w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Prognostic
impact
of
the
number
of
resected
lymph
node
on
survival
in
Colorectal
Cancer
Katia
M.
Ladeira
a,b,
Sandra
Fátima
Fernandes
Martins
a,b,c,∗aUniversidadedoMinho,EscoladeCiênciasdaSaúde,Braga,Portugal
bLifeandHealthSciencesResearchInstitute/3B’s(ICVS/3B’s),PTGovernmentAssociateLaboratory,Braga/Guimarães,Portugal cCentroHospitalardeTrás-os-MonteseAltoDouro,UnidadedeChaves,DepartamentodeCirurgia,VilaReal,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15January2016 Accepted4April2016 Availableonline26April2016
Keywords:
ColorectalCancer Lymphnodes Staging Survival
a
b
s
t
r
a
c
t
Introduction:ColorectalCancer(CRC)isthethirdmostcommoncancerandthesecond lead-ingcauseofdeathinWesterncountries.InPortugal,intheNorth,emergesasthesecond mostcommoncancer.Thepresenceoflymphnodemetastasisisanimportantpredictor ofoverallanddisease-freesurvivalandseveralstudiesrecommendtheevaluationofat least12–14regionallymphnodes,asitcontributestoimprovecancerstagingandpatient outcomes.
Aims:Epidemiologicalcharacterizationofthestudiedpopulationandidentifyapossible relationshipbetweenthenumberoflymphnodesevaluatedinthesurgicalspecimenand survival.
Methods:Weprecededtothestudyof1065CCRpatients,submittedtosurgicalresection between1January2000and31August2012,inBragaHospital.
Discussion/Conclusion:Theresultsoftheepidemiologicalcharacterizationofthispopulation arecoincidentwiththosedescribedintheliterature.Itwasobservedasignificant correla-tionbetweenage,tumorsize,serosalinvasion,differentiation,tumorpenetration,venous andlymphaticinvasion,metastasis,TNMstageandthenumberoflymphnodesevaluated. However,wedidnotobserveastatisticallysignificantcorrelationbetweenpatientsurvival andnumberoflymphnodesevaluated(p>0.05).Apossibleexplanationisthepracticeof oncologists,addressingpatientswithlessthan12nodesidentifiedinthesurgical speci-menas“N-positive”andundergoingadjuvanttherapy.Abetterharvestandcarefulanalysis oflymphnodeswould leadtomoreaccuratestaging,avoidingovertreatmentand side effectsassociated,andallowbettereconomicmanagementofhospitalresources,inreal N0patients.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileirade Coloproctologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](S.F.F.Martins).
http://dx.doi.org/10.1016/j.jcol.2016.04.001
Impacto
prognóstico
do
número
de
linfonodos
ressectados
na
sobrevida
de
pacientes
com
câncer
colorretal
Palavras-chave:
Câncercolorretal Linfonodos Estadiamento Sobrevida
r
e
s
u
m
o
Introduc¸ão: Ocâncercolorretal(CCR)ocupaoterceirolugaremtermosdefrequênciae,além disso,éasegundacausaprincipaldemortenospaísesocidentais.EmPortugal,nonorte, CCRsurgecomoosegundocâncermaiscomum.Apresenc¸ademetástaseaoslinfonodos épreditorimportantedesobrevidaemgeraledesobrevidalivredadoenc¸a;váriosestudos recomendamaavaliac¸ãodepelomenos12–14linfonodosregionais,poistalprocedimento contribuiparaaprimoraroestadiamentodocâncereosdesfechosparaospacientes.
Objetivos:Caracterizac¸ãoepidemiológicadapopulac¸ãoestudadaeidentificac¸ãodepossível relac¸ãoentreonúmerodelinfonodosavaliadosnoespécimecirúrgicoesobrevida.
Métodos: Estudode1065pacientescomCCR,submetidosàressecc¸ãocirúrgicaentre1de janeirode2000e31deagostode2012emumhospitalemBraga.
Discussão/Conclusão: Osresultadosdacaracterizac¸ãoepidemiológicadessapopulac¸ão coin-cidemcomosresultadosdescritosnaliteratura.Foiobservadaumacorrelac¸ãosignificativa entre idade,tamanho dotumor,invasão da serosa, diferenciac¸ão,penetrac¸ão tumoral, invasãovenosaelinfática,metástase,estágioTNMenúmerodelinfonodosavaliados.Mas nãoobservamosumacorrelac¸ãoestatisticamentesignificativaentresobrevidadopacientee númerodelinfonodosavaliados(p>0,05).Umaexplicac¸ãopossíveléapráticados oncologis-tas,quetratampacientescommenosde12nodosidentificadosnoespécimecirúrgicocomo “N-positivos”,prosseguindocomterapiaadjuvante.Umacoletamaisapropriadaeuma análisecuidadosadoslinfonodosresultariaemumestadiamentomaispreciso,evitando otratamentoexcessivoeosefeitoscolateraisassociados,alémdepermitirumtratamento commelhorcusto-benefícioparaosrecursoshospitalaresempacientesrealmenteN0.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade Coloproctologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
TheColorectalCancer(CRC)isthethirdmostcommoncancer andthesecondleadingcauseofdeathintheUnitedStatesand inWesterncountries.1InthenorthofPortugal,itarisesasthe
secondmostcommoncancer,withanincidencerateof41.6%, and34%inthedistrictofBraga.2DatafromtheWorldHealth
Organizationbetween1997and2007revealedthatthe mortal-ityratedeclinedabout 2%peryear:19.7to17.4/100000for men(worldstandardizedrates),andfrom12.5to10.5/100000 forwomenandthis decreaseisduetoearlydiagnosis and treatment,withaconsequentincreaseinsurvival.3
ThestageoftheCRCatdiagnosisistheprimary determi-nant ofsurvivaland the mainpredictor of mortality.4 The
survivalrates atfive years may be higher than 90% if the diagnosis is made at an early stage, however only37% of thecasesarediagnosedatthisstage.5 Lymphnode
metas-tasesareanimportantfactor fortheindicationofadjuvant chemotherapyandperformanimportantpredictorofoverall anddisease-freesurvival.Thereisevidenceofimproved onco-logicaloutcomesandcancerstagingasgreater thenumber oflymphnodesidentified.6,7However,thenumberoflymph
nodesthatshouldbeevaluatedremainscontroversial.8 The
InternationalUnionagainstCancer,the AmericanJoint Commit-teeonCancer,theAmericanCollegeofSurgeonsandtheNational QualityForum consider that isnecessary to reviewatleast twelvelymphnodestoexcludetheachievementofdisease.9,10
In the 7th edition of the AJCC Cancer StagingManual, it is
recommendedtoevaluateatleasttwelvetofourteenregional lymphnodes asaprognosticfactorofCRC, andevaluation offewerthan twelvelymph nodeshavelowdiscriminative power.11Statisticalanalysisshowedthatprobabilityof
find-ing asingle metastasis inlymphnodes increaseswith the numberofnodesanddecreasesabout46%whenonly eigh-teennodesarefound.12Thus,itisrecommendedthatsmall
gangliabetween0.1and0.2cmindiametermustbelocated. Nevertheless,furtherinvestigationsrevealedthatover60%of U.S.institutionsfailinachievingtheproposedtargetofa min-imumoftwelvelymphnodesassessed.13 Someresearchers
believethatradicallymphadenectomyhasabeneficial ther-apeuticeffectwhileothersbelievethatthisonlyprovidesa moreaccuratestaging.14
Factorscontributingtothenumberofnodesevaluated
It has been shown that the relation between the number ofnodes evaluatedand stagingisnotsimple. Threemajor factorsinfluencingthisrelationwereidentified:thehospital (qualityofoncologicalandsurgicalcareandnumberof can-cercases),thepatientcharacteristics(youngerage≤ 60years,
female sex),and tumorproperties (larger size and greater tumor extension (pT), right colon localization, and higher stage).Thesefactorsareassociatedwithhigherlymphnodes achievement.Thus,alownumberofnodesexaminedcanbe anindicatorofpoorsurgicalandoncologicalcare.6,15Among
inresectedspecimens,themethodologyusedin pathologi-calpracticeisthe mostimportant(namelyincollection of lymphnodesand processingformicroscopicexamination). Thenon-uniformity ofthisapproach iscurrentlythe most problematicfactor,15makingtheroleofthepathologist
essen-tialgiventhatanextensivepathologicdiagnosiswillallowa correctstaging.16
Otherfactorscontributingtothevariationinthenumber ofnodescontainedinthesurgicalspecimenarethesurgical techniqueandthevariationsinthespecimensmanipulation: diligenceofsearchforlymphnodes,theuseofsolutionsto increase macroscopic visualization ofnodes; threshold for acceptablenumberoflymphnodesusinghalfversusalllymph nodes found for microscopic evaluation; amount of tissue acquired for observation, and the separation of nodes by anatomicsite.Thus,itisrecommendedthatalllymphnodes found should besectioned, and it has been demonstrated thattwelvetofifteennegativenodesarepredictorsof nega-tiveregionallymphnodeinvasion.Iflessthantwelvenodes arefound,thenadditionaltechniquestoimprovevisualization shouldbeconsidered.15
Anotherfactorinrectalcancerthatinfluencesthe num-berofnodesevaluatedisneoadjuvanttherapy,17,18including
preoperativeradiationtherapy.19Accordingtosomeauthors,
this therapy improves resectability, sphincter preservation and localcontrolofthe disease,althoughits survival ben-efitis controversialsincethe reductionofrecurrence does notnecessarilytranslateintoincreasedsurvivalrate.17,20–22In
addition,theneoadjuvanttherapyisassociatedwith reduc-tionintumormass,but alsowithincreasedtissuefibrosis, which hampers identification of the lymph nodes.23 The
hypothesisthatfewerlymphnodesaredetectedinthe sur-gicalspecimenafterneoadjuvanttherapyhasbeenconfirmed byseveralauthors.24–26Therearecurrentlyno
recommenda-tionsonthe actualnumberoflymphnodes thatshouldbe foundafterneoadjuvant therapy(staging ypN),however in theliteraturethemeannodesfoundvariesbetweenfourand fourteen.27,28
Neoadjuvanttherapyalsoappearstohaveanimportant effectonmesorectallymphnodes,contributingtodecreasein theirsize.29–31Murphyetal.32haveidentifiedthesizeoflymph
nodesasanindependentprognosticindicatorofsurvivalin negativenodesafterprimarysurgery.Itisbelievedthata sig-nificantnumberofmesorectallymphnodesmicrometastases, smallerthan0.5cmarenotdetectedbymanuallymphnodes counting and by typicalpathological diagnosis methods.17
Someauthors concludedthat theabsence ofnodes (ypNx) ordecreasednumberofnodesfoundinpatientswithstage ypN-negativedoesnotimplyapooreroncologicoutcome.The numberofnodes seemstohavenoimpactonsurvivaland recurrenceinpatients’ypN-negative.33Iffewerthantwelve
lymphnodesarefoundandthereisnoopportunitytofind more,adjuvanttherapyisrecommendedinhighrisk situa-tions.Thefailuretoreachaminimummarkoftwelvenodes found is currently used by oncologists in their treatment decisions.17
Giventhecontroversialthemeandtheabsenceofstudies inPortugal,thisstudywasconductedinorderto character-izeepidemiologicallypatientsoperatedbyCRCintheperiod January 1, 2000 to August 31, 2012, at Braga Hospital and
identifies apossiblerelationbetweenthenumber oflymph nodesexaminedandthesurvivalofpatientsoperatedforCRC.
Materials
and
methods
Datafrom1065patientstreatedinBragaHospital,northof Por-tugal,betweenJanuary1,2000,andAugust31,2012withCRC diagnosisandsubmittedtosurgicaltreatmentwascollected retrospectively.
Data collected from clinical and preoperative diagnos-ticexaminationsincludes:age, genderandtumorlocation. Histopathologicalreportsinclude:tumorsize,serosal exten-sion, presenceofsincronetumors,histologicaltype,tumor differentiation,macroscopictumorappearance,tumorextent (T),numberoflymphnodesevaluatedandextentofspread to the lymph nodes (N), lymphatic and blood vessel inva-sion,andTMNstaging.Thelevelofpositivelymphnodeswas notdescribedinallspecimens.Twoexperiencedpathologists determinedthehistologicaltypeofCRCandthetumorstaging wasgradedaccordingtoTNMclassification,6thedition.
All patientswere followedupperiodicallyand their out-comes were investigated and collected until August 2012. Follow-up datarecorded includedrecurrenceofthe disease andtimeofdeath.
Statisticalanalysis
All data was collected and stored inan ExcelPC database andstatisticallyanalyzedusingtheStatisticalPackageforthe SocialSciences,version22.0(SPSSInc.,Chicago,Illinois,USA). Asimpledescriptiveanalysisofeachoneofthevariableswas realized,withdeterminationofthetotalnumberofcasesand relativefrequencies.Themedianandmeanwasdetermined forthenumberoflymphnodesassessed.
Allcomparisonswereexaminedforstatisticalsignificance using Pearson’s chi-square (2)test and Fisher’s exact test
(whenn<5),withthethresholdforsignificancepvalues<0.05. Overallsurvival(OS)wasdefinedastimefromdisease diag-nosisuntildeathfromanycause,anditwasassessedusing theKaplan–Meiermethod.
Ethicscommitteeapproval
ThestudyprotocolwasapprovedbytheEthicsCommitteeof BragaHospital.
Results
1384patientswereidentifiedwiththediagnosisofCRC,and 1065ofthesemettheinclusioncriteriapreviouslydefined.
Table1–Epidemiologicalcharacterizationofpatientsanditsrelationshipwiththemeanandmediannumberoflymph nodesevaluated.
Variable n % Mediannumberof
nodesretrieved
Meannumberof nodesretrieved
Overall 1065 100 11 13
Sex
Female 428 40.2 11 13
Male 637 59.8 11 13
Age(years)
≤71.5 573 53.8 11 14
>71.5 492 46.2 10 12
Location
Rightcolon 243 22.8 13 15
Leftcolon 486 45.6 10 12
Rectum 336 31.5 10 13
Tumorsize(cm)
≤4.5 597 56.1 9 12
>4.5 419 39.3 13 15
Serousinvasion
Absent 257 24.1 8 12
Present 791 74.3 11 13
Sincronetumors
No 1034 97.1 11 13
Yes 30 2.8 11 16
Histologicaltype
Adenocarcinoma 898 84.3 10 13
Mucinousadenocarcinoma 121 11.4 13 15
Invasiveadenocarcinoma 36 3.4 9 10
Signetring&mucinouscells 10 0.9 12 31
Histologicalgrade
Differentiated 438 41.1 10 11
Undifferentiated 53 5.0 11 12
Depthofinvasion
Tis 13 1.2 7 19
T1 50 4.7 7 9
T2 148 13.9 9 12
T3 758 71.2 11 13
T4 63 5.9 11 16
Nodesretrieved
<12 583 54.7 -
-≥12 457 42.9 -
-Invadednodes
0 606 56.9 -
-01/mar 289 27.1 -
-≥4 145 13.6 -
-pN
pN0 596 56.0 10 13
pN1 293 27.5 10 11
pN2 149 14.0 13 15
pM
pM0 820 77.0 11 13
pM1 125 11.7 11 15
Resectionmargins
Withoutinvolvement 1007 94.6 11 13
Involved 36 3.4 11 15
VenousInvasion
Without 595 55.9 10 13
Table1–(Continued)
Variable n % Mediannumberof
nodesretrieved
Meannumberof nodesretrieved
LymphaticInvasion
Without 383 36.0 10 13
With 478 44.9 11 13
Stage
I 168 15.8 8 12
II 392 36.8 10 13
III 369 34.7 11 15
IV 126 11.8 11 15
Relapse
Absent 790 74.2 11 14
Present 151 14.2 11 11
Differentiated,wellandmoderatelydifferentiatedtumors;Undifferentiated,poorlydifferentiatedandundifferentiatedtumors;Tis, intra-mucous/insitucarcinoma;T1,submucousinvasion;T2,muscularispropriainvasion;T3,subserosous/notperitonizedpericolicconjunctivetissue invasion;T4,organsandstructuresinvasion.
Morenodeswerefoundinpatientsagedlessthan71.5years (median11 nodes).Regarding itslocation,thetumorswere moreofteninthecolon(68.4%,n=729),particularlyintheleft colon(45.6%,n=486).Themedianlymphnodesevaluatedwas greaterintherightcolon(Md=13),followedbytheleftcolon andrectum,bothwiththesamemedian(Md=10). In56.1% (n=597)ofcases,thetumorshowedadimension≤4.5cm,with
moreserosalinvasion(74.3%,n=791).Themajorityofpatients hadnosynchronoustumors(97.1%,n=1034).Themedianof nodeswasgreaterintumors>4.5cm(Md=13),andintumors withserosalinvasion(Md=11).Thepresenceofsynchronous tumorshadnoimpactinthemedianofnodesassessed(eleven nodesinbothcases).
Histologically,the tumorswere mainly adenocarcinoma (84.3%,n=898),andmucinousadenocarcinomawasthe sec-ondmostfrequenttumor(11.4%,n=121),followedbyinvasive adenocarcinomain3.4%ofcases(n=36).Tumorswithsignet ringcellsandmucinousareashad asmallfrequency(0.9%,
n=10).Themediannodesretrievedwasgreaterinmucinous adenocarcinoma (Md=13), followed by tumors with signet ringcellsandmucinousareas(Md=12)andadenocarcinoma (Md=10). Invasive adenocarcinoma had the lower median nodesevaluated(Md=9).
Relativelytotumorextension(T),themajorityoftumors areclassifiedasT3(71.2%,n=758),followedbyT2in13.9%of cases(n=148).T4lesionswerepresentonlyin5.9%ofcases (n=63),followedbytheT1(4.7%,n=50)andTisin1.2%ofcases (n=13).Thehigher mediannodes wasfound inT3and T4 tumors(Md=11).
Differentiatedtumorsweremorefrequent(41.1%,n=438) thanundifferentiated(5%,n=53).However,undifferentiated tumors had higher median nodes (Md=11). Regarding the numberoflymphnodesinsurgicalspecimen,54.7%(n=583) ofpatientshadlessthantwelvenodesretrieved,whereasin 42.9%(n=457),twelveormorelymphnodeswere assessed. Inthegreatmajority,56.9%ofcases(n=606),nometastatic lymphnodewasfound,andin27.1%(n=289)ofpatients1–3 metastaticlymphnodeswere found.Inonly13.6%(n=145)
cases,fourormorelymphnodeswereinvaded.In94.6%of cases(n=1007),therewasfreesurgicalmarginswithno neo-plastic lesion, and in 3.4%of cases(n=36) the tumor was interceptedbymarginsofexcision,andmediangangliafound inbothcaseswasthesame(Md=11).
Morepatientshadnovenousinvolvement(55.9%,n=595) butmosthadlymphaticinvasion(44.9%,n=478).Themedian ofnodesassessedwasgreaterinthepresenceofvenousand lymphaticinvolvement(Md=11).Mostpatients(56%,n=596) were classifiedasN0, followedbyN1in27.5%(n=293)and N2 in 13.9% of patients (n=148). In 77% of cases (n=820) therewasnodistantmetastases.pN2stagerecordedhigher mediannodesassessed(Md=13)andthepresenceorabsence ofdistantmetastases(PM0andpM1)hadnoinfluenceonthis result(Md=11).ThestagesIIandIIIwerethemostfrequently observedin36.8%(n=392)and34.7%(n=369)ofcases, respec-tively.ThestagesIIIandIVwerethosewhoreportedhigher mediannodesassessed(Md=11).
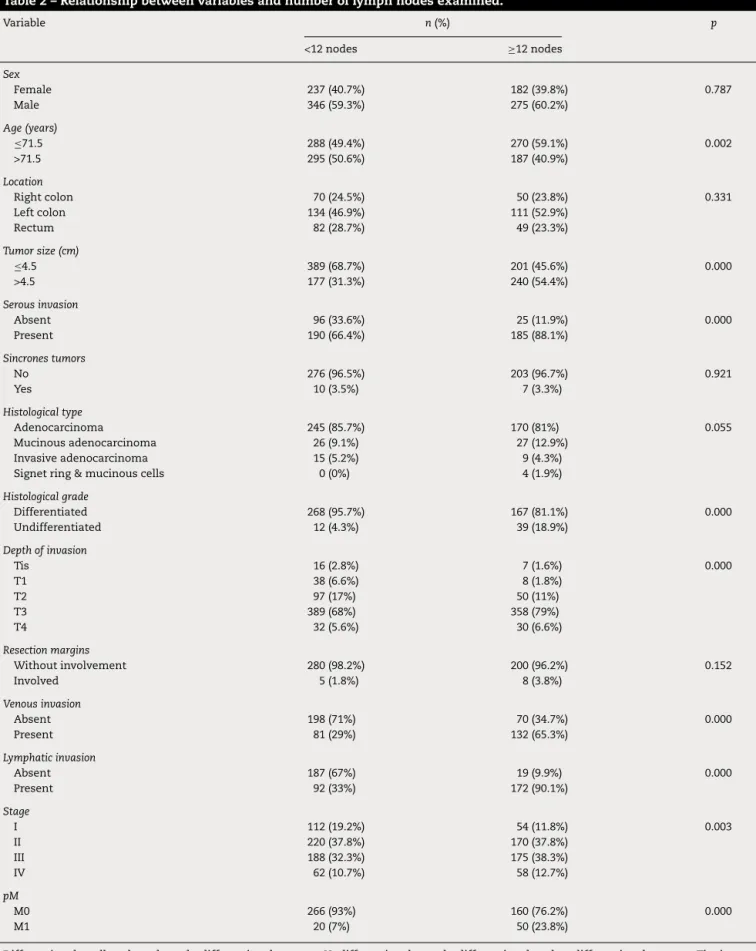
74.2% ofpatients (n=790)were freeofrelapses,and the medianlymphnodesevaluatedwas11,regardlessofthe exist-enceofrecurrences.Themajorityofpatients,59.6%(n=635), are alive, and the median nodes assessed was higher in this patients (Md=11). Relating the number ofnodes ana-lyzedwithseveralvariables(Table2),significantcorrelations werefoundwith:age(p=0.002),tumorsize(p=0.000),serosal invasion (p=0.000), differentiation (p=0.000), tumor pene-tration(p=0.000),venousandlymphaticinvasion(p=0.000), presenceofmetastasis(p=0.000)and TNMstage(p=0.003). Therewerenostatisticallysignificantcorrelationswith gen-der(p=0.787),tumorlocation(p=0.331);synchronoustumors (p=0.921),histologicaltype(p=0.055),andresectionmargins invasion(p=0.152).
Table2–Relationshipbetweenvariablesandnumberoflymphnodesexamined.
Variable n(%) p
<12nodes ≥12nodes
Sex
Female 237(40.7%) 182(39.8%) 0.787
Male 346(59.3%) 275(60.2%)
Age(years)
≤71.5 288(49.4%) 270(59.1%) 0.002
>71.5 295(50.6%) 187(40.9%)
Location
Rightcolon 70(24.5%) 50(23.8%) 0.331
Leftcolon 134(46.9%) 111(52.9%)
Rectum 82(28.7%) 49(23.3%)
Tumorsize(cm)
≤4.5 389(68.7%) 201(45.6%) 0.000
>4.5 177(31.3%) 240(54.4%)
Serousinvasion
Absent 96(33.6%) 25(11.9%) 0.000
Present 190(66.4%) 185(88.1%)
Sincronestumors
No 276(96.5%) 203(96.7%) 0.921
Yes 10(3.5%) 7(3.3%)
Histologicaltype
Adenocarcinoma 245(85.7%) 170(81%) 0.055
Mucinousadenocarcinoma 26(9.1%) 27(12.9%)
Invasiveadenocarcinoma 15(5.2%) 9(4.3%)
Signetring&mucinouscells 0(0%) 4(1.9%)
Histologicalgrade
Differentiated 268(95.7%) 167(81.1%) 0.000
Undifferentiated 12(4.3%) 39(18.9%)
Depthofinvasion
Tis 16(2.8%) 7(1.6%) 0.000
T1 38(6.6%) 8(1.8%)
T2 97(17%) 50(11%)
T3 389(68%) 358(79%)
T4 32(5.6%) 30(6.6%)
Resectionmargins
Withoutinvolvement 280(98.2%) 200(96.2%) 0.152
Involved 5(1.8%) 8(3.8%)
Venousinvasion
Absent 198(71%) 70(34.7%) 0.000
Present 81(29%) 132(65.3%)
Lymphaticinvasion
Absent 187(67%) 19(9.9%) 0.000
Present 92(33%) 172(90.1%)
Stage
I 112(19.2%) 54(11.8%) 0.003
II 220(37.8%) 170(37.8%)
III 188(32.3%) 175(38.3%)
IV 62(10.7%) 58(12.7%)
pM
M0 266(93%) 160(76.2%) 0.000
M1 20(7%) 50(23.8%)
1.0
0.8
0.6
0.4
0.2
0.0
0 50
Cum
ulativ
e sur
viv
al
Duration (months)
<12
≥12
<12-censored
≥12-censored
100 150 200
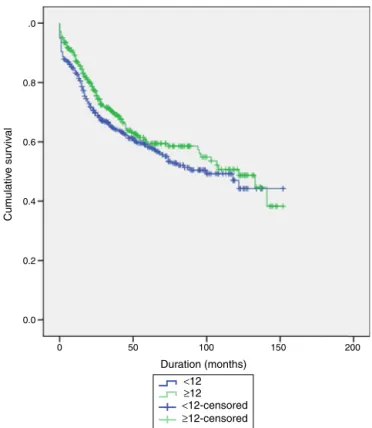
Fig.1–Survivalcurveinfunctionofthenumberoflymph nodeevaluatedinCRCpatientssubmittedtosurgical treatment,assessedbylog-ranktest(p=0.642).
.0
0.8
0.6
0.4
0.2
0.0
0 50 100 150 200
<12
≥12
<12-censored
≥12-censored
Cum
ulativ
e sur
viv
al
Duration (months)
Fig.2–Survivalcurveinfunctionofthenumberoflymph nodeevaluatedinColonCancerpatientssubmittedto surgicaltreatment,assessedbylog-ranktest(p=0.171).
10
8
6
4
2
0
0 50 100 150 200
<12
≥12
<12-censored
≥12-censored
Cum
ulativ
e sur
viv
al
Duration (months)
Fig.3–Survivalcurveinfunctionofthenumberoflymph nodeevaluatedinRectalCancerpatientssubmittedto surgicaltreatment,assessedbylog-ranktest(p=0.204).
Discussion/Conclusion
PathologicalstagingisamajorprognosticfactorforCRCand theregionallymphnodemetastasesareoneofthestrongest predictorsofoutcomeaftersurgicalresection.Currently, sev-eralguidelinessuggestaminimumscoreof12lymphnodes assessedinthesurgicalspecimenasaprognosticfactorof CRC.11,34–36
Theresultsofpatient’sepidemiologicalcharacterization,in thisstudy,coincidewiththosementionedbyseveralauthors, highlightingthisregionasanareaofhighincidenceofCRC. Inthisstudy,thedistributionofCRCbysexandageiswell proven,affectingmorementhanwomenandnotingahigher incidenceinindividualsagedlessthan71.5years.Inthis pop-ulation,colontumors,leftcoloninparticular,werethemost prevalent,andadenocarcinomawasthemostcommon his-tologicaltype,asdocumentedintheliterature.37–39 Dataof
countrieswithhighincidenceofCRCshowthatabout20%of patients arediagnosedinstageIVand 25%instageI,4,40,41
whichcoincideswiththeresultsobtained.
Weobservedasignificantcorrelationbetweenthenumber ofnodesevaluatedandthevariables:age,tumorsize,serosal invasion,differentiation,penetration,venousandlymphatic invasion,presenceofmetastasesandTNMstage.Thisnumber islowerinolderpatients,andapossibleexplanationmaybe thatthenumberoflymphnodestendstodecreasewithage.42
thisisduetosurgicaltechnique.Ontheotherhand,these fac-torsrelatetopoorprognosisandcanthusbeassociatedwith increasednodesdimensionandconsequentlybetter visual-izationandcollectionbythepathologistsandalsoagreater diligenceinidentificationofassociatednodes.
This study also demonstrate that factors such as age, location,tumorsize,histologictype,venousand lymphatic invasion,andtumorpenetrationinfluencethemediannodes assessed. This number is higher in tumors≥ 4.5cm, right
colontumors,patientsaged≤72.5years,tumorswithvenous
andlymphaticinvasion,inmucinousadenocarcinomaandin tumorswithinvasionofsubserousorotherorgans/structures (higherpT),whichgoesagainsttheliterature.15However,sex,
resectionmargins involvement,presenceofdistant metas-tasesandrelapsesdidnothaveanyinfluenceonthemedian nodesassessed,unlikereportedinvariousstudies.
Theresultsdemonstratethatinthecaseofcolontumors, assessmentoftwelveormorenodesresultsinagreater sur-vival.Inrectalcancer,it wasfoundthatsurvivaldecreases afterapproximately twenty-fivemonthsofdiagnosis, com-pared to patients with less than twelve lymph nodes evaluated.However,theseresultsarenotstatistically signif-icant(p>0.05),anditisnotpossibletoadmittheexistence ofacorrelationbetweensurvivalandthenumber ofnodes assessed be larger or smaller/equal to twelve. The results obtained inthis study contradict various studies and cur-rentrecommendations.Thisisacontroversialtopic,andthe optimalnumberofnodestoevaluate,inordertoobtain sig-nificantresultsinpatientssurvival,isstillhighlydebatedand questionable.Onepossibleexplanationfortheresultsofthis studylies inthe factthatiscommonpracticeofthe onco-logistsinthis hospitallabelpatientswithless than twelve nodes,identifiedinsurgicalrecession,as“N-positive”;thus, thesepatientsaresubjectedtoadjuvanttherapyiftheir gen-eralconditionpermits.Thismeansthattheyareovertreated patientswhomightactuallybeN0,butaretreatedashaving nodalmetastasessincelessthantwelvenodeswereretrieved. Itis not possible to rule out other factors that also influ-encesurvival,includingcomorbidities,performedtreatments andpost-surgical mortality.Surgicaland pathological tech-niquesshouldalsobetakenintoconsiderationinobtaining lymphnodes.15,16 Amore carefulresectionof mesorectum
andamoreaccuratenodespathologicalevaluationcontribute toimprovedstagingandthereforemoreaccurateevaluation and patient follow up. Thus, subject patients foradjuvant treatment toxicity, forwhich this is unnecessary,could be avoided,reducingconsequenthospitalcosts,botheconomic andhumans.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. JemalA,MurrayT,WardE,SamuelsA,TiwariRC,GhafoorA, etal.Cancerstatistics.CACancerJClin.2005;55:10–30.
2.Roreno.RegistoOncológicoRegionaldoNorte;2007.
http://www.roreno.com.pt[accessed13.06.12].
3.BosettiC,LeviF,RosatoV,BertuccioP,LucchiniF,NegriE, etal.RecenttrendsincolorectalcancermortalityinEurope. IntJCancer.2011;129:180–91.
4.AlexanderDD,WaterborJ,HughesT,FunkhouserE,GrizzleW, ManneU.African-AmericanandCaucasiandisparitiesin colorectalcancermortalityandsurvivalbydatasource:an epidemiologicreview.CancerBiomark.2007;3:301–13.
5.MendesV.PreveniroCancrodoCóloneRecto.JPort Gastrenterol.2008;15:153–5.
6.KanemitsuY,KomoriK,IshiguroD,WatanabeT,SugiharaK, etal.Therelationshipoflymphnodeevaluationand colorectalcancersurvivalaftercurativeresection:a multi-institutionalstudy.AnnSurgOncol.2012;125:34–40.
7.ComptonCC,FieldingLP,BurgartLJ,ConleyB,CooperHS, HamiltonSR,etal.Prognosticfactorsincolorectalcancer. CollegeofAmericanPathologistsConsensusStatement1999. ArchPatholLabMed.2000;124:979–94.
8.TsaiHL,LuCY,HsiehJS,WuDC,JanCM,ChaiCY,etal.The prognosticsignificanceoftotallymphnodeharvestinpatient withT2-4N0M0colorectalcancer.JGastrointestSurg. 2007;11(5):660–5.
9.NationalComprehensiveCancerNetwork.http://wwwnccn. org/professionals/qualitymeasures/PDF/
colonqualitymeasures.pdf[accessed13.06.12]. 10.AmericanCollegeofSurgeons.
http://www.facs.org/cancer/qualitymeasures.html[accessed 13.06.12].
11.AJCCcancerstagingmanual.7thed;2010.
www.cancerstaging.org/staging/index.html[accessed 13.06.12].
12.GoldsteinNS.Lymphnoderecoveriesfrom2427pT3 colorectalresectionspecimensspanning45years: recommendationsforaminimumnumberofrecovered lymphnodesbasedonpredictiveprobabilities.AnJSurg Pathol.2002;26:179–89.
13.BilimoriaKY,BentremDJ,StewartAK,TalamontiMS, WinchesterDP,RussellTR,etal.Lymphnodeevaluationasa coloncancerqualitymeasure:anationalhospitalreportcard. JNatlCancerInst.2008;100:1310–7.
14.ComptonCC,FieldingLP,BurgartLJ,ConleyB,CooperHS, HamiltonSR,etal.Prognosticfactorsincolorectalcancer. CollegeofAmericanPathologistsConsensusStatement1999. 2000;980:192–249.
15.ChapuisPH,DentOF,FisherR,NewlandRC,PheilsMT,Smyth E,etal.Amultivariateanalysisofclinicalandpathological variablesinprognosisafterresectionoflargebowelcancer.Br JSurg.1985;72:698–702.
16.ScabiniS,FerrandoV.Numberoflymphnodesafter neoadjuvanttherapyforrectalcancer:howmanyare needed?WorldJGastrointestSurg.2012;27:32–5.
17.SauerR,BeckerH,HohenbergerW,RodelC,WittekindC, FietkauR,etal.Preoperativeversuspostoperative chemoradiotherapyforrectalcancer.NEnglJMed. 2004;351:1731–40.
18.HyamsDM,MamounasEP,PetrelliN,RocketteH,JonesJ, WieandHS,etal.Aclinicaltrialtoevaluatetheworthof preoperativemultimodalitytherapyinpatientswithoperable carcinomaoftherectum:aprogressreportofNational SurgicalBreastandBowelProjectProtocolR-03.DisColon Rectum.1997;40:131–9.
19.GlimeliusB,OliveiraJ.Rectalcancer:ESMOclinical recommendationsfordiagnosis,treatmentandfollow-up. AnnOncol.2008;19:31–2.
21.BujkoK,NowackiMP,Nasierowska-GuttmejerA,MichalskiW, BebenekM,KryjM.Long-termresultsofarandomizedtrial comparingpreoperativeshort-courseradiotherapywith preoperativeconventionallyfractionatedchemoradiationfor rectalcancer.BrJSurg.2006;93:1215–23.
22.KapiteijnE,MarijnenCA,NagtegaalID,PutterH,SteupWH, WiggersT,etal.Preoperativeradiotherapycombinedwith totalmesorectalexcisionforresectablerectalcancer.NEnglJ Med.2001;345:638–46.
23.SchofieldJB,MounterNA,MallettR,HaboubiNY.The importanceofaccuratepathologicalassessmentoflymph nodeinvolvementincolorectalcancer.ColorectalDis. 2006;8:460–70.
24.NorwoodMG,SuttonAJ,WestK,SharpeDP,HemingwayD, KellyMJ.Lymphnoderetrievalincolorectalcancerresection specimens:nationalstandardsareachievable,andlow numbersareassociatedwithreducedsurvival.ColorectalDis. 2010;12:304–9.
25.WichmannMW,MullerC,MeyerG,StraussT,HornungHM, Lau-WernerU,etal.Effectofpreoperative
radiochemotherapyonlymphnoderetrievalafterresectionof rectalcancer.ArchSurg.2002;137:206–10.
26.EvansMD,BartonK,ReesA,StamatakisJD,KarandikarSS. Theimpactofsurgeonandpathologistonlymphnode retrievalincolorectalcanceranditsimpactonsurvivalfor patientswithDukes’stageBdisease.ColorectalDis. 2008;10:157–64.
27.SobinLH.TNMclassification:clarificationofnumberof regionallymphnodesforpN0.BrJCancer.2001;85:780.
28.RinkusKM,RussellGB,LevineEA.Prognosticsignificanceof nodaldiseasefollowingpreoperativeradiationforrectal adenocarcinoma.AmSurg.2002;68:482–7.
29.MarijnenCA,NagtegaalID,KleinKranenbargE,HermansJ, vandeVeldeCJ,LeerJW,etal.Nodownstagingafter short-termpreoperativeradiotherapyinrectalcancer patients.JClinOncol.2001;19:1976–84.
30.KohDM,ChauI,TaitD,WotherspoonA,CunninghamD, BrownG.Evaluatingmesorectallymphnodesinrectalcancer beforeandafterneoadjuvantchemoradiationusing
thin-sectionT2-weightedmagneticresonanceimaging.IntJ RadiatOncolBiolPhys.2008;71:456–61.
31.PerezRO,PereiraDD,ProscurshimI,Gama-RodriguesJ,Rawet V,SãoJuliãoGP,etal.Lymphnodesizeinrectalcancer
followingneoadjuvantchemoradiation–canwerelyon radiologicnodalstagingafterchemoradiation?DisColon Rectum.2009;52:1278–84.
32.MurphyJ,PocardM,JassJR,O’SullivanGC,LeeG,TalbotIC. NumberandsizeoflymphnodesrecoveredfromdukesB rectalcancers:correlationwithprognosisandhistologic antitumorimmuneresponse.DisColonRectum. 2007;50:1526–34.
33.KimYW,KimNK,MinBS,LeeKY,SohnSK,ChoCH,etal.The prognosticimpactofthenumberoflymphnodesretrieved afterneoadjuvantchemoradiotherapywithmesorectal excisionforrectalcancer.JSurgOncol.2009;100:1–7.
34.JosephNE,SigurdsonER,HanlonAL,WangH,MayerRJ, MacDonaldJS,etal.Accuracyofdeterminingnodalnegativity incolorectalcanceronthebasisofthenumberofnodes retrievedonresection.AnnSurgOncol.2003;10:213–8.
35.ScottKW,GraceRH.Detectionoflymphnodemetastasesin colorectalcarcinomabeforeandafterfatclearance.BrJSurg. 1989;76:1165–7.
36.CaplinS,CerottiniJP,BosmanFT,ConstandaMT,GivelJC.For patientswithDukes’B(TNMstageII)colorectalcarcinoma, examinationofsixorfewerlymphnodesisrelatedtopoor prognosis.Cancer.1998;83:666–72.
37.SvagzdysS,LesauskaiteV,PavalkisD,NedzelskieneI,PranysD, TamelisA.Microvesseldensityasnewprognosticmarker afterradiotherapyinrectalcancer.BMCCancer.2009;9:95.
38.BrennerH,HoffmeisterM,HaugU.Shouldcolorectalcancer screeningstartatthesameageinEuropeancountries? Contributionsfromdescriptiveepidemiology.BrJCancer. 2008;99:532–5.
39.ZavoralM,SuchanekS,ZavadaF,DusekL,MuzikJ,SeifertB, etal.ColorectalcancerscreeninginEurope.WorldJ Gastroenterol.2009;15:5907–15.
40.ZafarSY,AbernethyAP,AbbottDH,GrambowSC,MarcelloJE, HerndonJE2nd,etal.Comorbidity,age,raceandstageat diagnosisincolorectalcancer:aretrospective,parallel analysisoftwohealthsystems.BMCCancer.2008;8:345.
41.BensonIIIAB.Epidemiology,diseaseprogressionand economicburdenofcolorectalcancer.JManagCarePharm. 2007;13:5–18.