Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Original
article
Clinical
and
epidemiological
evaluation
of
patients
with
sporadic
colorectal
cancer
夽
Glaucia
Maria
de
Mendonc¸a
Fernandes
a,b,
Cássia
Veridiana
Dourado
Leme
a,
Mariângela
Torreglosa
Ruiz-Cintra
c,
Érika
Cristina
Pavarino
d,
João
Gomes
Netinho
e,
Eny
Maria
Goloni-Bertollo
d,∗aFaculdadedeMedicinadeSãoJosédoRioPreto(Famerp),SãoJosédoRioPreto,SP,Brazil
bResearchUnitinGeneticsandMolecularBiology(UPGEM),FaculdadedeMedicinadeSãoJosédoRioPreto(Famerp),SãoJosédoRio
Preto,SP,Brazil
cDepartmentofBiologicalSciences,FederalUniversityofTrianguloMineiro(UFTM),Uberaba,MG,Brazil
dDepartmentofMolecularBiology,ResearchUnitinGeneticsandMolecularBiology(UPGEM),FaculdadedeMedicinadeSãoJosédoRio
Preto(Famerp),SãoJosédoRioPreto,SP,Brazil
eColoproctologyService,DepartmentofSurgery,FaculdadedeMedicinadeSãoJosédoRioPreto(Famerp),SãoJosédoRioPreto,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27January2014 Accepted11August2014
Availableonline4September2014
Keywords:
Colorectalneoplasms Epidemiology Riskfactors Clinicalsymptoms
a
b
s
t
r
a
c
t
Background:Thisstudyaimstoperformasurveyonclinicaldata,sociodemographicand riskfactorsfrompatientswithsporadiccolorectalcancer(SCRC)treatedbetween2004and 2008intheColoproctologyServiceofateachinghospitalintheNorth-westernregionofSão Paulo.
Methods:Weanalyzed749medicalrecords.Ofthese,460werefromcoloncancerpatients and289fromrectalcancerpatients.Mostoftheindividualshadwhiteskinandwereaged over62years.Thevariablesthatwereanalyzedincludedgender,age,skincolor, profes-sionaloccupation,alcoholdrinkingandcigarettesmoking,familyhistoryofcancer,and comorbidities.Theidentificationoftheclinical-sociodemographicprofileandriskfactorsin apopulationwiththeSCRCthenorthwestregionofSãoPaulowasperformedtocollaborate withpreventionstrategies.
Results:TheoccurrenceofSCRCdidnotdiffermuchbetweengenders.Themostprevalent professionaloccupationswerethoserelated tohouseholdchores,agriculturaland com-mercialactivities.Amongthecomorbidities,hypertensionandcholelithiasiswerethemost representative.The mostcommondiagnosismethodandtreatment forthemajorityof patientswerecoloscopyandsurgery,respectively.Onaverage,thetimeofthedisease pro-gressionwaseightmonths.Themediannumberoflymphnodesexcisedrangedbetween 11and14.Themostcommonmetastasiswashepatic.
夽
ThestudywascarriedoutattheFaculdadedeMedicinadeSãoJosédoRioPreto(Famerp),SãoJosédoRioPreto,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](E.M.Goloni-Bertollo).
http://dx.doi.org/10.1016/j.jcol.2014.08.001
Conclusion: Theoccurrenceofcolorectalcancerismorefrequentinmen’swhiteskinwith agedover62years.Professionaloccupationseemstobemoreimportantforthoseexposed tocarcinogenicagents.Thistypeoftumormostlyaffectsthedistalregionsofthecolonand rectumwiththeoccurrenceoflivermetastasis.Theaffectedindividualsusuallyhavelow survivalduetoitshighaggressiveness.
©2014SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Avaliac¸ão
clínica
e
epidemiológica
de
pacientes
com
câncer
colorretal
esporádico
Palavras-chave:
Neoplasiascolorretais Epidemiologia Fatoresderisco Sintomasclínicos
r
e
s
u
m
o
Experiência: Opresenteestudotemcomoobjetivorealizarumlevantamentodedados clíni-cosefatoressociodemográficosederiscodepacientescomcâncercolorretalesporádico (CCRE)tratadosentre2004e2008noServic¸odeColoproctologiadeumhospital-escolana regiãoNoroestedeSãoPaulo.
Métodos: Foramanalisados749prontuáriosclínicos.Destes,460foramdepacientescom câncerdecólonede289depacientescomcâncerretal.Amaioriadosindivíduoserada rac¸abranca,commaisde62anosdeidade.Asvariáveisanalisadasforamgênero,idade,cor dapele,ocupac¸ãoprofissional,consumodeálcooletabagismo,históriafamiliardecâncere co-morbidades.Aidentificac¸ãodoperfilclínico-sociodemográficoedosfatoresderiscoem umapopulac¸ãocomCCREnaregiãonoroestedeSãoPaulofoirealizadaparacolaborarcom asestratégiasdeprevenc¸ão.
Resultados: AocorrênciadeCCREnãodiferiumuitoentregêneros.Asocupac¸ões profission-aismaisprevalentesforamasrelacionadasaosafazeresdomésticos,atividadesagrícolas ecomerciais.Entreascomorbidades,hipertensãoecolelitíaseforamasmais representati-vas.Ométododediagnósticoedetratamentomaiscomumparaamaioriadospacientesfoi colonoscopiaecirurgia,respectivamente.Emmédia,otempodeprogressãodadoenc¸afoide oitomeses.Onúmeromedianodelinfonodosextirpadosvariouentre11e14.Ametástase maiscomumfoiahepática.
Conclusão: Aocorrênciadecâncercolorretalémaisfrequenteemhomensdepelebranca comidadesuperiora62anos.Aocupac¸ãoprofissionalparecesermaisimportantepara aspessoasexpostasaagentescancerígenos.Estetipodetumorafetaprincipalmenteas regiõesdistaisdocólonedoreto,comaocorrênciademetástasesnofígado.Geralmente,os indivíduosafetadosexibembaixasobrevida,devidoàaltaagressividadedessaneoplasia.
©2014SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Background
Sporadiccolorectalcancer(SCRC)isatermformalignant neo-plasmsthatarenotafamilialorinheriteddisease,whichoccur inthelargeintestine(colon)andrectum.1 Itoftendevelops initiallyasanadenomatouspolyp.2–6
This type of cancer is the second most common in Westerncountries.3,7In2012,astudyconductedbythe Brazil-ianNational CancerInstitute (BNCI)reportedan estimated 518,510newcasesofcancerinthecountry.Ofthese, approxi-mately30,000werecolorectalcancer.Itranksfifthasthemost frequentcauseofdeathinBrazil.Approximately14,180cases inmenand15,960casesinwomenarenewlydiagnosedeach year.1
The carcinogenesis of colorectal and rectum cancers involvethe interactionbetweenenvironmentaland genetic
factors.8,9Someriskfactorsarewell-established,suchasage over50 years,1,9–12 lifestylehabits,suchashighlysaturated fattyaciddietandredmeat,1,3,7,8,10alcoholconsumption,and smoking,2,8,9,11 besidescomorbidities,suchascholelithiasis, metabolicsyndrome,anddiabetes.
Signsandsymptomsofcolorectalcanceroccuraccording totheanatomicalregionaffected.SCRCalsodependsonits physiologyandclinicalparameterssuchassize,extent,and spreadoftheneoplasia.Itisacharacteristicofthistumorto presentintestinalobstruction,bleeding(hematochezia, enter-orrhagia),changeinbowelhabits,andsystemicsettingssuch assignificantweightloss.1,3,12,13
is the prevention through an early diagnosis by means of a physical examination performed by a proctologist, laboratory tests (fecal occult blood test, carcinoembryonic antigen CEA test), and imaging screenings (colonoscopy, proctosigmoidoscopy)1,3; and the tertiary phase isthe pre-ventionofsporadicSCRC withrelief ofthe symptomsand preventionofconsequences.7
InBrazil thereisashortage ofdetailed population data in SCRC. Therefore the present study aims establish the clinical–sociodemographicprofileandriskfactors ina pop-ulationwiththeSCRCthenorthwestregionofSãoPauloto collaboratewithpreventionstrategies.
Methods
ThestudywasapprovedbytheLocalEthicsCommittee(CEP) –SãoJosédoRioPretoMedicalSchool–FAMERP(n◦216/2009). Were included in the study, the clinical reports of all patientswhohadaclinicaldiagnosisand/or histopatholog-icalofcoloncancerbythephysicianinColoproctologyService ofauniversityhospitalintheregionnorthwestofSãoPaulo. Were excluded patients havingfamily members diagnosed withcancerorcasesofhereditarycolorectalcancer,according toevaluationofColoproctologyservice.
Thevariables that were analyzed included gender, age, skin color, professional occupation, alcohol drinking and cigarettesmokingand comorbidities.Skincolorwas classi-fiedaswhiteornon-white;weconsideredindividualswhose skin color was non-white as Grayish-browns, Blacks and Yellows.
Weconsideredsmokersthosepatientswhosmokedovera 100cigarettesandalcoholicsthosepatientswhodrankmore thanfourdrinksperweekforsixmonthsorlonger.8
Byanalysingthemedicalrecords,weobtainedthe follow-ingclinicaldata:symptomatology,comorbidities,primarysite oftumor, location ofthetumor thatwere classified inthe largeintestineaseitherproximal(cecum,ascendingor trans-versecolon)ordistal(descendingcolon,sigmoid,rectosigmoid junctionorrectum),clinical stage,levelofhistologic differ-entiation,andpatientsurvival.StagingofDukesisclassified inStageA(growth limitedtothe walloftherectum with-outextensiontooutsidetherectaltissuesandwithoutlymph nodesmetastasis),StageB(growthextendsthroughthewall intheoutsidetherectaltissues,butthelymphnodesarefree ofmetastasis),StageC(lymphnodesinvolvedwithtumor)and stageD(distantmetastasis).14
Astler-CollerconsidersstaginginStageB1andB2 (respec-tively,incompleteandcompletepenetrationofthemuscularis propria),B3 (complete penetrationofthe distal muscularis propria),StagesC1(absenceoflymphnodes), C2(presence oflymph nodes), C3(presence oflymph nodes affected in the ligation point proximal vascular) and stage D (distant metastasis).14
Currentlytheclassificationadoptedinaccordancewiththe InternationalUnionControlCancer(UICC),issuedin2002,the clinicalstaging(TNM),usedtoanalyzetheaggressivenessof tumors,isdividedintostagesIthroughIV.Tumorswere clas-sified accordingtothe TNMfollowingthreecriteria: tumor
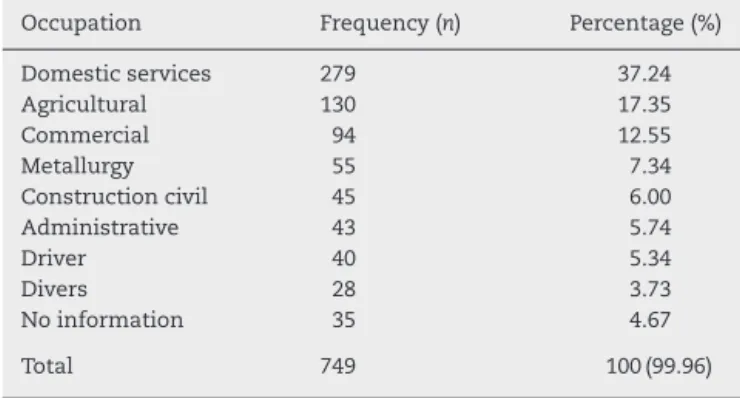
Table1–Percentdistributionofoccupationalactivities.
Occupation Frequency(n) Percentage(%)
Domesticservices 279 37.24
Agricultural 130 17.35
Commercial 94 12.55
Metallurgy 55 7.34
Constructioncivil 45 6.00
Administrative 43 5.74
Driver 40 5.34
Divers 28 3.73
Noinformation 35 4.67
Total 749 100(99.96)
extent(T),presenceoflymphnodeinvolvementregional(N) andpresenceofdistantmetastasis(M).14,15
Thedatawereanalyzedbydescriptivestatistics,usingthe Excelsoftware(version2007).
Results
Weanalyzedthemedicalrecordsof749patients.Ofthese,460 wereaffectedbycoloncancer(GroupI)and289byrectalcancer (GroupII).
GroupIwascomposedof212women(46.08%)and248men (53.91%).GroupIIincluded135women(46.71%)and154men (53.28%).Themeanageatdiagnosisforcoloncancerpatients andrectalcancerpatientswas63years(±14.7)and62.6(±14.5) years,respectively.
Regarding skincolor,the groupofcolon cancerpatients included181whiteindividuals(91.87%),whileinthegroupof rectalcancerpatients,only54.63%werewhite.
Theassessmentofthepatients’ professionaloccupation showed a higher frequency of individuals whose working activities related tohousehold chores(37.24%),agricultural (17.35%)andcommercialactivities(12.55%).Thepercentages allocatedtotheoccupationactivitiesareshowninTable1.
Smokinghabitwasobservedin26.90%and26.82%ofthe patientsinGroupsIandII,respectively.Alcoholaddiction cor-responded to20.81% inthe first and 20.48%in the second group.
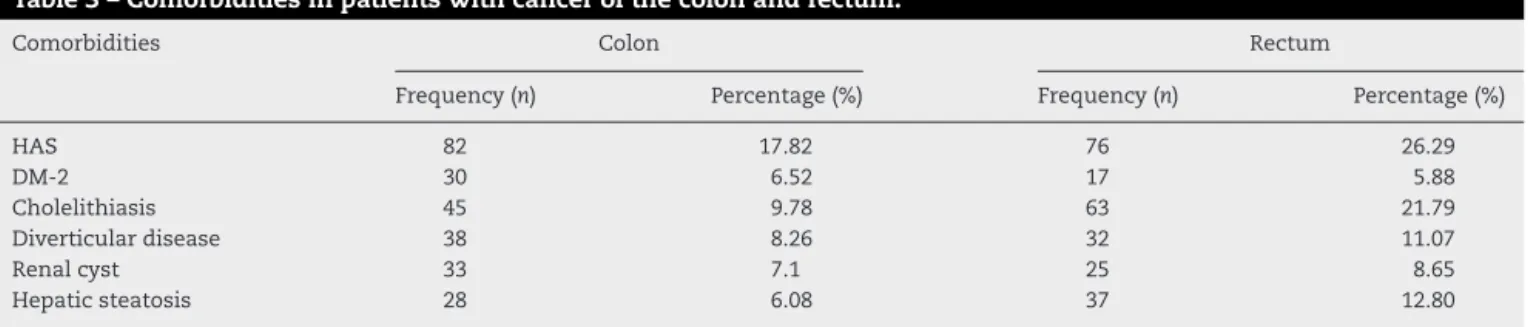
Themostcommonsymptomspresentedbypatientswith colon cancer were intestinal obstruction (10%), bleeding (8.91%),andabdominalpain(8.26%).Amongthosewho pre-sented neoplasia inthe rectum,bleeding(32.17%),diarrhea (14.53%),andweightloss(8.99%)wherepredominant(Table2). Themostprevalent comorbiditiesareshown inTable3. Inwhichthemostfrequentwasthesystemichypertension presentinpatientswithcoloncancer(17.82%)andinpatients withrectalcancer(26.29%)followedbycholelithiasis,9.78% and21.79%,inpatientswithcancerofthecolonandrectum, respectively.
Theoccurrenceofcanceraccordingtotheprimarytumor sitewaspredominantintherectum(41.70%).Signsand symp-tomsvaryaccordingtotheanatomicalregion.
Table2–Signsandsymptomsreportedinthefirstconsultation,inaccordancewiththeanatomicalgroups.
Signsandsymptoms Colon Rectum
Frequency(n) Percentage(%) Frequency(n) Percentage(%)
Bleeding 41 8.91 93 32.17
Abdominalpain 38 8.26 10 3.46
Diarrhea 22 4.78 42 14.53
AAObstructive 46 10 13 4.49
Weightloss 21 4.56 26 8.99
Stoolstape 6 1.30 6 2.07
AAInflammatory 6 1.30 0 0
Anemia 7 1.52 0 0
AA,acuteabdomen.
with colon cancer, 75.70% had neoplasms in stage III and IVequally distributed by genderof which about one third died.Forindividualswithrectumcancer,colonoscopywasthe methodofdiagnosisof52.68%ofpatients.Ofthese,62.96% hadtumorsinstagesIandIIequallydistributedbygenderof which44.11%ofthepatientsdied.
The mean age of the patients at death was 67.8 years (±15.21)and68years(±15.34)inGroupsIandII,respectively. Thetimebetweendiagnosisanddeathwascorrespondingly4 and5months(±8.31)and9.8months(±12.25)inGroupsIand II,respectively.
Thecoexistenceofcancerandadenomawasidentifiedin 46and27patientsinGroupsIandII,respectively.The pre-dominanthistologicaltypewastheadenocarcinoma,which represented 88.83% of colon cancers and 93.65% of rectal cancers.Insomecases,histologicalidentificationwasnot pos-sible.
Regardingthetreatment,surgerywasperformedin77.15% ofpatientsinthefirstgroupand65.85%inthesecondgroup.In addition,chemotherapywasperformedusing5-fluorouracilin combinationwithfolinicacidin47.20%and55.12%ofpatients inGroupsIandII,respectively.
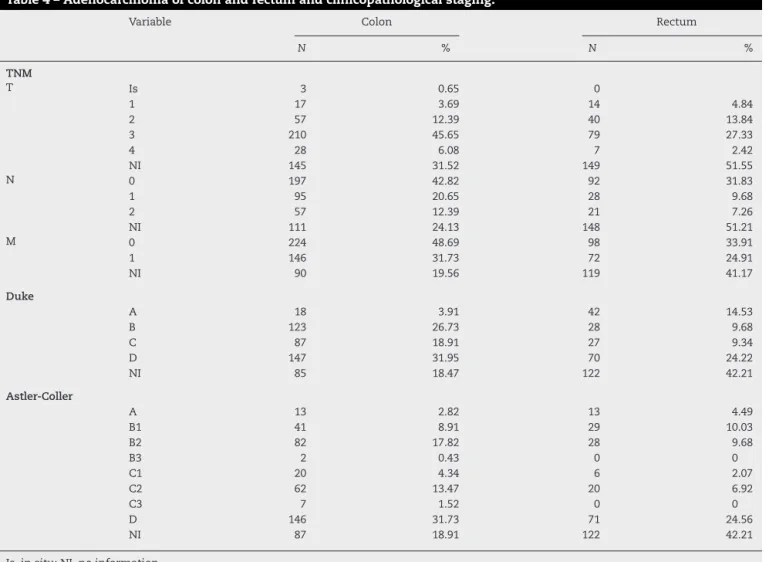
Theinitialclinicopathologicalstages(TNM)ofcolonand rectalcancersareshowninTable4.Themediannumberof lymph nodes parched during surgery for histopathological analysiswas14and11incolonandrectalsurgery,respectively. Themainsitesofdisseminationofpatientswhopresented metastatic colon cancer were liver (64.51%), peritoneum (19.35%),andlung(9.67%);amongthemetastasesobservedin rectalcancerpatients, theliverwas alsothemostaffected organ (54.11%), followed by the peritoneum (12.94%), lung
(11.76%),bone (8.23%),central nervoussystem (5.88%), and urinarysystem(7.05%).
Discussion
OurfindingsshowedthattheoccurrenceofSCRCdidnotdiffer betweengender,whichcorroboratesotherstudiesthatalso reportasimilardistributionbetweenmenandwomen1,5,6,16; althoughSantosetal.5observedahigherincidenceofcolon cancerinwomenandrectalcancerinmen.5
Steele etal.16reportedapredominanceofoccurrenceof SCRCinwhite-skinnedindividualswithpercentageragingup to80%.Ourstudy foundsimilarresultsinrelationtocolon cancer(91.87%)andshowedasmallerpercentage(54.63%)in rectalcancer.Otherstudies haveshownahigherincidence andsurvivalofsporadicSCRCamongAfrican-Americans.16,17 ItisworthmentioningthattheBrazilianpopulation,whichis representativeofourstudy,hasanethniccompositionwith greatconfluenceofseveralotherethnicgroups,makingit dif-ficulttoanalyzetheinfluenceofthisvariable.
Itisestablishedintheliteraturetheageof50yearsasrisk factorfordevelopingsporadicSCRC.1,5,9,10,12,18 Corroborated withtheliterature,inourstudy,themeanageatdiagnosis was63years(±14.7)forpatientswithcoloncancerand62.6 years(±14.5)forpatientswithrectalcancer.
Regarding theprofessional occupation,our datashowed a predominance of SCRC in those who perform activities related to household chores, agricultural and commer-cial activities. In fact, the exposure to some carcinogenic agents used in agriculture, and in some industries is
Table3–Comorbiditiesinpatientswithcancerofthecolonandrectum.
Comorbidities Colon Rectum
Frequency(n) Percentage(%) Frequency(n) Percentage(%)
HAS 82 17.82 76 26.29
DM-2 30 6.52 17 5.88
Cholelithiasis 45 9.78 63 21.79
Diverticulardisease 38 8.26 32 11.07
Renalcyst 33 7.1 25 8.65
Hepaticsteatosis 28 6.08 37 12.80
Table4–Adenocarcinomaofcolonandrectumandclinicopathologicalstaging.
Variable Colon Rectum
N % N %
TNM
T Is 3 0.65 0
1 17 3.69 14 4.84
2 57 12.39 40 13.84
3 210 45.65 79 27.33
4 28 6.08 7 2.42
NI 145 31.52 149 51.55
N 0 197 42.82 92 31.83
1 95 20.65 28 9.68
2 57 12.39 21 7.26
NI 111 24.13 148 51.21
M 0 224 48.69 98 33.91
1 146 31.73 72 24.91
NI 90 19.56 119 41.17
Duke
A 18 3.91 42 14.53
B 123 26.73 28 9.68
C 87 18.91 27 9.34
D 147 31.95 70 24.22
NI 85 18.47 122 42.21
Astler-Coller
A 13 2.82 13 4.49
B1 41 8.91 29 10.03
B2 82 17.82 28 9.68
B3 2 0.43 0 0
C1 20 4.34 6 2.07
C2 62 13.47 20 6.92
C3 7 1.52 0 0
D 146 31.73 71 24.56
NI 87 18.91 122 42.21
Is,insitu;NI,noinformation.
relatedtotheSCRC,suchasdichlorodiphenyltrichloroethane (DDT),dichlorodiphenyldichloroethylene(p,p′-DDE),and
poly-chlorinated biphenyl (PCB).19 In our study, however, the investigationofsuchexposureswasnotpossible.
Severaletiologicalfactorsresultingfromtheinteractionof environmentalandgeneticfactorsareinvolvedinthe devel-opment ofcolon and rectal cancers. Amongthem wecan mentionfamilyhistory,alcoholdrinkingandsmoking,3,8,9 a highly saturated fat diet and red meat,1,6,20 and the pres-enceofcomorbidities,suchascholelithiasis,20–22 metabolic syndrome,23typeIIdiabetes,20,24,25andobesity.26,27
SmokinghabitisariskfactorforSCRC,28,29andits occur-renceseemstoreflectmoreonthebuildingupoftheamount ofyearlyexposurethan onthetimeofexposure,29–31 espe-ciallyinrectalcancer.31 Alcoholdrinkingincreasesthe risk of developing SCRC in individuals who drink 30–45g/day, and especially those who ingest more than 45g/day.32 An increasedrisk ofthose who drink more than 100g/week33 has also been demonstrated. Genetic polymorphisms of enzymes that act on the metabolism of ethanol, folate, and DNA repair together, these factors may determine a genotoxic effect and also act as a solvent to tobacco car-cinogens and also, which might induce the production of free radicals34 and decrease the absorption of folate in alcoholics;32 also, they would stimulate the production
of free radicals34 and decrease the absorption of folate in alcoholics.32 Smoking and drinking were observed in our study; however, it was not possible to determine the amount ofexposureduetothe retrospective natureofthe study.
Regardingthediet,althoughstudiesarestillcontroversial, itisnotoriouslyknownthatfruits,leguminousplants,green vegetables,anddairyproductsplayaprotectiveroleagainst cancerofthealimentarysystem.Ontheotherhand,excessive intakeofmeatandanimalfatisnotrecommended.1,7,9Wedid notevaluatedthefoodhabitsinourstudy.Asitisareviewof medicalrecords,thesedonotshowthisinformation.
Amongothercomorbiditiesassociatedwiththe develop-mentofsporadicSCRCarehyperinsulinemia,obesity,24,25and metabolicsyndrome.23 Thelatterisalsorelatedtoahigher incidenceoflivermetastasisandtumorrecurrence.Italsois aprobableindependentfactorofworseprognosisinsurvival ofpatientswiththistypeofneoplasm.35
Theweightgaininbothgenderhasbeenassociatedwith an increasedrisk of SCRC, although the body massindex incrementdoes notseemtocontributetothe development ofthisneoplasia.21,27 Thus,itbecomesimportanttoidentify individualswithmetabolicsyndrome.Theymayrepresenta populationsusceptibletothe developmentofSCRC.Inour study,wewereunabletoassessthefrequencyofmetabolic syndromeamongthosewhodevelopedthistypeofneoplasia. Regardingthemostaffectedanatomicalregion,ourstudy found a higher incidence of SCRC in the rectum, which isconsistent withthe findings ofother studies.5,6 As each anatomicalregion presents distinct embryological develop-ment and physiology when exposed to carcinogens, the mechanismofdevelopmentofneoplasiaaswellasthe symp-tomspresentedbythepatientineachanatomicalsegment ispeculiartotheirlocation.Thus,thecorrectidentification oftheprimarysiteoftumordevelopmentisofvital impor-tancetoassistinthechoiceoftreatmentamongthedifferent therapeuticapproaches.36
Symptoms of SCRC are expressed according to tumor location in association with the anatomy and physiology of the affected region, such as an obstruction, bleeding (hematochezia,enterorrhagia),change inbowelhabits, and significant weight loss,1,3,12,13,37 and these symptoms may helpintheearlydetectionofthisneoplasm.38Inthisstudy, as found in the literature, the most common symptoms presented by patients with colon cancer were intestinal obstruction,rectalbleeding,andabdominalpain.1,37,38
Colonoscopyisanimportantadditionaltestforthe detec-tion of SCRC and as well as of its precursor lesion, the adenoma.Whenidentifiedatanearlystage,afive-year sur-vivalappearstobegreaterthan90%.37,39,40Someprotocols, suchastheEPAGEII,whichwasdevelopedinEurope, deter-minethescreeningmethodtobeperformed.Itisbasedon thesymptomatologyaswellasonthepresenceofriskfactors andageofthepatient.39Thus,coloscopy,thegoldstandard fordetectionofSCRC,actsatthesecondarypreventionlevelof cancer,39,40anditrepresentsanimportanttoolusedinpublic healthprograms.Inthisstudy,54.31%ofpatientswithcolon cancerand52.68%ofpatientswithrectalcancerwere sub-jectedtothistest.Thispercentagereflectsthefactthatthe majority(75.70%)ofthemwasreferredtotheColoproctology Serviceinanadvancedstageoftheneoplasticprocess(T3and T4).
Thepredominant histological malignant neoplasm type inourstudywastheadenocarcinoma(88.83%ofcolon can-cers and 93.65% of rectal cancers). It is responsible for more than 90% of the cases reported in the literature.2,3 Becausethe adenoma is typically a premalignantlesion,36 its early detection is of utmost importance, since it is an independentriskpredictorfortheSCRC.41Otherhistological malignant neoplasm types, including mucinous adenocar-cinoma(17%), ofwhich 2–4% are squamoussignet-ring cell carcinoma, squamouscell carcinoma, and undifferentiated carcinoma.3
Among the therapeutic options available for colorectal cancer,chemotherapystandsout,whosetoxicityisvariable according to the agent applied and that can decrease the quality of life of patients in relation to psychological and physical activity.42,43 Currently, the public health network
usesanassociationbetween5-fluorouracilandfolinic acid-leucovorin.38 This drug therapy has been associated with improvedsurvivalanddecreasedtumorrecurrenceinpatients undergoing this therapeuticregimen.36,43,44 Althoughthere areotherdrugsthathaveshownasignificantimprovementin thesepatients’survival,suchasthebevacizumab.36,42,43Inour study,47.20%ofthecoloncancerpatientsand55.12%ofthe rectalcancerpatientsunderwentchemotherapyusingmainly 5-fluorouracilandfolinicacid.
Anothertherapeuticmethodusedisthesurgicalresection of thetumor associatedwiththe removal oflymph nodes foradequatestaging.40Internationalconsensusandscientific papersrecommendanevaluationofatleast12regionallymph nodesintheanatomicalsampleduringthecurativetreatment bysurgery,inordertoobtainmorereliabledataforthe appro-priateclinicalstaging.18,45Inourstudy,weobservedthatthe procedureperformedatourinstitutionisinaccordancewith thatestablishedintheliterature,sincethemediannumberof lymphnodesresectedwas14incolonsurgeryand11inrectal surgery.
Regardingthesystemicdisseminationofcolonandrectal cancers,theliteratureindicatesthatthemainmechanismof tumorspreadoccursviaahematogenouspathwayand,toa lesserextent,bythelymphaticroutewithpossible implan-tation oftumorcells inorgans suchas liver, lungs, bones, cerebrum,ovaries,andskin.2,18Additionally,the dissemina-tionofneoplasticcellscanoccurbycontinuity,whichhappens throughthewalloftheorgans.2,12,19Inthisstudy,wefounda higherincidenceoflivermetastases,followedbythose affect-ingtheperitoneum,lung,bones,centralnervoussystem,and urinarysystem.
In2004,Tucunduvaetal.46 conductedastudy with non-oncologistsphysiciansatahealthserviceinordertoassess their knowledge and attitude toward preventive measures forthemostcommoncancers.Itwashighlightedthatthese physicians showed interest in the prevention of various cancers,buttheyhaddifficulty incarryingoutthe counsel-ing recommended by the consensus.47 Thus, the study of colorectal cancerisrelevantbecauseabetterknowledgeof preventivemeasures,riskfactors,associatedsignsand symp-toms,researchmethods,andappropriatetimeforreferralto specialists,includinggeneralpractitionerscontributetothe reductionofsurvivalmorbidityandimprovepublichealthand qualityoflife.
Conclusion
Funding
PIBIC/CNPq, Assistance Researcher (BAP) – FAMERP, CNPq, FAMERP-FUNFARME.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. InstitutoNacionaldoCâncer(INCA).Availablefrom:
http://www.inca.gov.br(accessed01.05.12).
2. GiurizatoCSB,AreiasMAC.Estudodaprevalênciadecâncer colorretalnoperíodode2005emumhospitaldoSistema ÚnicodeSaúdenacidadedeDourados-MS.Interbio. 2008;2:21–8.
3. ZampinoMG,LabiancaR,BerettaGD,MagniE,GattaG, LeonardiMC,etal.RectalCancer.CritRevOncolHematol. 2009;70:160–82.
4. CeratoMM,CeratoNL,MeurerL,EdelweissaMI,PüttenAC, GolbspanL.VariabilidadeInterobservadornoDiagnóstico HistológicodosPóliposColorretais.RevBrasColoproct. 2007;27:007–15.
5. SantosJR,MJC.Câncerano-reto-cólico:aspectosatuaisIII– câncerdereto–terapêuticaneoadjuvante.RevBras Coloproct.2008;28:108–11.
6. CruzGMG,FerreiraRMRS,NevesPM.CancerRetal:Estudo Demográfico.DiagnósticoeEstadiamentode380Pacientes AcompanhadosaoLongodeQuatroDécadas.RevBras Coloproct.2004;24:208–24.
7. PinhoM,RossiBM.Conceitosatuaissobreacarcinogênese colorretal.RevBrasColoproct.1999;19:57–60.
8. GertigDM,HunterDJ.Genesandenvironmentintheetiology ofcolorectalcancer.CancerBiol.1998;8:285–98.
9. RoginCC,ModugnoF,GollinSM.Theepidemiologyandrisk factorsofheadandneckcancer:afocusonhuman papillomavirus.JDentRes.2007;86:104–14.
10.GiacosaA,RondanelliM,CenaH,FrascioF,HillMJ.Dietand colorectalcancerrisk:currentviews:currentviews.Ann Gastroenterol.2002;15:324–32.
11.MallmannACM,KoshimizuRT,CarvalhoLP,MuxfeldtRA. Rastreamentodocâncercolorretal.MomPerspecSaúde. 2003;16:13–5.
12.DinizBSO,Lacerda-FilhoA.Prevenc¸ãosecundáriadocâncer colorretalemindivíduosdebaixorisco.RevMedMinas Gerais.2004;14:46–52.
13.CapelhuchnikP,NadalCRM,BianchiniPA,BinFC,KlugWA. Sinaissintomasdocâncercolorretalediagnósticoprecoce. RevbrasColo-Proct.1991;11:125–7.
14.KeighleyMRB,WilliamsNS.Cirurgiadoânus,retoecolo.São Paulo:Manole;1998.p.811–4.
15.InstitutoNacionaldoCâncer.UICC–UniãoInternacional ContraoCâncer,2002–TNM–Classificac¸ãodeTumores Malignos.6a
.Ed.RiodeJaneiro:INCA;2004.
16.SteeleSR,BrownTA,RushRM,MartinMJ.Laparoscopicvs opencolectomyforcoloncancer:resultsfromalarge nationwidepopulation-basedanalysis.JGastrointestSurg. 2008;12:583–91.
17.PoliteBN,DignamJJ,OlopadeOI.Colorectalcancerandrace: understandingthedifferencesinoutcomesbetweenAfrican Americanandwhites.MedClinNorthAm.2005;58:771–93.
18.ByrneLH,JankuF,BirdBR,O’KeeffeJ,O’MurchuE,
O’CallaghanL,etal.Thecorrelationbetweenthenumberof
lymphnodesidentifiedandtreatmentoutcomesincolorectal patients:single-institutionexperience.JClinOncol.2010;28: e14096.
19.ChenK,ZhaoYW,MaXY,ZhangLJ,ZhengS.Relationship betweenorganochlorinepollutioninsoilandriceandthe incidenceofcolorectalcancerinJiashancounty,Zhejiang province.ZhonghuaLiuXingBingXueZaZhi.2004;25: 479–83.
20.HuangCW,SunLC,ShihYL,TsaiHL,ChenCW,YehYS,etal. Theimpactonclinicaloutcomeofhighprevalenceof diabetesmellitusinTaiwanesepatientswithcolorectal cancer.WorldJSurgOncol.2012;10:76.
21.SilvaEJ,PelosiA,AlmeidaEC.Índicedemassacorpórea, obesidadeabdominaleriscodeneoplasiadecólon:estudo prospectivo.RevBrasColoproct.2010;30:199–202.
22.GoldacreMJ,AbisgoldJD,SeagroattV,YeatesD.Cancerafter cholecystectomy:record-linkagecohortstudy.BrJCancer. 2005;92:1307–9.
23.SiddiquiAA.Metabolicsyndromeanditsassociationwith colorectalcancer:areview.AmJMedSci.2010[Epubaheadof print].
24.MatthewsCE,SuiX,LaMonteMJ,AdamsSA,HébertJR,Blair SN.Metabolicsyndromeandriskofdeathfromcancersofthe digestivesystem.Metabolism.2010;59:1231–9.
25.CostaFO,RochaGZ,DiasMM,CarvalheiraJBC.Mecanismos epidemiológicosemolecularesqueassociamobesidadee câncer.ArqBrasEndocrinolMetabol.2009;53:145–50.
26.ShenZ,YeY,BinL,YinM,YangX,JiangK,etal.Metabolic syndromeisanimportantfactorfortheevolutionof prognosisofcolorectalcancer:survival,recurrence,andliver metastasis.AmJSurg.2010;200:59–63.
27.EngelandA,TretliS,AustadG,BjorgeT.Heightandbody massindexinrelationtocolorectalandgallbladdercancerin twomillionNorwegianmenandwomen.CausesCancer Control.2010;1:987–96.
28.LoAC,SolimanAS,KhaledHM,AboelyazidA,GreensonJK. Lifestyle,occupational,andreproductivefactorsandriskof colorectalcancer.DisColonRectum.2010;53:830–7.
29.BoyleP,LeonME.Epidemiologyofcolorectalcancer.BrMed Bull.2002:641–725.
30.LüchtenborgM,WhiteKKL,WilkensL,KolonelLN,Marchand LL.Smokingandcolorectalcancer:differenteffectsbytypeof cigarettes?CancerEpidemiolBiomarkersPrev.2007;16:1341–7.
31.LiangPS,ChenTY,GiovannucciE.Cigarettesmokingand colorectalcancerincidenceandmortality:systematicreview andmeta-analysis.IntJCancer.2009;124:2406–15.
32.LinOS.Acquiredriskfactorsforcolorectalcancer.Methods MolBiol.2009;472:361–72.
33.MoskalA,NoratT,FerrariP,RiboliE.Alcoholintakeand colorectalcancerrisk:adose–responsemeta-analysisof publishedcohortstudies.IntJCancer.2007;210:664–71.
34.BoffettaP,HashibeM.Alcoholandcancer.LancetOncol. 2006;7:149–56.
35.OhSW,KimYH,ChoiYS,ChangDK,SonHJ,RheePL,etal. Thecomparisonoftheriskfactorsandclinical
manifestationsofproximalanddistalcolorectalcancer.Dis ColonRectum.2008;51:56–61.
36.SchernhammerES,LeitzmannMF,MichaudDS,SpeizerFE, GiovannucciE,ColditzGA,etal.Cholecystectomyandthe riskfordevelopingcolorectalcanceranddistalcolorectal adenomas.BrJCancer.2003;88:79–83.
37.SantosJCM.CâncerAno-Reto-Cólico:AspectosAtuaisII– CâncerColorretal–FatoresdeRiscosePrevenc¸ão.RevBras Coloproct.2007;27:459–73.
39.ProjetoDiretrizes–Associac¸ãoMédicaBrasileiraeConselho FederaldeMedicina.Diagnóstico,EstadiamentoeTratamento CirúrgicoeMultidisciplinardoCâncerColorretal;2001. 40.JuilleratP,Peytremann-BridevauxI,VaderJP,ArditiC,
SchusseléFilliettazS,DuboisRW,etal.Appropriatenessof colonoscopyinEurope(EPAGEII)–presentationof
methodology,generalresults,andanalysisofcomplications. Endoscopy.2009;41:240–6.
41.Bixquert-JimenezM.Selectivecolorectalcancerscreeningin average-riskpopulations.RevEspEnfermDig.2009;101:821–5.
42.KaminskiMF,RegulaJ,KraszewskaE,PolkowskiM, WojciechowskaU,DidkowskaJ,etal.Qualityindicatorsfor colonoscopyandtheriskofintervalcancer.NEnglJMed. 2010;362:1795–803.
43.RoqueVMN,ForonesNM.Avaliac¸ãodaqualidadedevidae toxicidadesempacientescomcâncercolorretaltratadoscom
quimioterapiaadjuvantebaseadaemfluoropirimidinas.Arq Gastroenterol.2006;43:94–101.
44.TononLM,SecoliSR,CaponeroR.Câncercolorretal:uma revisãodaabordagemterapêuticacombevacizumabe.Rev BrasCancerol.2007;53:173:182.
45.WolpinBM,MayierRJ.Systemictreatmentofcolorectal cancer.Gastroenterology.2008;134:1296–331.
46.TucunduvaLTCM,SáVHLC,KoshimuraET,PrudenteFVB, SantosAF,SamanoEST,etal.Estudodaatitudeedo conhecimentodosmédicosnãooncologistasemrelac¸ãoàs medidasdeprevenc¸ãoerastreamentodocâncer.RevAssoc MedBras.2004;50:257–62.