BrazJOtorhinolaryngol.2014;80(6):476---479
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
ORIGINAL
ARTICLE
Classification
of
rhinoplasties
performed
in
an
otorhinolaryngology
referral
center
in
Brazil
夽,夽夽
Flávio
Barbosa
Nunes
∗,
Paulo
Fernando
Tormin
Borges
Crosara,
Isamara
Simas
de
Oliveira,
Leandro
Farias
Evangelista,
Danilo
Santana
Rodrigues,
Helena
Maria
Gonc
¸alves
Becker,
Roberto
Eustáquio
Santos
Guimarães
DepartmentofOtorhinolaryngologyandOphthalmology,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
Received30June2013;accepted24May2014 Availableonline23August2014
KEYWORDS
Plasticsurgery; Esthetics; Rhinoplasty; Education
Abstract
Introduction:Facialplasticandreconstructivesurgeryinvolvestheuseofsurgicalprocedures toachieveestheticandfunctionalimprovement.Itcanbeusedfortraumatic,congenital,or developmentalinjuries.Medicine,withanemphasisonfacialplasticsurgery,hasmadeprogress inseveral areas,includingrhinoplasty, providing good long-termresults andhigher patient satisfaction.
Objective:Toevaluatecasesofrhinoplastyanditssubtypesinareferralcenter,andto under-standtherelevanceofteachingrhinoplastytechniquesinaserviceofotolaryngologyresidency.
Methods:Aretrospectivestudythatassessed325rhinoplastiesperformedbythird-yearmedical residentsunderthe supervision ofchief residentsinchargeofthe ServiceofFacialPlastic SurgeryinthishospitalwasconductedfromJanuaryof2003toAugustof2012.TheService Protocolincludedthefollowingsubtypes:functional, esthetic,post-traumatic,revision,and reconstructiverhinoseptoplasty.
Results:Oftherhinoplastiesperformed184(56.21%)werefunctional,59(18.15%)were post-traumatic, 27were (8.30%)esthetic,15were (4.61%)reconstructive,and40(12.30%) were revisionprocedures.
夽 Pleasecitethisarticleas:NunesFB,CrosaraPF,OliveiraIS,EvangelistaLF,RodriguesDS,BeckerHM,etal.Classificationofrhinoplasties performedinanotorhinolaryngologyreferralcenterinBrazil.BrazJOtorhinolaryngol.2014;80:476---9.
夽夽
Institution:DepartmentofOtorhinolaryngology,HospitaldasClínicas(HC),UniversidadeFederaldeMinasGerais(UFMG),Belo Hori-zonte,MG,Brazil.
∗Correspondingauthor.
E-mail:[email protected](F.B.Nunes).
http://dx.doi.org/10.1016/j.bjorl.2014.08.002
Classificationofrhinoplastiesperformedinanotorhinolaryngologyreferralcenter 477
Conclusion: Functionalrhinoseptoplastieswerethemostprevalenttype,whichhighlightsthe relevanceofteachingsurgicaltechniques, notonlyforseptoplasty,butalsotheinclusionof rhinoplastytechniquesinteachingcenters.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Cirurgiaplástica; Estética; Rinoplastia; Capacitac¸ão
Classificac¸ãodasrinoplastiasrealizadasemumcentrodereferênciaem otorrinolaringologianoBrasil
Resumo
Introduc¸ão: Acirurgiaestéticaereconstrutoratêmporobjetivoautilizac¸ãodeprocedimentos cirúrgicosparaalcanc¸armelhoraestéticaefuncional.Podeserutilizadaparalesões traumáti-cas, congênitasou de desenvolvimento.A Medicina,com ênfase naplástica facial, obteve avanc¸osnasmaisdiversasáreas,inclusivenarinoplastia,permitindobonsresultadosalongo prazoemaiorsatisfac¸ãodospacientes.
Objetivo: Avaliar acasuística do setor de rinoplastia e suas subdivisões em um centro de referência.Compreender arelevânciado ensino dastécnicas derinoplastia em um servic¸o deresidênciamédicadeotorrinolaringologia.
Método: Estudoretrospectivoondeforamanalisados325rinoplastias,realizadaspormédicos residentesdoterceiroanocomsupervisãodospreceptoresresponsáveispeloservic¸odeCirurgia PlásticadaFacedessehospital,noperíododejaneirode2003aagostode2012.Oprotocolo doservic¸ofoipreenchidocomenfoquenasseguintessubdivisões:rinosseptoplastiafuncional, estética,pós-traumática,revisionalereconstrutora.
Resultados: Das rinoplastias realizadas, 184 (56,21%) foram funcionais, 59 (18,15%) pós-traumáticas,27(8,30%)estéticas,15(4,61%)reconstrutorase40(12,30%)revisionais.
Conclusão:As rinosseptoplastias funcionais foram as mais prevalentes, o que mostra a importânciadoensino,nãosomentedastécnicasdeseptoplastias,mastambém,dainclusão doaprendizadodetécnicasderinoplastiasemcentrosdeensino.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Cosmetic surgeries are on the rise, and among them, rhinoplasty is one of the most commonly performed. Through the use of a good technical basis in basic rhi-noseptoplastysurgery,itispossibletotreatapproximately 95% of primary patients seen in a private practice of esthetic surgery, demonstrating the increasing need for inclusionofmorerefinedtechniquesofrhinoplastyinroutine otorhinolaryngology.1
In the late19th century, rhinoplastywasnearly exclu-sivelyreconstructivesurgeryforlargenasalmutilations.2In
theearly20thcentury, itwasrapidlydisseminated world-wideasan estheticprocedure,but inthe 21stcentury,it hasbecome moreconservative, withmodelingtechniques ratherthancartilageresectionandwithasignificant reduc-tioninaggressiveosteotomies.3,4
The number of rhinoplasties and their subtypes (functional, esthetic, reconstructive, revision, and post-traumatic surgeries) has significantly increased since the mid-20th century.3,5 However,thenose representsa
com-plexanatomicalregion,inwhichsmallfunctionalalterations can cause great harm to the patient.6 Thus, the study
of rhinoplasty techniques associated with thoseof septo-plasty has gained prominence in referral otolaryngology services,whichareregardedasprofessionalgeneration cen-ters,withthegreatestresponsibilityforthetrainingofthese professionals.2,4
Thepresentstudyaimedtoevaluateaseriesofpatients who underwent rhinoplasty in a referral center, focusing ontheesthetic,functional,post-traumatic,reconstructive, and revision subtypes. Reconstructive surgeries are those performedtocorrectdefectsduetolossofsubstance(e.g., aftertumorresection);revisionproceduresaresurgical re-interventions, either performed by the same surgeon or anotherone;post-traumaticsurgeriesarethoseperformed due toinjuries resulting from external causes; functional proceduresconsist of any approachaiming at respiratory functioncorrection;andestheticproceduresarepurely cos-meticsurgeries.
Methods
478 NunesFBetal.
Table1 Generalaspectsofthestudy.
Numberofpatients 325 Agerangeofpatients 12---71years
Females 185(56.92%)
Males 140(43.07%)
serviceprotocols,fromJanuary2003toAugust2012.7The
inclusion criteria were all patients submitted to rhino-plastyduringthatperiod,withrecordscontainingallclinical andsurgicalinformation,whiletheexclusioncriteriawere patients whose records were incomplete. There were no clinicalconditionsofexclusion.
Patients underwent general clinical and otorhinolaryn-gologicalassessment, preoperative evaluation,in addition to photo sessions and surgical procedure scheduling by profilometry. The following parameters were evaluated: facialthirds,facialfifths,nasofrontalandnasolabialangles, columella-lobule angle, natural horizontal facial plane, nasallength,andtipprojection.8
Third-yearresidentsperformedtherhinoplastysurgeries, under the supervision of the chief residents in charge of the Service of Facial Plastic Surgery of the Otolaryngol-ogyDepartmentofthis hospital.Whenevernecessary,the chiefresidentsintervenedinthesurgery,correctingfaults, developingthetechnique,andfinalizingthesurgerywithin asafetimeperiodforthepatient.Allprocedureswere per-formedunderlocalorgeneralanesthesia,andmostoften, thepatientwasdischargedwithin24h.
Postoperatively, patients underwent ambulatory moni-toring,returningfor consultationsseven, 15,and 30 days afterthesurgery,withfollow-upvisitsatthreemonths,six months,andannuallythereafter.On theseoccasions,new photographsweretakenandsurgicalresultswereanalyzed. The protocol, modified from the literature to adapt to this service,9 was completed for the following
sub-typesofrhinoplasty:functionalrhinoseptoplasty,cosmetic, reconstructive,revision,andpost-traumaticrhinoplasty.All patients signed an informed consent. Data regarding the typeofsurgeryperformedwerecarefullyverifiedfromthe patients’surgicalrecordsandprocessedinMicrosoftExcel®.
The study was approved by the Ethics Committee on Human Research of the Hospital, under number 0138.0.203.000-11.
Results
Afterapplyingtheinclusionandexclusioncriteria,atotalof 325patientswereidentified.Of these,185(56.92%)were femalesand 140(43.07%) weremales.The meanage was 30.9±7.5years(Table1).
Of the 325 selected rhinoplasties, 184 (56.61%) were functional,59(18.15%)post-traumatic,27(8.30%)esthetic, 15 (4.61%) reconstructive, and 40 (12.30%) were revision surgeries(Fig.1).
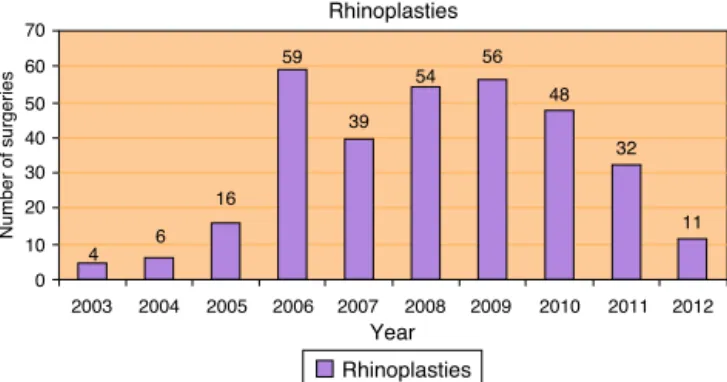
The meannumberof surgeriesperformedperyear was 32.5,withaminimumoffoursurgeriesin2003anda maxi-mumof59surgeriesin2006(Fig.2).
200 180 160 140 120 100 80 60 40 20 0 27 184 59 15 40 Categories Rhinoplasties
Number of surgeries
Esthetical
Reconstructive Revisional Functional Traumatic
Figure 1 Functional, esthetic, post-traumatic, reconstruc-tive, andrevision rhinoseptoplastiesperformedfromJanuary of2003toAugustof2012.
Rhinoplasties
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Year 4 6 16 59 39 54 56 48 32 11 70 60 50 40 30 20 10 0
Number of surgeries
Rhinoplasties
Figure2 Rhinoplastiesperformedperyear,fromJanuaryof 2003toAugustof2012.
Discussion
Thepopularityoffacialplasticsurgerieshasgrownfromthe mid-20thcenturyandshowsastrongtendencytowardhigher growth,mainlyinfluencedby theexpansionofthe beauty andbodymetamorphosisindustries.Braziliscurrentlythe secondlargestmarketinnumberoffacialplasticsurgeries, secondonlytotheUnitedStates.2,10
Of all the facial cosmetic procedures, face-lifts, facial liposuction, blepharoplasty, and rhinoplasty are predominant. Rhinoplasty, however, is the most fre-quently performed facial esthetic surgery in the United States, mainly due to itsstrong esthetical and functional characteristics.9,10
Reparative rhinoplasty for the reconstruction of large nasal mutilations has become more conservative, with greater use of modeling maneuvers and with less carti-lage resectionand asignificant reduction of theneed for aggressiveosteotomies.Moreover,itsassociationwithmore refined techniques of septoplasty has resulted in greatly improved functional outcomes.4,11 However, even today,
these procedures require extensive technical and scien-tificknowledge,placinggreatresponsibilityonthereferral centersthathave theobligationtoprovidetheeducation, training,andexperienceinthisarea.9
Classificationofrhinoplastiesperformedinanotorhinolaryngologyreferralcenter 479
the increasing need for improved rhinoseptoplasty tech-niques, rather than exclusively septoplasty techniques. Tannaetal.2 reportedmedicalresidency asthemain
fac-torinthelearningcurveinthistypeofprocedure,andcited anaverageof15surgeries/year/residentinmajorreferral centersintheUnitedStates.Thisisinlinewithourstudy, whichshowsanaverageof32.5surgeries/yearfortwo third-year medicalresidents, providinga majorcontribution to professionaltraininginfacialplasticsurgery.
Conclusion
Rhinoplasty requires surgical skills and experience to achieve good results. The authors believe that residents should perform such surgeries, and training centers can provideasufficientnumberandfrequencyofcases.Thereis aclearprevalenceofrespiratorysymptomsinpatients seek-ing otorhinolaryngological evaluation for this procedure. Therefore,giventhehighoverall prevalenceof functional rhinoseptoplasties,theimportanceofteachingrhinoplasty techniques, associated with septoplasty and other tech-niquesaimedatimprovementofnasalairflow,isnoteworthy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.DanielRK.Theroleofdicedcartilagegraftsinrhinoplasty. Aes-thetSurgJ.2006;26:209---13.
2.TannaN,LesavoyMA,KawamotoHK,BoydJB,FedortsovaN, Andrews BT,et al. Experientiallearning inaesthetic surgery training:aquantitativecomparisonamongsurgical subspecial-ties.PlastReconstrSurg.2012;129:528e---34e.
3.Rosdeutscher JD. The history of otolaryngology in plastic surgery.PlastReconstrSurg.2003;111:2377---85.
4.Maniglia AJ, Maniglia JV, Maniglia CP. História e evoluc¸ão da rinosseptoplastia reconstrutora, funcional e estética. In: Maniglia AJ, Maniglia JJ, Maniglia JV, editors. Rinoplastia: estética, funcional, reconstrutora. Rio de Janeiro: Revinter; 2002.p.1---6.
5.Faidiga GB, Carenzi LR, Yassuda CC, Tassiana do Lago FS, LeiteMGJ,Anselmo-LimaWT.Long-termevaluationinaesthetic rhinoplasty in anacademic referralcenter. Braz J Otorhino-laryngol.2010;76:437---41.
6.Asaria J, Pepper JP, Baker SR. Key issues in nasal recon-struction. Curr Opin Otolaryngol Head Neck Surg. 2010;18: 278---82.
7.Freitas VA, Becker CG, Guimarães RE, Crosara PF, Morais GA, Moura M. Surgical treatment of otosclerosis in medi-cal residency training. Braz J Otorhinolaryngol. 2006;72: 727---30.
8.GunterJP, HackneyFL.Avaliac¸ãoclínicaeanálise facial.In: GunterJP,RohrichRJ,AdamsJrWP,editors.Dallasrinoplastia -cirurgiadonarizpelosmestres.RiodeJaneiro:Revinter;2006. p.31---42.
9.MeningaudJP,LantieriL,BertrandJC.Rhinoplasty:anoutcome research.PlastReconstrSurg.2008;121:251---7.
10.Liu TS, Miller TA. Economic analysis of the future growth of cosmetic surgery procedures. Plast Reconstr Surg. 2008;121:404e---12e.