ABSTRACT:Objective: To describe the incidence and mortality rates from colon and rectal cancer in Midwestern Brazil. Methods: Data for the incidence rates were obtained from the Population-Based Cancer Registry (PBCR) according to the available period. Mortality data were obtained from the Mortality Information System (SIM) for the period between 1996 and 2008. Incidence and mortality rates were calculated by gender and age groups. Mortality trends were analyzed by the Joinpointsoftware. The age-period-cohort efects were calculated by the R software. Results: The incidence rates for colon cancer vary from 4.49 to 23.19/100,000, while mortality rates vary from 2.85 to 14.54/100,000. For rectal cancer, the incidence rates range from 1.25 to 11.18/100,000 and mortality rates range between 0.30 and 7.90/100,000. Colon cancer mortality trends showed an increase among males in Cuiabá, Campo Grande, and Goiania. For those aged under 50 years, the increased rate was 13.2% in Campo Grande. For those aged over 50 years, there was a signiicant increase in the mortality in all capitals. In Goiânia, rectal cancer mortality in males increased 7.3%. For females below 50 years of age in the city of Brasilia, there was an increase of 8.7%, while females over 50 years of age in Cuiaba showed an increase of 10%. Conclusion: There is limited data available on the incidence of colon and rectal cancer for the Midwest region of Brazil. Colon cancer mortality has generally increased for both genders, but similar data were not veriied for rectal cancer. The indings presented herein demonstrate the necessity for organized screening programs for colon and rectal cancer in Midwestern Brazil.
Keywords: Rectal neoplasms. Colonic neoplasms. Incidence. Mortality. Trends. Brazil.
Incidence and mortality from colon
and rectal cancer in Midwestern Brazil
Incidência e mortalidade por câncer de cólon e reto no Centro-Oeste do Brasil
Anderson Gomes de OliveiraI, Maria Paula CuradoI,II,III, Alice KoechlinIII, José Carlos de OliveiraIV, Diego Rodrigues Mendonça e SilvaI,II
ORIGINAL ARTICLE / artigo original
IPostgraduate Program in Health Sciences, Universidade Federal de goiás – Goiânia (GO), Brazil.
IIEpidemiology Department, International Center for Research, A.C. Camargo Cancer Center – São Paulo (SP), Brazil.
IIIInternational Prevention Research Institute – Écully, France.
IVPopulation-Based Cancer Registry of Goiânia, Association Against Cancer of Goiás – Goiânia (GO), Brazil.
Corresponding author: Maria Paula Curado. A.C. Camargo Cancer Center. Rua Tagua, 440, Liberdade, CEP: 01508-020, São Paulo, SP, Brasil. E-mail: [email protected]
Conlict of interests: nothing to declare. Financial support: Fundação de amparo à Pesquisa do Estado de goiás, training Grant,
IntroductIon
Colon and rectal cancer is the third most common cancer in both genders worldwide, especially in more developed countries, with estimated incidences varying between 36.3 and 37.9 per 100,000 inhabitants1,2. The lowest incidence rates were to be found in South Africa (1.70/100,000) and in India (2.0/100,000). In South American countries, rates vary between 5.0/100,000 (Cuenca – Ecuador) and 35.5/100,000 (São Paulo – Brazil) with the latter being comparable to rates in developed countries3. In European countries, there has been a signif-icant increase in the incidence of colon and rectal cancer in males4,5. However, these trends contrast with the standards encountered in the USA, where incidence trends have decreased in the last two decades. This decrease is attributed to organized screening programs6.
In Brazil, colon and rectal cancers are among the ive most diagnosed cancers, and are the third highest cause of cancer-related deaths7. Data from the Population-Based Cancer Registry (PBCR) for the period 2002 – 2010 indicate that the highest incidence rates for males and females occurred in Porto Alegre, São Paulo and Goiânia while the lowest rates were observed in Recife and João Pessoa8. According to the aforementioned data, colon and rectal cancer incidence rates have presented similar patterns in southern and southeastern Brazil, although there are no existing studies to assess these results or verify this proile in the Midwest.
Mortality rates are still showing an increasing trend in countries with more limited resources, including Brazil and Chile in South America9,10. Colon and rectal cancer mor-tality trends in Brazilian state capitals, in both males and females, increased between 1980 and 200611. This was followed by a period of stability up to 2010, according to the data.
RESUMO:Objetivo: Descrever o peril do câncer de cólon e reto no Centro-Oeste do Brasil. Métodos: Os dados de incidência foram obtidos dos Registros de Câncer de Base Populacional (RCBP) de acordo com o período disponível. Dados sobre os óbitos foram obtidos do Sistema de Informação em Mortalidade (SIM). As taxas de incidência e mortalidade foram calculadas por gênero e grupos etários. As tendências de mortalidade foram analisadas pelo software Joinpoint. Os efeitos de idade-período-coorte foram calculados no software R. Resultados:As taxas de incidência do câncer de cólon variaram de 4,49 a 23,19/100.000, e a mortalidade, de 2,85 a 14,54/100.000. A incidência do câncer de reto variou de 1,25 a 11,18/100.000; a mortalidade, de 0,30 a 7,90/100.000. As tendências de mortalidade por câncer de cólon mostraram um aumento entre homens em Cuiabá, Campo Grande e Goiânia. Para aqueles abaixo dos 50 anos, o aumento foi de 13,2% em Campo Grande. Para aqueles acima dos 50 anos, houve um aumento signiicante em todas as capitais. Em Goiânia, a mortalidade por câncer de reto em homens aumentou 7,3%. Para mulheres abaixo dos 50 anos em Brasília, o aumento foi de 8,7%, enquanto que para mulheres acima dos 50 anos em Cuiabá foi de 10%. Conclusão: Os dados de incidência do câncer de cólon e reto no Centro-Oeste do Brasil são limitados. A mortalidade por câncer de cólon tem aumentado para ambos os sexos, mas o mesmo não foi veriicado para câncer de reto. Os resultados demonstram a necessidade de programas organizados de rastreamento para esta neoplasia no Centro-Oeste.
The number of deaths in Brazil decreased in the whole country with the exception of males in the Brazilian northern region12.
This study aimed to describe the incidence and mortality rates from colon and rectal cancer in Midwestern Brazil.
MEtHodS
This is an observational, descriptive, population-based study. The incidence of cases of colon and rectal cancer was obtained from SisBasepop Web at the National Institute for Cancer (INCA/MS), in Brazil13. The available time periods for analysis were Brasília (DF) 1999 – 2002, Campo Grande (MS) 2000 – 2001, and Cuiabá (MT) 2000 – 2004. Data for Goiânia (GO) were obtained from the PBCR in Goiânia for the period 1988 – 2008. The variables were age, gender, and age groups (< 50 and ≥ 50).
Inclusion criteria for incident and mortality cases of colon and rectal cancer were based on codes C-18, C-19, and C-20 of the the International Statistical Classiication of Diseases and Related Health Problems, 10th Revision, (ICD-10)14.
Population estimates were taken from the data at the Brazilian Institute of Geography and Statistics (IBGE)15. The standard population, according to Segi16, was used to calculate standardized incidence and mortality rates.
Data on deaths due to colon and rectal cancer were obtained from the Mortality Information System (SIM/DATASUS) of the Brazilian Ministry of Health (MS)17. Mortality rates were calculated in the cities of Goiânia, Brasília, Cuiabá, and Campo Grande for the period 1996 – 2008.
rESuLtS
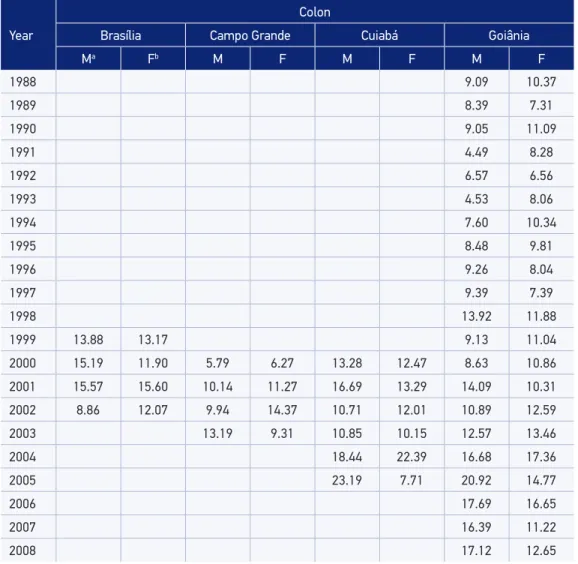
There is a lack of continuous data on the incidence of colon and rectal cancer for the period 1988 – 2008 in Midwestern Brazil. According to the PBCR of this region, the rates for colon cancer incidence vary from 4.49 to 23.19/100,000. The highest inci-dence rates for colon cancer were observed in Cuiabá, with 23.19 and 22.39/100,000 in males and females, respectively. The incidence of rectal cancer ranged from 1.25 to 11.18/100,000, which is two times lower in comparison with colon cancer. The high-est rectal cancer incidence rates were observed for males and females in Cuiabá and Goiânia, respectively (Table 1).
Table 1. Age-standardized incidence rates for colon and rectal cancer in males and females in Midwestern Brazil for the period 1988 – 2008.
Year
Colon
Brasília Campo Grande Cuiabá Goiânia
Ma Fb M F M F M F
1988 9.09 10.37
1989 8.39 7.31
1990 9.05 11.09
1991 4.49 8.28
1992 6.57 6.56
1993 4.53 8.06
1994 7.60 10.34
1995 8.48 9.81
1996 9.26 8.04
1997 9.39 7.39
1998 13.92 11.88
1999 13.88 13.17 9.13 11.04
2000 15.19 11.90 5.79 6.27 13.28 12.47 8.63 10.86
2001 15.57 15.60 10.14 11.27 16.69 13.29 14.09 10.31
2002 8.86 12.07 9.94 14.37 10.71 12.01 10.89 12.59
2003 13.19 9.31 10.85 10.15 12.57 13.46
2004 18.44 22.39 16.68 17.36
2005 23.19 7.71 20.92 14.77
2006 17.69 16.65
2007 16.39 11.22
2008 17.12 12.65
Year
Rectal
Brasília Campo Grande Cuiabá Goiânia
Ma Fb M F M F M F
1988 3.25 3.54
1989 3.45 2.01
1990 2.03 3.50
1991 2.52 1.88
1992 1.94 2.59
1993 3.20 4.36
1994 4.54 3.67
1995 5.61 3.77
1996 1.25 4.03
1997 2.50 3.99
1998 4.50 5.54
1999 5.54 4.87 5.10 6.10
2000 7.24 3.31 4.68 2.56 7.86 11.18 4.49 5.05
2001 5.26 5.22 5.68 2.32 7.86 8.63 6.60 3.98
2002 4.90 4.68 3.98 3.07 7.77 6.22 5.60 5.50
2003 1.73 2.47 6.70 5.29 5.18 6.01
2004 8.00 4.60 9.48 6.93
2005 7.52 6.88 8.81 8.69
2006 8.55 6.28
2007 6.27 6.35
2008 5.16 3.43
aMales; bFemales. Source: Sisbasepop13.
Table 1. Continue.
The highest mortality rates for males with colon cancer were observed in Campo Grande (14.54/100,000), and for females, it reached 10.26/100,000 in Goiânia. Rectal mortality, how-ever, was higher in Cuiabá for males (7.92/100,000) (Table 2).
Table 2. Age-standardized mortality rates for colon and rectal cancer in males and females in Midwestern Brazil for the period 1996–2008.
Year
Colon
Brasília Campo Grande Cuiabá Goiânia
Ma Fb M F M F M F
1996 5.14 4.65 7.46 3.72 2.85 4.96 5.66 5.18
1997 5.64 3.83 8.27 6.97 6.50 4.20 5.89 4.87
1998 3.59 7.63 4.31 5.72 5.07 3.84 6.49 4.87
1999 7.80 6.14 8.18 7.59 4.77 8.27 9.79 4.30
2000 7.26 4.84 3.94 6.61 4.66 5.29 6.79 6.18
2001 8.10 6.05 7.12 7.05 5.81 8.82 7.57 5.88
2002 7.25 7.64 7.25 8.26 9.94 5.42 6.91 6.61
2003 4.55 5.48 9.26 5.90 5.79 4.76 8.28 7.43
2004 7.99 8.30 10.20 8.48 8.04 5.01 9.68 8.35
2005 9.99 7.20 12.12 8.57 10.92 7.53 10.04 8.14
2006 9.42 9.72 11.65 9.40 9.95 6.97 11.44 10.26
2007 6.76 6.60 8.08 8.82 6.25 5.39 12.04 8.27
2008 6.67 6.47 14.54 6.41 11.05 7.97 9.18 7.65
Year
Rectal
Brasília Campo Grande Cuiabá Goiânia
Ma Fb M F M F M F
1996 3.80 1.43 2.62 4.36 4.26 1.34 1.97 3.02
1997 4.82 2.43 0.30 1.47 2.45 0.99 4.05 3.57
1998 3.59 2.19 5.11 2.44 7.92 4.10 3.75 3.17
1999 2.27 1.31 3.90 3.98 1.35 1.72 3.26 3.58
2000 3.20 1.57 1.91 2.05 0.34 2.42 3.19 3.33
2001 3.42 2.61 0.66 2.56 2.50 1.70 5.16 3.07
2002 2.30 3.10 4.45 3.07 1.17 2.32 4.87 3.13
2003 3.41 3.43 3.47 2.56 3.20 0.74 6.10 2.24
2004 4.15 3.06 2.07 2.99 5.53 3.75 6.87 5.02
2005 2.82 3.49 2.13 2.71 2.33 5.72 6.46 4.74
2006 2.57 3.51 4.14 2.29 3.03 2.82 5.81 4.60
2007 2.76 2.70 1.48 2.41 1.95 1.89 5.23 4.02
2008 3.36 3.42 1.85 2.11 7.90 4.88 5.40 2.86
Table 3. Mortality trends for colon and rectal cancer, in males and females, in Midwestern Brazil, for the period 1996 – 2008.
Colon
Year
APCa (95%CIb) p-value APCa (95%CIb) p-value
Males Females
Brasília 1996-2008 3,7 (-0.6, 8.3) 0.0882 4,0 (0.4, 7.7) 0.0320
Campo Grande 1996-2008 6,4 (1.3, 11.6) 0.0173 4,0 (0.6, 7.5) 0.0249
Cuiabá 1996-2008 8,1 (3.4, 13.1) 0.0027 3,1 (-1.2, 7.4) 0.1405
Goiânia 1996-2008 5,4 (2.9, 8.0) 0.0004 6,1 (3.8, 8.4) 0.0000
Rectal
Year
APCa (95%CIb) p-value APCa (95%CIb) p-value
Males Females
Brasília 1996-2008 -2.0 (-5.4, 1.6) 0.2366 6,9 (2.7, 11.3) 0.0036
Campo Grande 1996-2008 2,8 (-10.2, 17.8) 0.6615 -1.4 (-5.9, 3.4) 0.5278
Cuiabá 1996-2008 3,5 (-10.3, 19.4) 0.6113 7,5 (-2.0, 17.9) 0.1148
Goiânia 1996-2008 7,3 (3.3, 11.4) 0.0017 1,7 (-2.0, 5.6) 0.3327
aAnnual Percentage Change; bConidence interval. Source: Mortality Information System/DATASUS17.
increased for males in Goiânia to 7.3% (3.8; 11.0) and for females in Brasília to 6.9% (p < 0.05) (Table 3).
The highest trends for mortality from colon cancer in males aged under 50 years occurred in Campo Grande, at 13.2% (3.4; 24.0), and reached 11.5% (3.7; 19.9) in Cuiabá; however, mortality increased in all cities for those aged over 50 years, from 4.9% (0.5; 9.6) to 8.2% (2.4; 14.3). Rectal cancer mortality trends increased by 7.4% (3.1; 11.8) in males over 50 years of age in Goiânia, while in females under 50 years of age, the increase reached 8.7% (1.3; 6.7) in Brasília (Table 4).
Table 4. Mortality trends for colon and rectal cancer, according to age groups for males and females in Midwestern Brazil, for the period 1996 – 2008.
Period
Colon
< 50 years ≥ 50 years
APCa (CIb) p-value APCa (CIb) p-value APCa (CIb) p-value APCa (CIb) p-value
Males Females Males Females
Brasília
1996–2008 (-4.9; 14.6)4.4 0.332 (1.5; 10.0)5.7 0.014 (0.5; 9.6)4.9 0.033 (0.5; 8.1)4.2 0.032
Campo Grande
1996–2008 (3.4; 24.0)13.2 0.012 (-0.7; 29.0)13.2 0.061 (1.1; 10.8)5.8 0.012 (-0.3; 8.7)2.9 0.082
Cuiabá
1996–2008 (3.7; 19.9)11.5 0.007 (-5.1; 18.4)6.0 0.269 (2.4; 14.3)8.2 0.009 (-2.8; 7.5)2.2 0.354
Goiânia
1996–2008 (-2.0; 10.7)4.2 0.169 (-2.4; 11.4)4.3 0.193 (3.6; 8.9)6.2 <0.001
6.6
(3.4; 10.0) 0.001
Period
Rectal
< 50 years ≥ 50 years
APCa (CIb) p-value APCa (CIb) p-value APCa (CIb) p-value APCa (CIb) p-value
Males Females Males Females
Brasília 1996–2008
6.4
(-0.4; 3.7) 0.062 (1.3; 6.7)8.7 0.024 (-6.3; 1.5)-2.5 0.193 (2.6; 13.3)7.8 0.007
Campo Grande
1996–2008 (-13.2; 7.6)-3.4 0.484 (-12.1; 5.2)-3.8 0.356
4
(-6.9; 16.0) 0.454 (-5.8; 5.8)-0.2 0.95
Cuiabá 1996–2008
2.0
(-12.4; 18.8) 0.764
-3.5
(-14.9; 9.3) 0.519
1.1
(-10.8; 14.6) 0.846
10.0
(1.1; 19.6) 0.03
Goiânia
1996–2008 (-1.9; 14.8)5.6 0.176 (-5.1; 22.4)7.8 0.217 (3.1; 11.8)7.4 0.003 (-3.7; 4.8)0.4 0.822
aAnnual Percentage Change; bConidence Interval = 95%. Source: Mortality Information System /DATASUS17.
dIScuSSIon
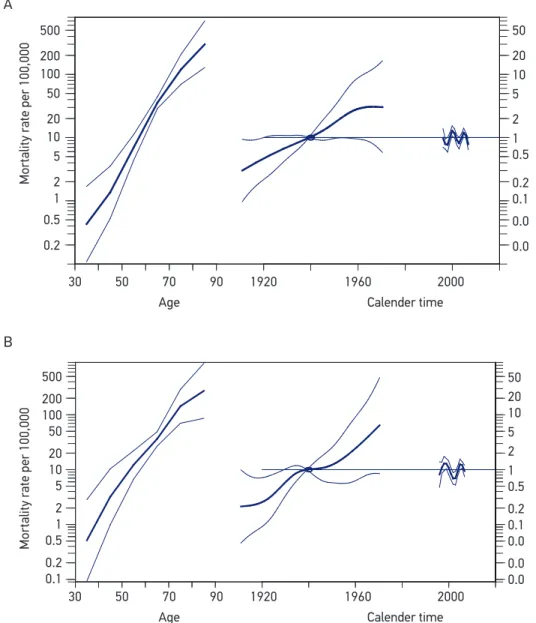
Figure 1. Age-period-cohort efect on colon cancer mortality rates between 1996 and 2008, in Brasília, for the male population (A), and in Campo Grande, for the female population (B).
500
200 100 50
20 10 5
2 1 0.5
0.2
30 50 70 90 1920 1960 2000
50
20 10 5
2 1 0.5
0.2 0.1
0.0
0.0
50 20 10 5 2 1 0.5
0.2 0.1 0.0
0.0 0.0
Mortality rate per 100,000
Mortality rate per 100,000
Age
A
B
Calender time
30 50 70 90 1920 1960 2000
Age Calender time
500
200 100 50
20 10 5
2 1 0.5
0.2 0.1
diet of the population tends to include the consumption of red meat and is accompanied by a low intake of vegetables, a dietary proile similar to that of the southern region23.
One characteristic of migrant groups is that they tend to maintain the typical eating habits and customs of their region of origin, and these eating habits persist for long peri-ods28. Thus, the immigrant population from Southern Brazil most likely retained typical habits, such as the consumption of herb tea, alcoholic beverages, smoking tobacco, and other dietary habits, such eating barbecue weekly21,29. Preserving these habits could have contributed to the higher incidence of colon and rectal cancer identiied in this study, par-ticularly in Cuiabá and Goiânia.
The mortality rates in Midwestern Brazil for colon and rectal cancer presented herein have increased throughout the years, although they were unstable. Despite the fact that colon and rectal mortality rates decreased in developed countries, such as the UK, France, and the USA2,30, increases have been documented in Asia, particularly in Japan, China, and Korea1,31 and also among US immigrants in general29. As such, our results remain similar to those found in Asia, Eastern Europe, Colombia, and Costa Rica32,33. Trends for colon cancer mortality showed an increase in the last decade, among both genders, although the rate of increase is more pronounced among the male population10.
In Midwestern Brazil, signiicant increases in colon cancer mortality were found among males under 50 years of age, speciically in Campo Grande and Cuiabá, while rectal cancer increased within the same age group for females in Brasília. However, for adults under the age of 50, increases were recorded in all the cities studied. Recent studies have found that the mortality rates from colon and rectal cancer have been decreasing in adults over 50 years of age. However, these rates have been increasing in adults under 5034.
In the age-period-cohort analysis, there was a signiicant efect of group on mortality, among the male population of Brasília (p = 0.01) and the female population of Campo Grande (p < 0.05). This result demonstrates that the increase in mortality rates is still connected to the lifestyle of the population, as it corresponds to a birth cohort efect35. Therefore, if adopted, organized screening programs can change this proile in Midwestern Brazil36,37.
The results obtained herein present two main limitations. The irst is the low level of historical incidence data available from the registries in the Midwest region. Data disconti-nuity in cancer registries hinders a more accurate analysis of rates. Another limitation is the quality of the data in the registries, with Campo Grande for example registering approxi-mately 20% of its cases only on the basis of death certiicates, which demonstrates a lack of completeness in abstracting the incident cases there.
concLuSIon
1. Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide. IARC CancerBase No. 11. Lyon: International Agency for Research on Cancer; 2013. Disponível em: http://globocan.iarc. fr (Acessado em 18 de janeiro de 2016).
2. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65(2): 87-108.
3. Forman D, Bray F, Brewster DH, Gombe Mbalawa C, Kohler B, Piñeros M, et al. Cancer Incidence in Five Continents Vol. X. IARC Scientiic Publication No. 164. Lyon: International Agency for Research on Cancer; 2014.
4. Ferlay J, Bray F, Steliarova-Foucher E and Forman D. (2014) Cancer Incidence in Five Continents: CI5plus. IARC Cancer Base No. 9 Lyon: International Agency for Research on Cancer; 2014. Disponível em: http://ci5.iarc.fr (Acessado em 6 de fevereiro de 2016).
5. Center MM, Jemal A, Ward E. International trends in colorectal cancer incidence rates. Cancer Epidemiol Biomarkers Prev 2009; 18(6):1688-94.
6. Cress RD, Morris C, Ellison GL, Goodman MT. Secular changes in colorectal cancer incidence by subsite, stage at diagnosis, and race/ethnicity, 1992-2001. Cancer 2006; 107(5 Suppl): 1142-52.
7. Schmidt MI; Duncan BB; Silva GA; Menezes AM; Monteiro CA; Barreto SM, et al. Doenças crônicas não transmissíveis no Brasil: carga e desaios atuais. Séries. Lancet 2011; 377(9781): 61-74.
8. Instituto Nacional de Câncer (INCA). Coordenação de Prevenção e Vigilância. Registros de Câncer de Base Populacional. Rio de Janeiro: INCA; 2010. Disponível em http://www2.inca.gov.br/wps/wcm/connect/ estatisticas/site/home/rcbp/ (Acessado em 6 de fevereiro de 2016).
9. Bosetti C, Bertuccio P, Malvezzi M, Levi F, Chatenoud L, Negri E, et al. Cancer mortality in Europe, 2005-2009, and an overview of trends since 1980. Ann Oncol 2013; 24(10): 2657-71.
10. Chatenoud L, Bertuccio P, Bosetti C, Malvezzi M, Levi F, Negri E, et al. Trends in mortality from major cancers in the Americas: 1980-2010. Ann Oncol 2014; 25(9): 1843-53.
11. Silva GA, Gamarra CJ, Girianelli VR, Valente JG. Cancer mortality trends in Brazilian state capitals and other municipalities between 1980 and 2006. Rev Saúde Pública 2011; 45(6): 1009-18.
12. Souza DL, Jerez-Roig J, Cabral FJ, de Lima JR, Rutalira MK, Costa JA. Colorectal cancer mortality in Brazil: predictions until the year 2025 and cancer control implications. Dis Colon Rectum 2014; 57(9): 1082-9. 13. Instituto Nacional de Câncer (INCA). Coordenação
de Prevenção e Vigilância. Programa Sisbasepop. Rio de Janeiro: INCA; 2010. Disponível em http://www2. inca.gov.br/wps/wcm/connect/estatisticas/site/ home/rcbp (Acessado em 10 de setembro de 2011). 14. World Health Organization (WHO). International
Statistical Classiication of Diseases and Related Health Problems, 10th Revision (ICD-10). WHO: 2011.
15. Brasil. Ministério da Saúde. Instituto Brasileiro de Geograia e Estatística (IBGE). Informações populacionais. 2009. Disponível em http://www2.datasus.gov.br/ DATASUS/index.php?area=0206&VObj=http:// tabnet.datasus.gov.br/cgi/deftohtm.exe?ibge/cnv/ pop (Acessado em 15 de setembro de 2011). 16. Segi M. Cancer mortality for selected sites in 24
countries (1950-57). Sendai: Department of Public Health, Tohoku University School of Medicine; 1960. 17. Brasil. Ministério da Saúde. Departamento de Informática do SUS (DATASUS). Informações de saúde/mortalidade. 2009. Disponível em http://www2.datasus.gov.br/DATASUS/ index.php?area=0205&id=6937&VObj=http://tabnet. datasus.gov.br/cgi/deftohtm.exe?sim/cnv/obt10 (Acessado em 15 de setembro de 2011).
18. National Cancer Institute. Division of Cancer Control & Population Sciences. Joinpoint Regression Program [computer program]. Version 3.5.1; Statistical Research and Applications Branch, National Cancer Institute. Disponível em http:// surveillance.cancer.gov/joinpoint/ (Acessado em 20 de setembro de 2011).
19. Carstensen B. Age-period-cohort models for the Lexis diagram. Stat. Med 2007; 26(15): 3018-45.
20. The R Core Team . R: A language and environment for statistical computing [computer program]. Vienna: R Foundation for Statistical Computing; 2010. 21. Marcolin, M. Tendências da incidência e da mortalidade
por câncer de cólon em residentes no município de São Paulo [dissertação de mestrado]. São Paulo: Universidade de São Paulo, Faculdade de Saúde Pública; 2009. Disponível em http://www.teses.usp.br/teses/ disponiveis/6/6132/tde-08012010-152638/ (Acessado em 20 de janeiro de 2016).
22. Wynder EL, Shigematsu T. Environmental factors of cancer of the colon and rectum. Cancer 1967; 20(9): 1520-61.
23. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Avaliação de Efetividade de Programas de Atividade Física no Brasil. Brasília: Ministério da Saúde; 2011.
24. Reis RJ, Santos MO, Bloch KV. Colorectal cancer in Porto Alegre and Fortaleza, Brazil: incidence trends and distribution pattern from 1990 to 1999. Cad Saúde Pública 2009; 25(5): 1046-53.
25. Brasil. Ministério da Saúde. Instituto Brasileiro de Geograia e Estatística (IBGE). Síntese de indicadores sociais: uma análise das condições de vida da população brasileira 2010. Disponível em: http://biblioteca.ibge. gov.br/visualizacao/livros/liv45700.pdf (Acessado em 18 de novembro de 2011).
26. Cunha JMP. Migração do Centro-Oeste Brasileiro: as tendências e características do período 1986/96. In: Hogan DJ, Carmo RL, Cunha JMP, Baeninger R. Migração e ambiente no Centro-Oeste. Campinas: NEPO; 2002. p. 89. 27. Kohlhepp G, Blumenschein M. Brasileiros sulistas como atores da transformação rural no Centro-oeste brasileiro: o caso de Mato Grosso. Território 2000; 5(8): 47-66. 28. Mirra AP. Imigração e câncer em São Paulo. Cad
Saúde Pública 1997; 13(1): 109-10.
29. American Cancer Society (ACS). Cancer Facts & Figures. 2004. Disponível em: http://www.pink-ribbon-pins.com/CancerRates2004.pdf (Acessado em 21 de setembro de 2011).
30. Saika K, Machii R. Time trends in colon, rectum and anus cancer mortality between 1955 and 2008 in Japan, USA and Europe based on the WHO mortality database. Jpn J Clin Oncol 2011; 41(9): 1153. 31. Fang JY, Dong HL, Sang XJ, Xie B, Wu KS, Du PL,
et al. Colorectal Cancer Mortality Characteristics and Predictions in China, 1991-2011. Asian Pac J Cancer Prev 2015; 16(17): 7991-5.
32. Chatenoud L, Bertuccio P, Bosetti C, Levi F, Curado MP, Malvezzi M, et al. Trends in cancer mortality in Brazil, 1980-2004. Eur J Cancer Prev 2010; 19(2): 79-86.
33. Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2016; 0: 1-9. 34. Inra JA, Syngal S. Colorectal cancer in young adults.
Dig Dis Sci 2015; 60(3): 722-33.
35. van Steenbergen LN, Lemmens VE, Louwman MJ, Straathof JW, Coebergh JW. Increasing incidence and decreasing mortality of colorectal cancer due to marked group efects in southern Netherlands. European J Cancer Prev 2009; 18(2): 145-52. 36. Levin B, Lieberman DA, McFarland B, Smith RA,
Brooks D, Andrews KS, Dash C, Giardiello FM, Glick S, Levin TR, Pickhardt P, Rex DK, Thorson A, Winawer SJ; American Cancer Society Colorectal Cancer Advisory Group; US Multi-Society Task Force; American College of Radiolog y Colon Cancer Committee. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin 2008; 58(3): 130-60.
37. Centers for Disease Control and Prevention (CDC). Vital signs: colorectal cancer screening, incidence, and mortality – United States, 2002-2010. MMWR Morb Mortal Wkly Rep 2011; 60(26): 884-9.
Received on: 10/09/2015