w w w . r b o . o r g . b r
Original
Article
Evaluation
of
functional
results
from
shoulders
after
arthroscopic
repair
of
complete
rotator
cuff
tears
associated
with
traumatic
anterior
dislocation
Glaydson
Gomes
Godinho
a,b,c,∗,
José
Márcio
Alves
Freitas
a,b,c,
Flávio
de
Oliveira
Franc¸a
a,b,c,
Flávio
Márcio
Lago
Santos
a,b,c,
Leandro
Furtado
de
Simoni
a,b,c,
Pedro
Couto
Godinho
a,b,caHospitalOrtopédico,BeloHorizonte,MG,Brazil
bHospitalLifecenter,BeloHorizonte,MG,Brazil
cHospitalBeloHorizonte,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6March2015 Accepted28May2015
Availableonline4February2016
Keywords:
Shoulder Arthroscopy Rupture Rotatorcuff Shoulderdislocation
a
b
s
t
r
a
c
t
Objective:Toevaluatetheclinicaloutcomeofarthroscopicrotatorcufffixationand,when
present,simultaneousrepairoftheBankartlesioncausedbytraumaticdislocation;andto assesswhetherthesizeoftherotatorcuffinjurycausedbytraumaticdislocationhasany influenceonthepostoperativeclinicaloutcomes.
Methods:Thirty-threepatientswithtraumaticshoulderdislocationandcompleterotator
cuffinjury,withatleasttwoyearsoffollowup,wereretrospectivelyevaluated.Foranalysis purposes,thepatientsweredividedintogroups:presenceoffixedBankartlesionorabsence ofthislesion,androtatorcufflesionssmallerthan3.0cm(groupA)orgreaterthanorequal to3.0cm(groupB).Allthepatientsunderwentarthroscopicrepairofthelesionsandwere evaluatedpostoperativelybymeansoftheUCLA(UniversityofCaliforniaatLosAngeles) scoreandstrengthmeasurements.
Results:ThegroupwithBankartlesionrepairhadapostoperativeUCLAscoreof33.96,while
the scoreofthegroupwithoutBankart lesionwas33.7,withoutstatisticalsignificance (p=0.743).GroupAhadapostoperativeUCLAscoreof34.35andgroupB,33.15,without statisticalsignificance(p=0.416).
Conclusion: Thefunctionaloutcomesofthepatientswhoonlypresentedcompleterotator
cufftearingaftertraumaticshoulderdislocation,whichunderwentarthroscopicrepair,were similartotheoutcomesofthosewhopresentedanassociatedwithaBankartlesionthat wascorrectedsimultaneouslywiththerotatorcuffinjury.Theextentoftheoriginalrotator cuffinjurydidnotalterthefunctionalresultsinthepostoperativeevaluation.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:glaydsongg@gmail.com(G.G.Godinho). http://dx.doi.org/10.1016/j.rboe.2016.01.007
Avaliac¸ão
dos
resultados
funcionais
dos
ombros
submetidos
ao
reparo
artroscópico
de
roturas
completas
do
manguito
rotador
associadas
a
luxac¸ões
traumáticas
anteriores
Palavras-chave:
Ombro Artroscopia Ruptura
Manguitorotador Luxac¸ãodoombro
r
e
s
u
m
o
Objetivo: Avaliarodesfecho clínico da fixac¸ão artroscópica domanguito rotador(MR)
e, quandopresente, a correc¸ãosimultânea da lesãode Bankart, causadaspor luxac¸ão traumática.AvaliarseadimensãodalesãodoMRcausadaporluxac¸ãotraumática influen-ciounosresultadosclínicospós-operatórios.
Métodos: Foramavaliadosretrospectivamente33 pacientescomluxac¸ãotraumáticado
ombroelesãocompletadomanguitorotadoreseguimentomínimodedoisanos.Parafins deanálise,ospacientesforamdivididosemgrupos:presenc¸adelesãodeBankartfixadaou ausênciadalesãoelesõesdoMRmenoresdoque3cm(grupoA)ouiguaisaoumaiores doque3cm(grupoB).Todosforamsubmetidosareparoartroscópicodaslesõese avalia-dos,pós-operatoriamente,peloescoredaUCLA(UniversityofCaliforniaatLosAngeles)e medidadaforc¸a.
Resultados: OgrupoemquehouveoreparodalesãodeBankartapresentouUCLA
pós-operatóriode33,96,emrelac¸ãoaogrupoemqueessalesãonãoestavapresente33,7,sem significânciaestatística(p=0,743).OgrupoAapresentouresultadodeUCLApós-operatório de34,35egrupoB33,15,semsignificânciaestatística(p=0,416).
Conclusão: Osresultadosfuncionaisdospacientesqueapresentaramapenasrotura
com-pleta do manguito rotador após luxac¸ão traumática do ombro, submetidos ao reparo artroscópico,mostrou-sesemelhanteàquelesqueapresentaramassociac¸ãodalesão de Bankart, corrigida simultaneamente com a lesão domanguito rotador. A extensão da lesãoinicialdomanguitorotadornãoalterouosresultadosfuncionaisnaavaliac¸ão pós-operatória.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Theshoulderisthejointwithgreatestmobilityandinstability inthehumanbody,andforthisreasonitistheonemostliable todislocate.1
Glenohumeraldislocationmaycausetearingoftherotator cuff.Thisisrelativelyrareamongpatientsundertheageof 40yearsbutmorefrequentamongpatientsoverthisage.2–4 Rotatorcuffinjuriesarethemaincomplicationdocumented aftershoulderdislocationamongpatientsovertheageof40 years.5Thisisduetothedifferentinjurypatternspresented bythestaticanddynamicstabilizersinthesegroups.
Capsuloligamentousanteriorstaticstabilizers,whichwere describedbyMcLaughlinetal.,6haveafundamentalrolein youngindividuals’shoulders,butnotinpatientsovertheage of40years.Whentheyareinjured,thisisexpressedinthe formofBankartlesions.7Afterthisage,thefunctionofthe rotatorcuffasadynamicstabilizerhasfundamental impor-tanceand,wheninjured,thisgenerateswhatDebiskietal.8 andCraigetal.9describedasposteriorinstability,with con-sequentlyincreasedanterior translation due toloss ofthe posterosuperiorblockagethattherotatorcuffprovides.
Combined repair of Bankart lesions and rotator cuff injuries,whenpresent,isstillamatterofcontroversyinthe literature.Fewstudieshavebeenpublished,andthesehaveall beenretrospective.Withtheadventofarthroscopyfortreating rotatorcuffinjuries,insteadofopensurgery,thebiggestissue
todayiswhetherassociatedrepairofBankartlesionsis nec-essaryornot.Itisbetterestablishedthatinthesesituations, rotatorcuffinjuriesshouldalwaysberepaired.
Theobjectivesofthisstudyweretoevaluatetheclinical outcomesfromarthroscopicfixationoftherotatorcuffand, when present, simultaneous correction of Bankart lesions causedbytraumaticanteriordislocationoftheshoulder;and to evaluatewhether the magnitudeof rotator cuffinjuries causedbytraumaticdislocationinfluencedthepostoperative clinicalresults.
Material
and
methods
This was a retrospective study covering the period from September1998toMarch2012.Overthisperiod,36patients withtraumaticanteriordislocationoftheshoulderin asso-ciationwithcompletetearingoftherotatorcuffunderwent surgicaltreatmentbymeansofvideoarthroscopy.Thepatients wereoperatedbythefourtitularsurgeonsofthegroup.
The inclusion criteria were that the patients needed to haveaclinicalandradiographicdiagnosisoftraumatic ante-rior glenohumeraldislocationinassociationwith complete tearingoftherotatorcuffandthattheircaseswere reeval-uatedbymeansofmagneticresonanceimagingandclinical examinationafteraminimumfollow-upoftwoyears.
arthrosis,incomplete documentation, not locatedfor eval-uation, fractureassociatedwiththe scapularbelt, previous neurologicallesionsandBankartlesionswithbonelossfrom theglenoidgreaterthan20%oftheanteroposteriordiameter, withinjurytotheanteroinferiorcapsulealone.
Thisstudywasapprovedbytheethicscommitteeofthe orthopedicshospital.
Thirty-threepatientsfulfilledtheprerequisitesfor partici-pationinthestudy:22males(67%)and11females(33%).Their meanagewas56years(range:34–81).
All the patients were right-handed. Twenty-four were affectedintherightshoulder(72%)andnineintheleft shoul-der(28%).
Theminimumlengthoffollow-upwas24monthsandthe maximumwas108months;themeanwas39months.
Thetraumaticcausewasthereasonforcomingtothe ini-tialconsultation,inthecasesofallthepatients.
Thenumberofdislocationsrangedfromonetomorethan 20episodes:18patients(54%)presentedonlyoneepisode;13 (40%)fromtwototen;andtwo(6%),morethan20dislocations. Twenty-two patients (66%)presented Bankart lesions in associationwithcompletetearingofthetendonsofthe rota-torcuff.Elevenpatients(33%)presentedshoulderinstability, withcompletetearingofthetendonsoftherotatorcuffbut withoutthepresenceofBankartlesions.
Toclassifytheinjuries,thecriteriaofCofield10wereused. Forthepurposesofstatisticalanalysis,thesmalland medium-sizedinjurieswereputtogetherintogroupAandthe large andextensiveinjuriesintogroupB.Thus,20patients(60%)
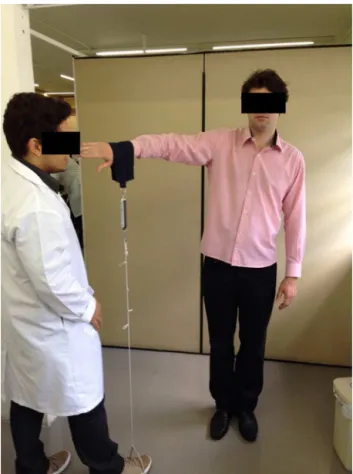
Fig.1–Positioningmethodandmeasurementofstrength usingadomesticspringbalance,inaccordancewiththe positionoftheJobetest.
presentedrotatorcuffinjuriessmallerthan3cm(smalland medium-sizedgroup)and13(40%)hadinjuriesgreaterthan orequalto3cm(largeandextensivegroup),inthe anteropos-teriordimensionoftheinjuries.
Two patientspresented three-way associations between dislocation, rotator cuff injury and axillary nerve injury (“unfortunatetriad”).
Aftertheoperation,thefunctionalevaluationwasmade using the UCLA score.11 Strength was evaluated using a domesticspringbalancewithamaximumloadof12kg (Per-formance Plus®),withthepatientpositionedinaccordance withtheJobetest,i.e.atabductionof90◦ and frontal-plane flexion of30◦, inanupright standing position (Fig. 1).The elbowwaskeptextended,withmaximumpronationofthe forearm.12Withoneoftheextremitiesofthestrength mea-surementdevicefixedtothepatient’sfootandtheotherto thelimbthatwastobeexamined,thepatientwasaskedto maintainmaximumdistensionofthesystemforfiveseconds andtheforceattainedwasrecorded.13
Allthepatientswereevaluatedusingradiographicimages in viewsthat compriseda traumaseries14: neutral antero-posteriorview,withthe patientinclinedat30◦ on theside examined; “true anteroposterior view”; lateral view of the scapula;andsimplelateralviewoftheaxilla.Inaddition,the lateralviewoftheacromion(outletview)14andstrictlateral viewoftheglenoid(Bernageauview)15wereused.
Surgicaltechnique
Thesurgicalpositionusedforallthepatientswhounderwent arthroscopic repairwaslateral decubitus,withlongitudinal andverticaltractiononthelimb.
The procedure was started with joint inspection,16 by means ofaposterior portal.When a lesionofthe anterior labroligamentous complex was present, an anterosuperior portalandananteroinferiorportalwereadded.17
Two or threethreadedmetalanchors ofdiameter4mm wereinsertedinaccordancewiththeextentofthelabral dein-sertion.Non-absorbableno.2threadswereattached tothe anchors, andthesewere usedforcapsulolabral reconstruc-tion,withretensioningoftheanteroinferiorlabroligamentous complex(capsularshifteffect)(Fig.2).18
Tenotomy ofthe bicepswasperformed whentherewas evidenceofadvanceddegenerationorinstability.
After the procedure on the joint, bursectomy was per-formed, with debridement of the borders of the lesion. Measurementsweremadealongitsanteroposteriorand lat-eromedialaxesusingamillimeterruler.19
Threadedanchorsofdiameter5mmwereinsertedinthe greater tubercle,withnon-absorbableno.2threadattached tothem.Thesynthesisonthe lesionwas performedusing tendon-bone sutures and modified Mason-Allen stitches20 and/orside-to-sidestitches,dependingontheelasticityand shapeofthelesion(Figs.3and4).
Acromioplastywasperformedwhensignsofsubacromial frictionwereseenduringbursoscopicinvestigation.
Fig.2–Suturingandretensioningofthecapsulolabral complexusinganchorsandhigh-tensionthread.
Fig.3–MethodforperformingMason-Allenstitches,with passageofasimplestitchthroughtheU-shapedstitch (mattress)thatservesasananchor.
Fig.4–FinalviewoftheMason-Allenstitch.
oftheacromialextremityoftheclavicle(totalMunford pro-cedure)wasindicatedwhentherewereradiographicsignsof jointdegeneration,inassociationwithawell-definedclinical conditionoflocalpain.
Thepatientswereinstructedtouseanabductionslingwith anauxiliarypadforaminimumofthreeweeksincasesof rotatorcuffinjuriesofupto2cmindiameterandforsixweeks incasesofinjuriesgreaterthan2cm.
Aftertheslinghadbeenwithdrawn,arehabilitation pro-gram was started, consisting of analgesia, hydrotherapy, rehabilitationofthepassiveandautopassiverangesofmotion (ROM). Strengthening of the rotator cuff muscles, initially bymeans ofisometric exercises, wasstarted 60 daysafter the operationincasesoflesions smallerthan 2cmand 90 daysaftertheoperationincasesoflesionslargerthan2cm, providedthatthepassiveROMhadbeenrecovered.Isotonic strengtheningwasintroduced90daysaftertheoperationfor thelesionssmallerthan2cmand120daysaftertheoperation forthelesionslargerthan2cm.Patientswereallowedtoreturn tosportssixmonthsaftertheoperation.Forcontactsports,the returnwasdelayeduntileightmonthsaftertheoperation.
Evaluationofthepatients
Thepatientswereevaluatedclinicallyaftertheoperationby meansoftheUCLAscore.Theirstrengthwasmeasuredwith theaidofadomesticspringbalance,asmentionedearlier.
Statisticalanalysis
To evaluatedifferences inUCLA scoresafter the operation betweenthepatientgroups,theMann–Whitneytestwasused. Thedatafromthisstudywereprocessedusingthe Statis-ticalPackagefortheSocialSciences(SPSS),version17.0.The significancelevelwastakentobep<0.05,forallthestatistical measurementsmade.
Results
TheUCLAvariablewasevaluatedstatisticallywiththe vari-ableofpresenceofBankartlesionsandwiththevariableof absenceofBankartlesions,andnostatisticaldifferencewas seenbetweenthem(Table1).
InevaluatingthevariableofpostoperativeUCLAscorein relationtogroupsAandBoftherotatorcuffinjuries (respec-tively,lesionssmallerthan3cmandgreaterthanorequalto 3cm),nostatisticaldifferencewasobserved(Table1).
Discussion
Dislocationoftheshoulderassociatedwithrotatorcuffinjury isgreatlystudiedtoday.However,althoughthisisarelatively frequentoccurrence,fewstudiesonthistopichavebeen pub-lished.
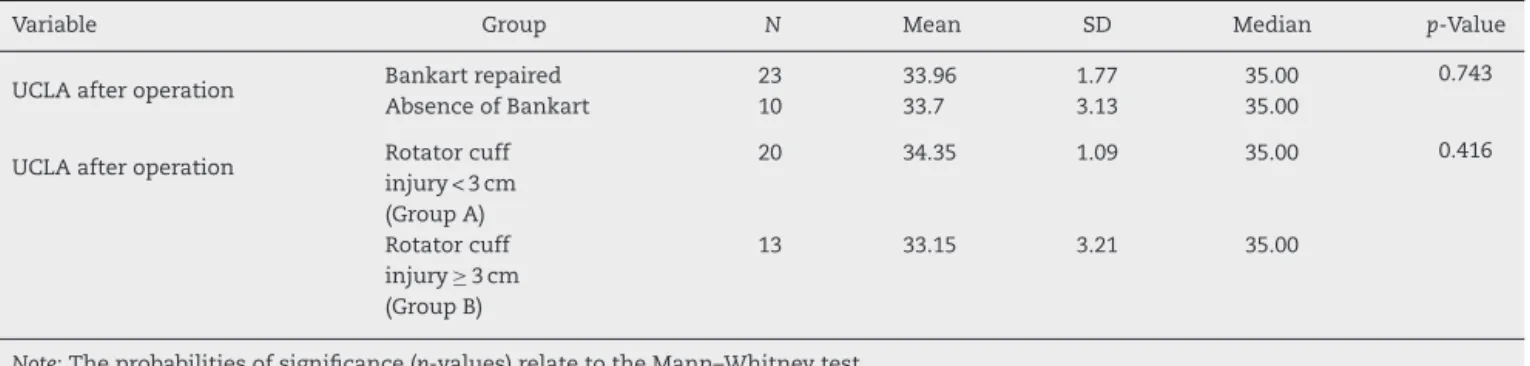
Table1–PatientdistributionaccordingtoUCLAscoreandthevariablesofrepairornon-repairoftheBankartlesionand extentoftherotatorcuffinjury.
Variable Group N Mean SD Median p-Value
UCLAafteroperation Bankartrepaired 23 33.96 1.77 35.00 0.743
AbsenceofBankart 10 33.7 3.13 35.00
UCLAafteroperation Rotatorcuff injury<3cm (GroupA)
20 34.35 1.09 35.00 0.416
Rotatorcuff injury≥3cm (GroupB)
13 33.15 3.21 35.00
Note:Theprobabilitiesofsignificance(p-values)relatetotheMann–Whitneytest.
patient(3%)undertheageof40yearspresentedrotatorcuff injuriesinassociationwithdislocation.
Berbiget al.5 evaluated167 patientsafter dislocationof theshoulder.Amongpatientswithanteriordislocationofthe shoulderwhowereundertheageof60years,theincidence ofrotatorcuffinjurieswas8.2%.Amongthoseovertheageof 60years,theincidenceofassociatedrotatorcufflesionswas 56%.Inourstudy,42%oftherotatorcuffinjurieswerepresent amongpatientsovertheageof60yearsand58%belowthis age.
Mostofthestudieshaveonlyaddressedrepairofrotator cuffinjuriesandhavenotevaluatedBankartlesions,regarding theirpresenceor absenceor regardingtheirrepairor non-repair.InrelationtoBankartlesions,authorssuchasPorcellini etal.24haveproposedthattheyarepresentinallcases.They arguedthatrotatorcuffinjurieswereinconsistentand there-foretreatmentofBankartlesionsshouldbeconsideredtobe essentialforthesepatients.Theyfoundamean postopera-tiveConstant scoreforcombined repairofthe rotator cuff andBankartlesionsof69.4.Otherauthors,suchasGumina etal.,25wereabletoreportresultsthatwereevenmore sat-isfactory.In threeout offivepatients withdislocationand rotatorcuffinjuries,inwhomBankartlesionswerepresent and were repaired,the mean postoperative Constantscore was77.Lastly,inaretrospectivestudy,Voosetal.26analyzed theresultsfromrepairstorotatorcuffinjuriesthatwere asso-ciatedwithBankartlesions,withoutdiscriminatingbetween partialand completerotator cufftears.Theyfoundthat16 patientspresentedameanpostoperativeASESscoreof95.8. Inourstudy,wefoundthat10patientswithdislocation pre-sentedrotatorcuffinjurieswithoutanyBankartlesion.Repair ofthesecasesofrotatorcuffinjuryalonedidnotpresentany statisticallysignificantdifferenceinUCLAscores,inrelation tothegroupof23patientsinwhomBankartlesionswerealso presentandwererepaired(33.7vs33.96,respectively).
Taking into consideration the extent ofthe rotator cuff injury and the clinical repercussions of its surgical repair amongthe patientswith traumaticdislocationand rotator cuffinjury,thereisanevengreaterscarcityofstudiesinthe literature.Guminaetal.25obtainedameanpostoperative Con-stantscoreof80points,forfivepatientswithlargeinjuries whounderwentrepairoftherotatorcuffalone,witha min-imumfollow-upoftwoyears.Forthreepatientswithsmall ormedium-sizedinjuries,theresultwasascoreof78points forthe same procedure. For three patients withextensive
injuries,simultaneousrepairproducedapostoperative Con-stantscoreof77points.Thus,thesescoreswereverysimilar anddidnotshowanysignificantdifference.Theirstudywas concordantwithourresults,inwhichthepatientsingroup AobtainedapostoperativeUCLAscoreof34.35,whilegroup Bhad apostoperativescoreof33.15, whichwasalsonota statisticallysignificantdifference.Inaretrospectiveanalysis on150patientsbetweentheagesof40and60years,withthe samediagnosis,Porcellinietal.24alsodidnotfindany statisti-callysignificantassociationsbetweenpatientswithcomplete tearsofthesubscapularistendon,extensivetearsofthe rota-torcuffandtearsofthesupraspinatustendonalone,whichis alsoconcordantwiththedatafoundinourstudy.
Sang-JinShinetal.27showedthatthereisstillnoconsensus regardingthestructuresthatshouldberepaired:rotatorcuff injuries,Bankartlesions,orboth.Theseauthorsshowedthat onlythroughrepairingbothstructurescouldshoulderstability berestoredwithoutlosingrangeofmotion.Theyalsoreported thatwhenbothstructureswererepaired,attentionwasgiven totakingcaretoavoidexcessivetensioningofthesuture,so astoavoidtheriskofstiffnessandsecondaryarthrosis.
With advances in arthroscopy and better knowledgeof theanatomyandphysiologyoftheshoulderjoint,the con-cept ofinstabilityhas becomemorewide-ranging and has ceasedtomeanonlydislocationsandsubluxation.This con-cepthascometoincludedysfunctionsoftheshouldercaused bymicroinstability,whichespeciallyinthiscontext,maybe causedbytheexistenceofanuncorrectedBankartlesion.This mayoriginateclinicalmanifestationsofpainandfunctional deficit,especiallyamongpatientsintheagegroupofover40 yearswhopracticesportsthatinvolvethrowing.28
Wedidnotobserveanycasesofrecurrenceofdislocation, subluxationorpainfultrappingaftertheoperationamongthe patientsevaluated,eitheringroupAoringroupB.Thisshows thatthetreatmentwaseffective,andthattherewasno corre-lationwiththeextentoftheinitialinjurytotherotatorcuff.
firsttodescribetheterribletriad,whichwaspresentedintwo patients.Althoughoneoftheirpatientspresentedincomplete neurologicalrecoveryattheendoftwoyears,thefunctional recovery ofboth of their patients was complete. However, differingfromourstudy,therotatorcuffinjurywastreated conservativelyinbothoftheircase.Likewise,otherauthors suchasGonzalesand Lopez30 and SimonichandWright,31 whotookthesameapproachasinourstudy,obtainedgood clinicalresultsattheendoftwoyearsoffollow-up.
Thepresentstudyhadthelimitationsofbeing retrospec-tiveandnothavingacontrolgroupformedbypatientswith Bankartlesionswhodidnotundergosurgicalrepair.
Conclusion
Thefunctionalresultsfromthepatientswhopresented com-pletetearingoftherotatorcuffalone,subsequenttotraumatic dislocationoftheshoulder,andwhounderwentarthroscopic repair, were shown to be similar to the results from the patientswhopresentedassociatedBankartlesionsthatwere correctedsimultaneouslywiththerotatorcuffinjuries.
Theextentoftheinitialinjurytotherotatorcuffdidnot alterthefunctionalresultsinthepostoperativeevaluation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BahkM,KeyurapanE,TasakiA,SauersEL,McFarlandEG. Laxitytestingoftheshoulder:areview.AmJSportsMed. 2007;35(1):131–44.
2. ReevesB.Arthrographyoftheshoulder.JBoneJointSurgBr. 1966;48(3):424–35.
3. TaylorDC,ArcieroRA.Pathologicchangesassociatedwith shoulderdislocations.Arthroscopicandphysical examinationfindingsinfirst-time,traumaticanterior dislocations.AmJSportsMed.1997;25(3):306–11. 4. HawkinsRJ,MorinWD,BonuttiPM.Surgicaltreatmentof
full-thicknessrotatorcufftearsinpatients40yearsofageor younger.JShoulderElbowSurg.1999;8(3):259–65.
5. BerbigR,WeishauptD,PrimJ,ShahinO.Primaryanterior shoulderdislocationandrotatorcufftears.JShoulderElbow Surg.1999;8(3):220–5.
6. McLaughlinHL.Injuriesoftheshoulderandarm.In: McLaughlinHL,HarrisonL,editors.Trauma.Philadelphia: Saunders;1959.p.233–96.
7. NeviaserRJ,NeviaserTJ,NeviaserJS.Concurrentruptureof therotatorcuffandanteriordislocationoftheshoulderinthe olderpatient.JBoneJointSurgAm.1988;70(9):1308–11. 8. DebskiRE,SakoneM,WooSL,WongEK,FuFH,WarnerJJ.
Contributionofthepassivepropertiesoftherotatorcuffto glenohumeralstabilityduringanterior-posteriorloading.J ShoulderElbowSurg.1999;8(4):324–9.
9. CraigEV.Theposteriormechanismofacuteanteriorshoulder dislocations.ClinOrthopRelatRes.1984;(190):212–6.
10.CofieldRH.Subscapularmuscletranspositionforrepairof chronicrotatorcufftears.SurgGynecolObstet.
1982;154(5):667–72.
11.AmstutzHC,SewHoyAL,ClarkeIC.UCLAanatomictotal shoulderarthroplasty.ClinOrthopRelatRes.1981;(155):7–20.
12.JobeFW,MoynesDR,BrewsterCE.Rehabilitationofshoulder jointinstabilities.OrthopClinNorthAm.1987;18(3):473–82. 13.GodinhoGG,SantosFM,FreitasJM.Avaliac¸ãodaforc¸a
muscularedafunc¸ãodoombro,apósreparodomanguito rotador.RevBrasOrtop.1994;29(9):643–6.
14.RockwoodCAJr,SzalayEA,CurtisRJ,YoungDC,KaySP.X-ray evaluationofshoulderproblems.In:RocwoodCAJr,Matsen FA,editors.Theshoulder.Philadelphia:Saunders;1990.p. 178–200.
15.BernageauJ,PatteD,DebeyreJ,FerraneJ.Intérêtduprofil glénoidiendansleluxationrécidivantesdel’épaule.RevChir Orthop.1976;Suppl.2:62.
16.GodinhoGG,SouzaJM,OliveiraAC,FreitasJM.Artroscopia cirúrgicanotratamentodasíndromedoimpacto:nossa experiênciaem100casoscirúrgicos.RevBrasOrtop. 1995;30(3):540–6.
17.GodinhoGG,SouzaJM,FreitasJM,SantosFM,VieiraAW,João FM.Tratamentodainstabilidadeanteriordoombro– ExperiênciacomatécnicadeMorgan.RevBrasOrtop. 1997;32(4):261–5.
18.GodinhoGG.Tratamentocirúrgicodainstabilidadeanterior doombropelatécnicaartroscópica.In:PardiniJuniorAG, editor.Clínicaortopédica.RiodeJaneiro:Medisi;2004. 19.GodinhoGG.Reparodaslesõesdomanguitorotadorporvia
artroscópica.In:PardiniJuniorAG,editor.Clínicaortopédica. RiodeJaneiro:Medisi;2000.
20.SchlegelTF,HawkinsRJ,LewisCW,TurnerAS.Aninvivo comparisonofthemodifiedMason-Allensuturetechnique versusaninclinedhorizontalmattresssuturetechniquewith regardtotendon-to-bonehealing:abiomechanicaland histologicstudyinsheep.JShoulderElbowSurg. 2007;16(1):115–21.
21.RoweCR.Prognosisindislocationsoftheshoulder.JBone JointSurgAm.1956;38-A(5):957–77.
22.ReevesB.Acuteanteriordislocationoftheshoulder.Clinical andexperimentalstudies.AnnRCollSurgEngl.
1969;44(5):255–73.
23.ItoiE,TabataS.Rotatorcufftearsinanteriordislocationof theshoulder.IntOrthop.1992;16(3):240–4.
24.PorcelliniG,PaladiniP,CampiF,PaganelliM.Shoulder instabilityandrelatedrotatorcufftears:arthroscopicfindings andtreatmentinpatientsaged40to60years.Arthroscopy. 2006;22(3):270–6.
25.GuminaS,PostacchiniF.Anteriordislocationoftheshoulder inelderlypatients.JBoneJointSurgBr.1997;79(4):540–3. 26.VoosJE,PearleAD,MatternCJ,CordascoFA,AllenAA,Warren
RF.Outcomesofcombinedarthroscopicrotatorcuffand labralrepair.AmJSportsMed.2007;35(7):1174–9. 27.ShinSJ,YooJC,McGarryMH,JunBJ,LeeTQ.Anterior
capsulolabrallesionscombinedwithsupraspinatustendon tears:biomechanicaleffectsofthepathologicconditionand repairinhumancadavericshoulders.Arthroscopy.
2013;29(9):1492–7.
28.BoileauP,ZumsteinM,BalgF,PeningtonS,BicknellRT.The unstablepainfulshoulder(UPS)asacauseofpainfrom unrecognizedanteroinferiorinstabilityintheyoungathlete.J ShoulderElbowSurg.2011;20(1):98–106.
29.GrohGI,RockwoodCAJr.Theterribletriad:anterior dislocationoftheshoulderassociatedwithruptureofthe rotatorcuffandinjurytothebrachialplexus.JShoulder ElbowSurg.1995;41Pt1:51–3.
30.GonzalezD,LopezR.Concurrentrotator-cufftearand brachialplexuspalsyassociatedwithanteriordislocationof theshoulder.Areportoftwocases.JBoneJointSurgAm. 1991;73(4):620–1.