www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Assessment
of
hearing
threshold
in
adults
with
hearing
loss
using
an
automated
system
of
cortical
auditory
evoked
potential
detection
夽
Alessandra
Spada
Durante
∗,
Margarita
Bernal
Wieselberg,
Nayara
Roque,
Sheila
Carvalho,
Beatriz
Pucci,
Nicolly
Gudayol,
Kátia
de
Almeida
FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
Received23November2015;accepted16February2016 Availableonline29April2016
KEYWORDS
Auditoryevoked potentials;
Auditoryperception; Hearingaids; Hearingloss; Electrophysiology
Abstract
Introduction:Theuseofhearing aidsbyindividualswithhearinglossbringsabetterquality oflife.Accesstoandbenefitfromthesedevicesmaybecompromisedinpatientswhopresent difficulties orlimitationsintraditionalbehavioralaudiological evaluation,suchasnewborns andsmallchildren, individualswithauditoryneuropathyspectrum,autism,andintellectual deficits,andinadultsandtheelderlywithdementia.Thesepopulations(or individuals)are unable to undergo abehavioral assessment, andgenerate agrowing demand for objective methodstoassesshearing.Corticalauditoryevokedpotentialshavebeenusedfordecadesto estimatehearingthresholds.Currenttechnologicaladvanceshaveleadtothedevelopmentof equipmentthatallowstheirclinicaluse,withfeaturesthatenablegreateraccuracy,sensitivity, andspecificity,andthepossibilityofautomateddetection,analysis,andrecordingofcortical responses.
Objective: Todetermine andcorrelate behavioralauditorythresholdswithcortical auditory thresholdsobtainedfromanautomatedresponseanalysistechnique.
Methods:Thestudyincluded52adults,dividedintotwogroups:21adultswithmoderateto severehearingloss(studygroup);and31adultswithnormalhearing(controlgroup).An auto-matedsystemofdetection,analysis,andrecordingofcorticalresponses(HEARLab®)wasused torecordthebehavioralandcorticalthresholds.Thesubjectsremainedawakeinanacoustically treatedenvironment.Altogether,150toneburstsat500,1000,2000,and4000Hzwere pre-sentedthroughinsertearphonesindescending-ascendingintensity.Thelowestlevelatwhich the subject detectedthe sound stimuluswas defined as thebehavioral(hearing) threshold (BT).Thelowestlevelatwhichacorticalresponsewasobservedwasdefinedasthecortical electrophysiologicalthreshold.Thesetworesponseswerecorrelatedusinglinearregression.
夽 Pleasecitethisarticleas:DuranteAS,WieselbergMB,RoqueN,CarvalhoS,PucciB,GudayolN,etal.Assessmentofhearingthresholdin
adultswithhearinglossusinganautomatedsystemofcorticalauditoryevokedpotentialdetection.BrazJOtorhinolaryngol.2017;83:147---54. ∗Correspondingauthor.
E-mail:[email protected](A.S.Durante).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.02.016
Results:Thecortical electrophysiologicalthresholdwas,onaverage,7.8dB higherthanthe behavioralforthegroupwithhearinglossand,onaverage,14.5dBhigherforthegroupwithout hearinglossforallstudiedfrequencies.
Conclusion:Thecorticalelectrophysiologicalthresholdsobtainedwiththeuseofanautomated responsedetectionsystemwerehighlycorrelatedwithbehavioralthresholdsinthegroupof individualswithhearingloss.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Potenciaisevocados auditivos;
Percepc¸ãoauditiva; Auxiliaresdeaudic¸ão; Perdaauditiva; Eletrofisiologia
Estimativadolimiarauditivoemadultoscomperdaauditivapormeiodeumsistema automatizadodedetecc¸ãodopotencialevocadoauditivocortical
Resumo
Introduc¸ão:Autilizac¸ãodaamplificac¸ãosonoraporpessoascomperdaauditivaofereceuma melhorqualidadedevida.Oacessoaesterecursoeoseubenefíciopodemficar comprometi-dosnocasodepacientesqueapresentemdificuldadesoulimitac¸õesnaavaliac¸ãoaudiológica tradicionalcomportamental,tais comoneonatosecrianc¸as pequenas,presenc¸adoespectro daneuropatiaauditivaedoautismo,déficitintelectualepresenc¸adeestadosdemenciaisde adultoseidosos.Estaspopulac¸ões(ouindivíduos)incapazesdeparticipardeumaavaliac¸ão com-portamentalgeramumacrescentedemandapormétodosobjetivosdeavaliac¸ãoauditiva.Os potenciaisevocadosauditivoscorticaissãoutilizadoshádecadas,comafinalidadedeestimaros limiaresauditivos.Avanc¸ostecnológicosatuaispermitiramodesenvolvimentodeequipamentos quepossibilitamseuusoclínico,dotadosderecursosquepermitemmaiorprecisão, sensibili-dadeeespecificidade,alémdapossibilidadededetecc¸ão,análiseeregistroautomatizadosdas respostascorticais.
Objetivo:Determinarecorrelacionarolimiarauditivocomportamentalcomolimiarauditivo corticalobtidosemequipamentodeanáliseautomatizadadasrespostas.
Método: Participaramdoestudo52adultos,distribuídosemdoisgrupos:21adultoscomperda degraumoderadoasevero(GrupoEstudo),e31comaudic¸ãonormal(GrupoControle).Parao registrodoslimiarescomportamentaisecorticaisfoiutilizadoumequipamentodotadodeum sistemacomdetecc¸ão,análiseeregistroautomatizadosdasrespostascorticais (HEARLab®). Osparticipantes permaneceram despertos,em um ambienteacusticamente tratado.Foram apresentados150estímulostipotoneburstnasfrequênciasde500,1.000,2.000e4.000Hz, pormeio defonesdeinserc¸ãoem intensidadesdescendente-ascendente. Omenornível no qual o sujeito detectou apresenc¸a do estímulosonoro foidefinido como o limiar auditivo comportamental.Omenor nível noqual uma respostacortical estavapresente foidefinido comoolimiareletrofisiológicocortical.Essasduasrespostasforamcorrelacionadaspormeio daregressãolinear.
Resultados: Olimiareletrofisiológicocorticalfoi,emmédia,7,8dBsuperioraocomportamental paraogrupocomperdaauditivae14,5dBsuperior,emmédia,paraogruposemperdaauditiva paratodasasfrequênciasestudadas.
Conclusão:Oslimiareseletrofisiológicoscorticaisobtidospormeiodeumsistemadedetecc¸ão automatizadoderespostasestavamfortementecorrelacionadoscomoslimiares comportamen-taisnogrupodeindivíduoscomperdaauditiva.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Theuseofhearingaidsbyindividualswithhearinglossbrings abetter qualityof life. Access toand benefitfromthese devicesmay be compromised in patients withdifficulties orlimitationsintraditionalbehavioralaudiological evalua-tion,suchasnewbornsandsmallchildren,individualswith
auditoryneuropathyspectrum,autism,intellectualdeficits, andin adultsandtheelderlywithdementia.These popu-lations(or individuals)areunabletoundergoabehavioral assessment,andgenerateagrowingdemandforobjective methodstoassesshearing.
Inthepast,the principalapplicationofthispotentialwas an objective estimation of hearing threshold in difficult-to-test adults,but it wasalso extensively investigatedin children.1
The assessment of hearing thresholds using CAEP has numerous advantages as it assesses the entire auditory systemfrombrainstemtocortex.Itcanberecordedin con-scioussubjectsusingavarietyofacousticstimulipresented either through earphones or in open field.2---5 Although it
has inestimable scientific and clinical value, the routine use of these cortical potentials has been hindered over thelastyearsbynumerousfactors.ThemainCAEP compo-nentsundergosubstantialchangesintheresponsepattern dependingonthestageofdevelopmentfrombirthto ado-lescence, as well as when the evaluation is performed during intermediate stages of drowsiness. There is also variability in response amplitude, latency, and morphol-ogyboth withinandbetween subjects.These variabilities providedifficultiesinrecognitionandinterpretationofthe responses,whichrequireexperiencedandspecialized pro-fessionals. In addition to these factors, the high cost of equipmenthasaddedtothetechnicallimitationofthe elec-trodes, filters, and amplifiers necessary to capture these potentials,anduntilrecentlyminimizedtheclinicaluseof CAEP.3,6
In order to overcome these barriers and promote its clinicaluse,theNationalAcousticLaboratory(NAL),an Aus-traliangovernmentinstitution,overthepastfewyearshas developed a device for the investigation of cortical audi-toryevokedpotentialsnamedHEARLab® (FryeElectronics;
United States). The difference of this system to its cur-rentlyavailable counterparts is that itis more affordable and has the potential for clinical use. Among other fea-tures,itcontainsadvancedanddifferentiatedtechnologies thatcanreducetheregistrationofnoiseandinterferenceby providingresidualnoisemeasurements,andhaselectrodes thataremoresensitiveincapturingresponses.However,the principaldifferenceisthatitreliesonauniquemethodof automatic detection and analysis of responses that takes into accountstatistical methods and tests, similarto the t-test, that determines the presence or absence of cor-tical response through confidence level calculations. This softwareexempts the examiner fromthe difficult taskof subjectivelyinterpretingthepresenceorabsenceofcortical responsebasedsolelyonavisualanalysis.1,3,5,7---14
The hypothesis of this study is that it is possible to estimate the behavioral hearing thresholds based on the corticalelectrophysiologicalthresholdsobtainedfrom auto-maticanalysisequipment.
In Brazil, there no studies of auditory thresholds have been performedwithanautomated analysisequipmentof corticalresponse.Thepresentstudy aimedtoanalyzethe useofCAEPtoestimatehearingthresholdsthroughan auto-matedCAEPresponseanalysisequipment.
Methods
ThisstudywasapprovedbytheResearchEthicsCommittee of theinstitution underNo.361/11. Allparticipants were informedabout theobjectives ofthe studyand signedan informedconsentform.
Caseseries
Thefollowinginclusioncriteriawereestablished:
• GroupC(control):adults(age≤65years),ofbothsexes, with normal hearing (tritonal mean of 500, 1000, and 2000Hz<20dBHL),withouthearingcomplaintsorhistory ofotologicproblems.
• Group S (study): adults(age≤65 years),of both sexes, withbilateralsymmetricalsensorineuralhearinglossthat wasmoderatetosevere(tritonalmeansof500,1000,and 2000Hz≥41dBHLand≤90dBHL).15
The exclusion criteria were the presence of neurolog-ical, psychiatric impairment, and/or declared or proven syndromes.
Procedures
Allsamplesubjectsunderwentthesameevaluationprotocol specifiedbelow.
To rule out problems in the middle ear that would prevent the inclusion in the study, visual inspection and tympanometrywereperformedusingamiddleearanalyzer (InteracousticsModelAZ-7R).
Fortheinvestigationofbehavioralpuretonethresholds, theaudiometerGNOtometricsIterawasusedwith supra-auralTDH-39earphonesinacousticbooths.Fullbehavioral audiometric evaluation was performed by pure tones at frequencies250---8000Hzfor airand500---4000Hzfor bone conductionusingthedescending---ascendingclassical tech-niqueoftonalthresholdassessment.Thesethresholdswere hereintermedaudiometricthresholds(AT).
Fortheassessmentofbehavioralhearingthresholdsfor tone burststimulus, the HEARLab® system wasused. The
equipment provides auditory stimuli at 500, 1000, 2000, 3000,and4000Hz, atintensities ranging from0to110dB HL,presented throughinsertearphones inan acoustically treated room. The descending---ascending threshold mea-surementtechniquewasused,andthelowestintensity at whichthe subjectwasabletodetect the tone burst pre-sentedwastermedbehavioralthreshold(BT).
InpreparationfortheCAEPassessment,thepatient’sskin wasproperlycleaned and prepared. The electrodes were placedaccordingtothefollowingposition:activeelectrode inthevertex(Cz),referenceelectrodeintherightor left mastoid(M1andM2),groundelectrodeintheforehead(Fz); theminimumacceptableconditionsofmaximumimpedance andbetweenelectrodes(≤5k)wereensured.Participants wereassessedwhile awake,distractedbyimagesairedon a TV without sound, in an acclimatized and acoustically treatedroom.
Assessment of BT and cortical electrophysiological threshold(CET)at 500, 1000,2000, and4000Hzwas per-formedin onlyoneearof eachsubject, chosen according tothe subject’sperception of his/her‘‘betterear’’ or at random,intheabsenceofreference.
TodetectandrecordtheCAEP,theHEARLab®systemwas
Table1 Demographicdataofsubjectsinstudyandcontrolgroups.
Group Nears(participants) Age(years) Auditorythreshold(dBHL)
Study 21(21) 48.9(±7.2) 58(±12)
Control 31(31) 23.7(±5.2) 2.1(±2.9)
Theassessmentofcorticalthresholdsfortoneburst fol-lowedthefollowingprotocol,dependingontheassessment group:1)ForGroupC,adultswithnormalhearing,theinitial intensityof70dBHLwasused;theresponsewasrecorded andthendecreasedto20dBHL.Whentherewasalso cor-ticalresponseatthatintensity,descendingintensitieswere usedinstepsof 10dBandascendingintensities of5dBup totheminimumthresholdofautomaticresponsedetection (minimumintensity). 2) ForGroup S, adults withhearing impairment,theinitialintensityof70dBHLwasalsoused. Whentherewasalsoacorticalresponse atthat intensity, descendingintensitiesinstepsof10dBandascending inten-sities of 5dB were used upto the minimum threshold of automaticresponsedetection,asinGroupC.However,ifno responsewasdetectedintheinitialintensityof70dBHL,the assessmentsurveywasperformedinincrementsofintensity in steps of 10dB and descending of 5dB up to the mini-mumthresholdofcorticalresponsedetection.Thedetected thresholdsweretermedCET.
The automatic detection of the presence and respec-tivecorticalresponsethresholdtoacousticstimulationtakes intoaccountthestatisticalp-valueinanexclusivesoftware providedwiththeequipment.The lower thep-value,the greatertheprobabilitythattherecordedwaveisrelatedto thesoundstimulus.Ap-valueof0.05isthethreshold con-sideredbytheequipmentandexaminerfordecision-making regardingthepresenceorabsenceofcorticalresponse;that is,thisthresholdmeansthattherewouldbeonlya5%chance forthisequipmenttorecordaresponseasfalse-positive.
Statisticalanalysis
For statistical analysis, central tendency measurements, Pearson’scorrelation,andlinearregressionwereused.
Inalltests,a0.05significancelevel(or5%)wasusedto rejectthenullhypothesis.
Results
Thefinalsampleofthisstudyincludedtheparticipationof 52 adult subjects (total),divided intotwo groups, Group CandGroupS,composedofindividuals withnormal hear-ing and hearing loss, respectively. In Group C, 31 adults wereevaluated:23(74.2%)femalesandeight(25.8%)males; mean age of 23.7 years (SD=5.2 years), with mean tri-tonalaudiometric thresholdsof2.1dBHL(SD=2.9dBHL). InGroupS,21adultsparticipated:15(71.4%)femalesand six(28.6%)males,meanageof48.9years(SD=7.2years), withmeantritonalvaluesat500,1000,and2000Hzof58dB HL(SD=12dBHL;Table1).
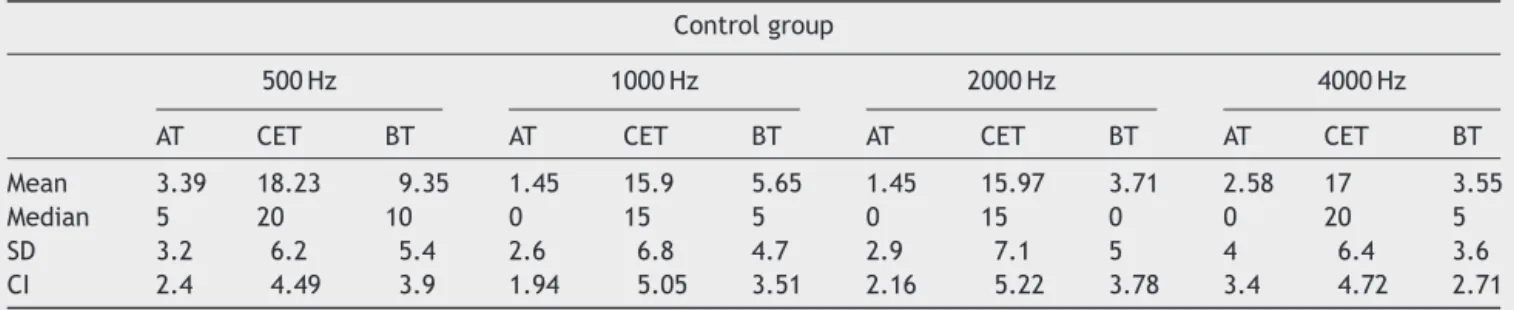
DescriptivemeasuresofAT,BT,andCETforthe frequen-cies of500,1000,2000,and4000Hzareshownin Table2 forGroupCandinTable3forGroupS.
At all frequencies, it could be observed that CET had higherthresholds comparedtoAT. Onaverage, the differ-ences between these thresholds were 8.6, 9.6, 6.0, and 7.1dB for frequencies of 500Hz, 1000Hz, 2000Hz, and 4000Hz,respectively, in Group S. For Group C,the mean differenceswere14.8,14.5,14.5,and14.8dB,respectively, forthesamefrequencies.
ThelinearregressionanalyzesperformedbetweenATfor puretone(‘‘goldstandard’’)andBTforspecific-frequency stimuli (tone bursts) showed that these thresholds are strongly correlated to all frequencies (r2≥0.7) in both
groups.Thus,itwasdecidedtocorrelatethebehavioraland electrophysiologicalthresholds.
InGroupC,thecorrelationbetweenCETandBTwaspoor. However, in Group S, the strong correlation between the twomeasuresisevidencedbyr2=0.71;0.72;0.83,and0.80
forallstudiedfrequenciesof500Hz,1000Hz,2000Hz,and 4000Hz,respectively.Fig.1showsthescatterplotsofGroup S,forthefouraudiometricfrequenciesseparatelywithCET ontheverticalaxisandBTonthehorizontalaxis.
Table2 Descriptivemeasures of auditory, electrophysiological, and behavioral thresholds obtained for control group by frequency.
Controlgroup
500Hz 1000Hz 2000Hz 4000Hz
AT CET BT AT CET BT AT CET BT AT CET BT
Mean 3.39 18.23 9.35 1.45 15.9 5.65 1.45 15.97 3.71 2.58 17 3.55
Median 5 20 10 0 15 5 0 15 0 0 20 5
SD 3.2 6.2 5.4 2.6 6.8 4.7 2.9 7.1 5 4 6.4 3.6
CI 2.4 4.49 3.9 1.94 5.05 3.51 2.16 5.22 3.78 3.4 4.72 2.71
Table3 Descriptivemeasuresofauditory,electrophysiological,andbehavioralthresholdsforthestudygroupbyfrequency.
Studygroup
500Hz 1000Hz 2000Hz 4000Hz
AT CET BT AT CET BT AT CET BT AT CET BT
Mean 49.2 57.8 55.2 56.1 65.7 60 57.1 63.1 60 55 62.1 57.8
Median 50 60 60 60 65 60 60 60 60 55 65 60
SD 13.8 6.2 13.8 12.9 9.7 12.9 11.3 11.2 9.8 11 10.3 11.2
CI 12.57 4.59 12.59 11.78 8.91 11.78 10.34 10.23 8.98 10.1 9.39 5.24
SD, standarddeviation; CI,confidenceinterval; AT, auditorythreshold;CET,cortical electrophysiologicalthreshold;BT, behavioral threshold.
Discussion
This study assessed and compared the behavioral hearing thresholdsobtainedthroughpuretones(‘‘goldstandard’’ ---AT)andthroughspecificfrequencies(toneburst---BT)ofall individuals in thesample, for both groups withloss hear-ingandwithnormalhearing.Duetothestrongcorrelation between thetwo thresholdsfor all frequencies (r2≥0.7); regardlessofthegroup,wechoseinthisstudytocorrelate CETwithBT.
Given that the criteria for inclusion in the sample of both groups assumed the presence of symmetrical tonal thresholds bilaterally and aiming to reduce the duration ofthetest,theauthorschosetoassesstheBT andCETat
frequencies of 500, 1000, 2000, and 4000Hz only in one earof each subject,chosen according totheirperception of their ‘‘better ear’’ or, in the absence of reference, randomly. In the study by Frizzo et al.,16 there were no
statistically significant differences between the cerebral hemispheres that could hinder the CAEP assessment on eitherear.Thus,theevaluationprotocolandmeasurement of behavioral and electrophysiological thresholds had an approximatedurationof60minpersubject.
The technicalprotocol usedwasthat suggested bythe manufacturer of the HEARLab System® (Frye Electronics,
UnitedStates).Theimpedanceofelectrodesremained bal-ancedanddidnotexceed5k.Thesoundstimulipresented through insert earphones were tone bursts with 150s
100
50
0
0 20 40 60
500 Hz 1000 Hz
4000 Hz 2000 Hz
80 100 120
0 20 40 60 80 100 120 0 20 40 60 80 100 120
0 20 40 60 80 100 120
100
50
0
100
50
0
100
50
0
r2=0.71
r2=0.83 r2=0.80
r2=0.72
Cor
tical electroph
ysiological threshold (dB HL)
Behavioral threshold (BT)
Durante
AS
et
al.
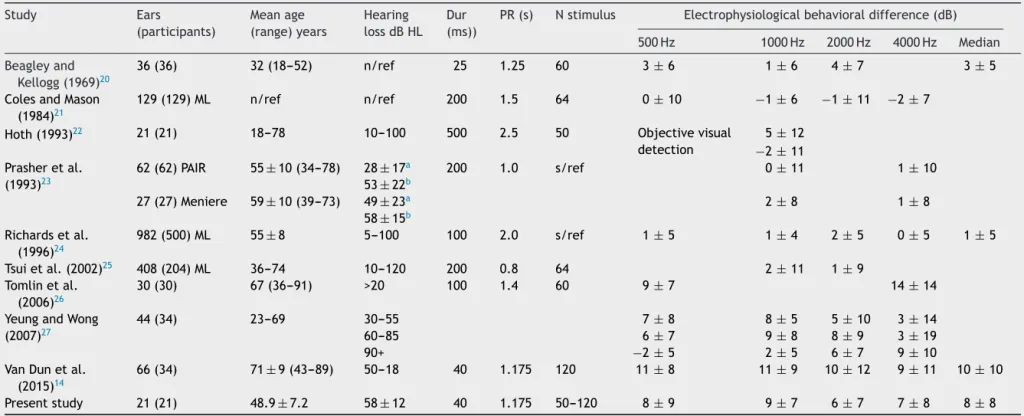
Table4 OverviewofstudiesperformedwithadultswithhearinglossforbehavioralauditorythresholdassessmentusingCAEP.
Study Ears
(participants)
Meanage (range)years
Hearing lossdBHL
Dur (ms))
PR(s) Nstimulus Electrophysiologicalbehavioraldifference(dB)
500Hz 1000Hz 2000Hz 4000Hz Median
Beagleyand Kellogg(1969)20
36(36) 32(18---52) n/ref 25 1.25 60 3±6 1±6 4±7 3±5
ColesandMason (1984)21
129(129)ML n/ref n/ref 200 1.5 64 0±10 −1±6 −1±11 −2±7
Hoth(1993)22 21(21) 18---78 10---100 500 2.5 50 Objectivevisual
detection
5±12
−2±11 Prasheretal.
(1993)23
62(62)PAIR 55±10(34---78) 28±17a 200 1.0 s/ref 0±11 1±10
53±22b
27(27)Meniere 59±10(39---73) 49±23a 2±8 1±8
58±15b
Richardsetal. (1996)24
982(500)ML 55±8 5---100 100 2.0 s/ref 1±5 1±4 2±5 0±5 1±5
Tsuietal.(2002)25 408(204)ML 36---74 10---120 200 0.8 64 2±11 1±9
Tomlinetal. (2006)26
30(30) 67(36---91) >20 100 1.4 60 9±7 14±14
YeungandWong (2007)27
44(34) 23---69 30---55 7±8 8±5 5±10 3±14
60---85 6±7 9±8 8±9 3±19
90+ −2±5 2±5 6±7 9±10
VanDunetal. (2015)14
66(34) 71±9(43---89) 50---18 40 1.175 120 11±8 11±9 10±12 9±11 10±10
Presentstudy 21(21) 48.9±7.2 58±12 40 1.175 50---120 8±9 9±7 6±7 7±8 8±8
Dur,duration;n/ref,noreference;PR,presentationrate;ML,medico-legal;NIHL,noise-inducedhearingloss.
a 1000Hz. b 2000Hz.
Note:Studiesinvolvingseveralindividuals(participantswithnormalhearingandhearingloss)thatcouldnotbeseparatedwerenotincluded.AllCAEPwereevaluatedbyvisualinspection oftheresponses,exceptinthestudiesbyHoth,22VanDunetal.,14andthepresentstudy.ThistablestructureissimilartoTable11.1byPicton.28Allstudies,exceptthosebyBeagleyand
Kellogg,20ColesandMason,21andRickardsetal.,24definedthresholdasthelowestintensitylevelatwhicharesponsecouldbeidentified.ThethresholdsbyBeagleyandKellogg20were
furtherreducedby2.5dB.ColesandMason21considered5dBthebestestimatethreshold.Rickardsetal.24consideredtheCAEPlowestintensitydetectionor5dBreduction,depending
ontheusedcriterion.
duration, although Lightfoot17 has reported that the use
of 10---20s duration stimuliare sufficient tocapture the
response, except when it is near the subject’s cortical threshold.
In thepresentstudy,subjectalertnessduring the eval-uationwascontrolledandmaintained.Näätänen18 warned
oftheinfluenceofdrowsinesseffectsonvariabilityof corti-calresponses.Unliketheshort-latencyelectrophysiological responses,whichrequirequalitycontrolandmuscle relax-ationduringthecaptureofCAEP,thesubjectsimplyneeds tostayawake andconsciouslyalert.This canbeachieved by askinghim/her toremain inthe sittingposition,while entertainedwiththeimagesofavideowithoutsound,for example. The differenceof this system over its currently availablecounterparts,isthatitisadevicewithadvanced anddifferentiatedtechnologiesthat,inadditiontoreducing the registration noise and interference, provides residual noise control measures and features increased-sensitivity electrodesforthecaptureofresponses.3
TheautomaticCAEPresponsesdetectionequipmentaims tofacilitate the examiner’s task of subjectively interpre-tingtheelectrophysiologicalwavesbasedsolelyonavisual analysisforthepresenceorabsenceofcorticalresponseto acousticstimuli.Thestatisticalmethodusedinthe equip-ment wasshown in previous studies tobe able todetect corticalresponseswithcombinedsensitivityandspecificity equal to or greater than that achieved by experienced examiners,3,9resultsthataresupportedinthepresentstudy.
In GroupS, the meandifferencesbetween CETandBT were 7.8dB. The values found in this study are slightly higher than thosereported in a preliminary study by Van Dun et al.,11 whose differences for the same frequencies
rangedfrom3.4to5.9dB.Inastudybythissameauthor,14
investigatingCAEPthresholdsin34adultswithhearingloss, theCETwereonaverage10dBhigher(SD=10dB)thanthe BT,similarresultstothepresentstudy.
Table 4 presents an overview of the studies that esti-matedtheauditorythresholdinadultsubjectswithhearing loss,reportingdifferencesbetweencortical electrophysio-logical andbehavioral thresholdsranging from9to14dB, withstandarddeviationof5---14dB.
In Group C, the differences between thresholds were higher(meanof14.5dB)forthesamefrequenciesstudied. Themeandifferencebetweenthepresentstudythresholds was similar to that found in the study by Lightfoot and Kennedy.19 They evaluated 24 adult subjects with normal
hearing andconcluded that94% of the sample thresholds were estimated with a difference ≤15dB and 80% could havetheir thresholdsestimated withadifference≤10dB. Thoseauthorsreportedthat,althoughthemeandifference betweenthethresholdswasbetween5and10dBinmostof thesample,itwasfoundthatinasmallsubsample(7%)the differencesbetweenthethresholdswereupto20dBhigher forBT.VanDunetal.14studyingindividualswithhearingloss,
alsoreportedthepresenceof4%ofwhattheycalled‘‘out of the curve’’ differences, referring to the subjects that presenteddifferencesbetweenthresholdsupto30dB,with corticalthresholdCETalwayshigherthanBT.Inthepresent study, this smallgroup was also present in 4% of records withdifferencesupto30dB.Paradoxically,cortical thresh-oldresponses,comparativelylowerthanthoserecordedfor BTsupto10dBwerealsoobservedin2.4%ofrecords.
When comparing the mean detection and response thresholdsofCAEPbetweenthegroupsofsubjectswith nor-malhearingandsubjectswithhearingloss,thedifference betweenBT andCET washigherinthe Group C.This dif-ferencebetweengroupswasalsoreportedinthestudyby Goldingetal.3Apossibleexplanationforthesubjectsinthe
GroupStorecordCETclosertotheBTorwithaminor sen-sationlevel(SL)appearsbebasedonthepotentialimpact oftherecruitmentphenomenononthosesubjectswith sen-sorineuralhearingloss,whichwouldincreasetheamplitude ofCAEPresponseatlowerorweakerSLs.9,10
Given the findings of this study, the CAEP obtained throughautomaticresponseanalysisequipmentwasshown tobe a viable test to estimate the auditory threshold in adultswithhearingloss.
Complementary studies using the automatic cortical responsethreshold analysis equipment would be of great clinical relevance to establish correction factors for the assessmentofhearingthresholds,aswellastheevaluation ofdifferentpopulations.
Conclusion
The results of this study indicated a strong correlation betweenbehavioral thresholdsand cortical electrophysio-logicalthresholds for frequenciesof 500,1000, 2000,and 4000Hzinadultswithhearingloss.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The authors would like thank the Fundac¸ão de Amparo a PesquisadoEstadodeSãoPaulo(FAPESP)forthe encourage-mentandfundingofthisstudy(processNo.2011-19556-3), andProfessorsVanDunB,DillonH,andSeetoMwhoallowed theadaptationofTable4presentedinthisstudy.
References
1.PurdySC,KatschR,DillonH,StoreyL,SharmaM,AgungK.Aided corticalauditoryevokedpotentialsforhearinginstrument eval-uationininfants.In:SeewaldRC,BamfordJM,editors.Asound foundationthroughearlyamplification.ProceedingsoftheThird internationalconference.Basel,Switzerland:PhonakAG;2005. p.115---27.
2.HallJW.Newhandbookofauditoryevokedresponses.Boston, MA:Pearson,AllynandBacon;2007.
3.GoldingM,DillonH,SeymourJ,CarterL.Thedetectionofadult corticalauditoryevokedpotentials(CAEPs)usinganautomated statisticandvisualdetection.IntJAudiol.2009;48:833---42.
4.AlvarengaKF, Vicente LC,Lopes RCF, SilvaRA, Banhara MR, Lopes AC,etal. Influênciadoscontrastesde falanos poten-ciais evocados auditivos corticais. Braz J Otorhinolaryngol. 2013;79:336---41.
6.CampbellK,ColrainI.Event-relatedpotentialmeasuresofthe inhibitionofinformationprocessing:II.Thesleeponsetperiod. IntJPsychophysiol.2002;46:197---214.
7.Ching TYC, Dillon H. Prescribing amplification for children: adult-equivalenthearingloss,real-earaidedgain,andNAL-NL1. TrendsAmplif.2003;7:1---9.
8.DillonH.So,baby,howdoesitsound?Corticalassessmentof infantswithhearingaids.HearJ.2005;58:10---7.
9.CarterL,GoldingM,DillonH,SeymourJ.Thedetectionofinfant corticalauditoryevokedpotentials(CAEPs)usingstatisticaland visualdetectiontechniques.JAmAcadAudiol.2010;21:347---56.
10.Munro KJ, Purdy SC, Ahmed S, Begum R, Dillon H. Obliga-torycorticalauditoryevokedpotentialwaveformdetectionand differentiationusingacommerciallyavailableclinicalsystem: HEARLabTM.EarHear.2011;32:782---6.
11.VanDunB,CarterL,DillonH.Sensitivityofcorticalauditory evokedpotential(CAEP)detectionforhearing-impairedinfants inresponsetoshortspeechsounds.AudiolRes.2012;2:65---76.
12.CarterL, DillonH, SeymourJ,Seeto M,VanDun B.Cortical auditory-evokedpotentials(CAEPs)inadultsinresponseto fil-teredspeechstimuli.JAmAcadAudiol.2013;24:807---22.
13.ChangHW,DillonH,CarterL,vanDunB,YoungST.The rela-tionship between cortical auditory evoked potential (CAEP) detectionandestimatedaudibilityininfantswithsensorineural hearingloss.IntJAudiol.2012;51:663---70.
14.VanDunB,DillonH,SeetoM.Estimatinghearingthresholdsin hearing-impairedadultsthroughobjectivedetectionofcortical auditoryevokedpotentials.JAmAcadAudiol.2015;26:370---83.
15.Lloyd LL, Kaplan H. Audiometric interpretation: a manual o basic audiometry, 94. Baltimore, MD: UniversityPark Press; 1978.p.16---7.
16.Frizzo ACF, Alves RPC, Colafêmia JF. Potenciais evoca-dos auditivos de longa latência: um estudo comparativo entre os hemisférios cerebrais. Rev Bras Otorrinolaringol. 2001;67:618---25.
17.LightfootGR.TheN1-P2corticalauditoryevokedpotentialin thresholdestimation.Audiologyonline;2010.Availablefrom:
http://www.audiologyonline.com/articles/n1-p2-cortical-auditory-evoked-851(accessed10.10.15).
18.NäätänenR,PictonT.TheN1waveofthehumanelectricand magneticresponsetosound:a reviewand ananalysisofthe componentstructure.Psychophysiology.1987;24:375---425.
19.LightfootGR,KennedyVL.Corticalelectricresponse audiom-etry hearing threshold estimation: accuracy, speed and the effects of stimulus presentation features. Ear Hear. 2006;27:443---56.
20.BeagleyHA,KelloggSE.Acomparisonofevokedresponseand subjectiveauditorythresholds.IntJAudiol.1969;8:345---53.
21.ColesRR,MasonSM.Theresultsofcorticalelectricresponse audiometry in medico-legal investigations. Br J Audiol. 1984;18:71---8.
22.Hoth S. Computer-aided hearing threshold determination from cortical auditory evoked potentials. Scand Audiol. 1993;22:165---77.
23.PrasherD,MulaM,LuxonL.Corticalevokedpotentialcriteriain theobjectiveassessmentofauditorythreshold:acomparison ofnoiseinducedhearinglosswithMénière’sdisease.JLaryngol Otol.1993;107:780---6.
24.RickardsFW,DeVidiS,McMahonDS.Corticalevokedresponse audiometry in noise induced hearing loss claims. Aust J Otolaryngol.1996;2:237---41.
25.TsuB,WongLL,WongEC.Accuracyofcorticalevokedresponse audiometryintheidentificationofnon-organichearingloss.Int JAudiol.2002;41:330---3.
26.TomlinD,RanceG,GraydonK,TsialiosI.Acomparisonof40Hz auditory steady-state response (ASSR) and cortical auditory evokedpotential(CAEP)thresholdsinawakeadultsubjects.Int JAudiol.2006;45:580---8.
27.YeungKNK,WongLLN.Predictionofhearingthresholds: com-parisonofcorticalevokedresponseaudiometry andauditory steady state response audiometry techniques. Int J Audiol. 2007;46:17---25.