtluS,etal.Effectsofdexmedetomidine pretreatmentonbupivacainecardiotoxicityinrats.RegAnesth PainMed.2009;34:565---8.
18.GhaliAM,MahfouzAK,Al-BahraniM.Preanestheticmedication inchildren:acomparisonofintranasaldexmedetomidineversus oralmidazolam.SaudiJAnaesth.2011;5:387---91.
19.MizrakA,GulR,GanidagliS,etal.Dexmedetomidine preme-dicationofoutpatientsunderIVRA.MiddleEastJAnesthesiol. 2011;21:53---60.
20.ÖzcengizD,GunesY,OzmeteO.Oralmelatonin, dexmedetomi-dine,andmidazolamforpreventionofpostoperativeagitation inchildren.JAnesth.2011;25:184---8.
21.SakuraiY, ObataT, OdakaA, et al.Buccal administrationof dexmedetomidine as a preanesthetic in children. J Anesth. 2010;24:49---53.
22.Talon MD, Woodson LC, Sherwood ER, et al. Intranasal dexmedetomidinepremedicationiscomparablewith midazo-laminburnchildrenundergoingreconstructivesurgery.JBurn CareRes.2009;30:599---605.
23.ZubD,BerkenboschJW,TobiasJD.Preliminaryexperiencewith oraldexmedetomidineforproceduralandanesthetic premedi-cation.PaediatrAnaesth.2005;15:932---8.
24.ErkolaO,KorttilaK,AhoM,etal.Comparisonofintramuscular dexmedetomidineand midazolam premedicationfor elective abdominalhysterectomy.AnesthAnalg.1994;79:646---53. 25.HinkleAJ,WeinlanderCM.Theeffectsof10%methohexitalon
therectalmucosainmice.Anesthesiology.1989;71:550---3. 26.Ozbakis-Dengiz G, Bakirci A. Anticonvulsant and hypnotic
effects of amiodarone. J Zhejiang Univ Sci B. 2009;10: 317---22.
27.LeungFW,SuKC,PiqueJM,etal.Superiormesentericartery ismoreimportantthaninferiormesentericarteryin maintain-ingcolonicmucosalperfusionandintegrityinrats.DigDisSci. 1992;37:1329---35.
28.GuneliE,KarabayYavasogluNU,ApaydinS,etal.Analysisofthe antinociceptiveeffectofsystemicadministrationoftramadol and dexmedetomidine combination on rat models of acute and neuropathic pain. Pharmacol Biochem Behav. 2007;88: 9---17.
29.YuenVM,HuiTW,IrwinMG,etal.Optimaltimingforthe admin-istrationofintranasaldexmedetomidineforpremedicationin children.Anaesthesia.2010;65:922---9.
30.Bergogne-BérézinE,BryskierA.Thesuppositoryformof antibi-oticadministration:pharmacokineticsandclinicalapplication. JAntimicrobChemother.1999;43:177---85.
31.MaxsonRT,DunlapJP, Tryka F,et al.The role ofthemucus gel layer in intestinal bacterial translocation. J Surg Res. 1994;57:682---6.
32.vanJoost T, Faber WR,ManuelHR. Drug-induced anogenital cicatricialpemphigoid.BrJDermatol.1980;102:715---8. 33.Engelhard K, Werner C,EberspächerE, et al. The effectof
the␣2-agonistdexmedetomidineandtheN-methyl-daspartate antagonist S+ ketamine on the expression of apoptosis-regulating proteins after incomplete cerebral ischemia and reperfusioninrats.AnesthAnalg.2003;96:524---31.
34.JolkkonenJ,PuurunenK,KoistinahoJ,etal.Neuroprotection bythe␣-adrenoceptoragonist,dexmedetomidine,inratfocal cerebralischemia.EurJPharmacol.1999;372:31---6.