www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Effectiveness
of
caudal
septal
extension
graft
application
in
endonasal
septoplasty
夽
Yunus
Karadavut
a,
Ilker
Akyıldız
a,∗,
Hatice
Karadas
¸
a,
Aykut
Erdem
Dinc
¸
b,
Gökc
¸e
Tulacı
a,
Eren
Tastan
aaAnkaraTrainingandResearchHospitalENTClinic,Ankara,Turkey
bBulentEcevitUniversity,ENTClinic,Zonguldak,Turkey
Received8October2015;accepted18January2016 Availableonline20April2016
KEYWORDS Nasalseptum; Nasalcartilage; Nasalobstruction; Intranasalsurgery; Grafting
Abstract
Introduction:Septaldeviationisacommondiseaseseenindailyotorhinolaryngologypractice andseptoplastyisacommonlyperformedsurgicalprocedure.Caudalseptumdeviationisalso achallengingpathologyforear,nose,andthroatspecialists.Manytechniquesaredefinedfor caudalseptaldeviation.
Objective: Toevaluatetheeffectivenessofcaudalseptalextensiongraft(CSEG)applicationin patientswhounderwentendonasalseptoplastyforashortanddeviatednasalseptum.
Methods: Fortypatientswithnasalseptaldeviation,shortnasalseptum,andweaknasaltip supportwhounderwentendonasalseptoplastywithorwithoutCSEGplacementbetweenAugust 2012andJune2013wereenrolledinthisstudy.Twentypatientsunderwentendonasal septo-plastywithCSEGplacement.Therestofthegroup,whorejectedauricularorcostalcartilage harvest for CSEG placement, underwent onlyendonasal septoplasty withoutany additional intervention.UsingtheNasalObstructionSymptomEvaluation(NOSE)andRhinoplastyOutcome Evaluation (ROE)questionnaires,pre-andpost-operativeacousticrhinometermeasurements wereevaluatedtoassesstheeffectofCESGplacementonnasalobstruction.
Results:In thecontrolgroup,preoperative andpostoperative minimalcross-sectionalareas (MCA1)were0.44±0.10cm2and0.60±0.11cm2,respectively(p<0.001).Inthestudygroup,
pre- andpostoperative MCA1values were0.45±0.16cm2 and0.67±0.16cm2,respectively
(p<0.01). In the control group, the nasal cavity volume (VOL1) value was 1.71±0.21mL preoperativelyand1.94±0.17mLpostoperatively(p<0.001).Inthestudygroup,pre-and post-operative VOL1swere 1.72±0.15mLand1.97±0.12mL,respectively(p<0.001).Statistical analysis ofpostoperative MCA1 andVOL1 valuesin thestudy and thecontrol groupscould
夽 Pleasecitethisarticleas:KaradavutY,AkyıldızI,Karadas¸H,Dinc¸AE,TulacıG,TastanE.Effectivenessofcaudalseptalextensiongraft applicationinendonasalseptoplasty.BrazJOtorhinolaryngol.2017;83:59---65.
∗Correspondingauthor.
E-mail:[email protected](I.Akyıldız).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.01.014
notdetectanysignificantintergroupdifference(p=0.093and0.432,respectively).Inthestudy group,meannasolabialangleswere78.15±4.26◦and90.70±2.38◦,respectively(p<0.001).
Conclusion:EndonasalseptoplastywithCESGplacementisaneffectivesurgicalprocedurewith minimalcomplicationrateforsubjectswhohaveadeviated,shortnasalseptumandweaknasal tipsupport.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Septonasal; Cartilagemnasal; Obstruc¸ãonasal; Cirurgiaintranasal; Aplicac¸ãodeenxerto
Eficáciadaaplicac¸ãodeenxertodeextensãoseptalcaudalemseptoplastiaendonasal
Resumo
Introduc¸ão:Desvio septalédoenc¸a comumno cotidianodaprática otorrinolaringológica, e aseptoplastiaéprocedimentocirúrgicocomumenterealizado.Desviocaudaldoseptonasal étambémuma condic¸ão desafiadorapara osotorrinolaringologistas. Sãomuitasastécnicas definidasparadesviocaudaldoseptonasal.
Objetivo:Avaliar a eficácia da aplicac¸ão de enxerto de extensão septalcaudal (EESC) em pacientesquepassaramporseptoplastiaendonasaldevidoaseptonasalcurtoecomdesvio.
Método: Foramrecrutadosparaoestudo,40pacientescomdesviodeseptonasal,septonasal curtoefracasustentac¸ãodapontadonariz,tratadoscomseptoplastiaendonasalcomousem aaplicac¸ão de EESC, entreagosto de 2012e junho de 2013. Ao todo, 20 pacientesforam tratadoscomseptoplastiaendonasalcomaplicac¸ãodeEESC.Orestantedogrupo,querejeitou coleta de cartilagemauricularoucostal paraa aplicac¸ãode EESC,foi tratadoapenas com septoplastiaendonasal,semqualqueroutra intervenc¸ão.Comaaplicac¸ãodosquestionários NOSE(NasalObstructionSymptomEvaluation,Avaliac¸ãodosSintomasdeObstruc¸ãoNasal)e ROE(RhinoplastyOutcomeEvaluation,Avaliac¸ãodosDesfechosdaRinoplastia),asmensurac¸ões préepós-operatóriascomorinômetroacústicoforamobtidascomoobjetivodeavaliaroefeito daaplicac¸ãodeEESCnaobstruc¸ãonasal.
Resultados: Nogrupocontrole,asáreasdesecc¸ãotransversalmínima(ASTM1)antesedepois daoperac¸ãoforam0,44±0,10cm2 e0,60±0,11cm2,respectivamente (p<0,001).Nogrupo
de estudo, os valores antes e depois da operac¸ão para ASTM1 foram 0,45±0,16cm2 e
0,67±0,16cm2,respectivamente (p<0,01).No grupocontrole, o valor para osvolumes da
cavidadenasal(VOL1)foi1,71±0,21mLnopré-operatórioe1,94±0,17mLnopós-operatório (p<0,001).Nogrupodeestudo,osVOL1antesedepoisdaoperac¸ãoforam1,72±0,15mLe 1,97±0,12mL,respectivamente(p<0,001).Aanáliseestatísticadosvalorespós-operatórios para ASTM1e VOL1 nosgrupos de estudo econtrolenão permitiuadetecc¸ão de qualquer diferenc¸a intergrupos(p=0,093 e 0,432,respectivamente).No grupode estudoe nogrupo controle,osângulosnasolabiaismédiosforam78,15±4,26◦ e90,70±2,38◦,respectivamente (p<0,001).
Conclusão:Aseptoplastiaendonasalcomaplicac¸ãodeEESCéumprocedimentocirúrgico efe-tivo,commínimopercentualdecomplicac¸ões parapacientesquese apresentamcomsepto nasalcurtoecomdesvioecomfracasustentac¸ãodapontadonariz.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Septaldeviation of the nose is one of the most common disorders seen in daily otorhinolaryngology practice, and septoplastyisafrequentlyperformedsurgicalprocedureby ear,nose,andthroatspecialists.1Despitethefactthatmany surgicalmethodshavebeendefined,suchasmorselization, cross-hatching incision, partial thickness incision, swing-door flap, and cut-suture technique, no single surgical procedureissuccessfullyapplicableinallconditions.1,2
developed by Byrd et al.3 However, the effectiveness of thistechnique hasnot been extensivelystudied beforein subjects with caudal nasal septal deviation, short nasal septum,andweaknasaltipsupport.
Theaimofthepresentstudywastoevaluatetheefficacy ofCSEG inpatientswhounderwentendonasal septoplasty forashortanddeviatednasalseptum.
Methods
Studydesign
Thestudywasconductedinaccordancewiththeprinciples oftheHelsinkiDeclarationandapprovedbythelocal Institu-tionalReviewBoard(No.0542,date:26/03/2014).Medical recordsof40patientswhounderwentendonasalseptoplasty andCSEGplacement betweenAugust 2012and June2013 wereretrospectivelyreviewed.
Twenty patientsunderwent endonasal septoplastywith CSEG placement (Study Group). The remainder of the patients, who rejected auricular or costal cartilage har-vestfor CSEGplacement,hadonly endonasal septoplasty, withoutanyadditionalinterventionsuchasturbinectomyor turbinoplasty(ControlGroup).
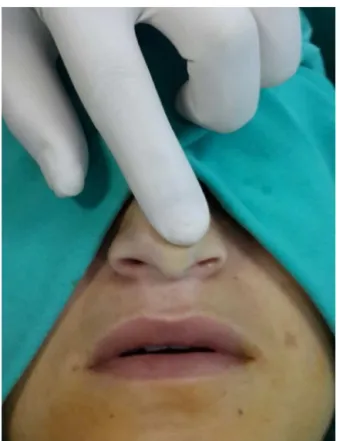
All patients were examined by a physician and a con-sultantbeforethesurgical decision-makingprocess.Nasal tipsupportwasexaminedby recoilmaneuver (Fig.1).All subjectswereevaluatedbyparanasalcomputerized tomo-graphy to reveal potential coexisting nasal or paranasal pathologies.Subjectswhohadmentalretardation, craniofa-cialanomaly,activeinflammatorysinonasaldisease(allergic rhinitis, acute or chronic sinusitis),asthma, dorsal septal deviation, acute nasolabial angle due to long and strong lateral crus, concha bullosa, or septal perforation were excludedfromthestudy.
Outcomeparameters
Allpatients wereevaluatedpre-andpostoperativelywith acousticrhinometerwithandwithout topicalnasal decon-gestant(RhinoMetricsSRE2000,InteracousticsAS---DK.5610, Assens, Denmark) and they were requested to complete theNasalObstructionSymptomEvaluation(NOSE)(Table1) and the Rhinoplasty Outcome Evaluation (ROE) question-naires (Table 2) pre- and postoperatively. Pre-operatively
Figure1 Recoilmaneuver.
andateightpostoperativemonths,minimalcross-sectional areas(MCA1)andvolumes(VOL1)ofthenasalcavitieswere measured with an acoustic rhinometer, before and after topicalnasaldecongestant(0.05%oxymetazoline hydrochlo-ride)application inordertominimizenasalcycle. Inboth groups,pre-andpostoperativeMCA1valuesatthedeviation side(convexside)wereanalyzed.Inboth groupspre-and postoperatively,nasalvolumes(VOL1)ofthedeviationside andthecontralateralsidewerealsoevaluatedbeforeand aftertopicalnasaldecongestiveapplication.
Surgicalprocedure
Surgicalprocedureswereperformedwitheitherlocalor gen-eralanesthesia,withhemitransfixionincisionviaendonasal approach by the same surgeon (K.Y.). All four mucoperi-chondrial/mucoperiostealflapscoveringfourtunnelswere
Table1 NasalObstructionSymptomEvaluation(NOSE)questionnaire.
Notaproblem Mildproblem Moderate problem
Badproblem Severe problem
Nasalcongestionorstuffiness 0 1 2 3 4
Frequencyofnasalcongestion 0 1 2 3 4
Troublebreathingthroughyour nose
0 1 2 3 4
Troublesleeping 0 1 2 3 4
Unabletogetenoughair throughyournoseduring exerciseorexertion
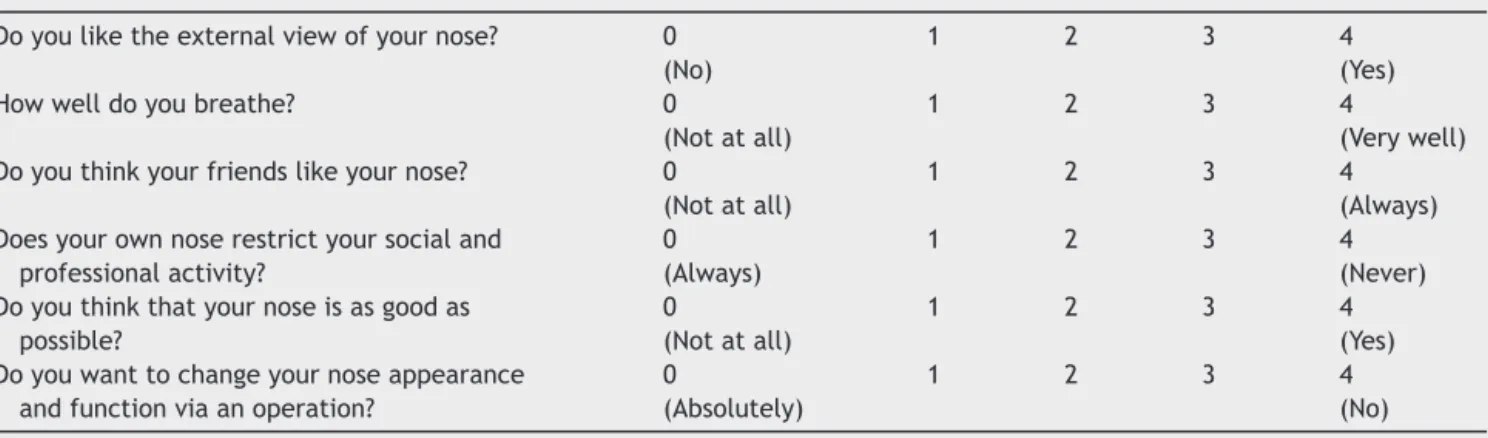
Table2 RhinoplastyOutcomeEvaluation(ROE)questionnaire.
Doyouliketheexternalviewofyournose? 0 (No)
1 2 3 4
(Yes) Howwelldoyoubreathe? 0
(Notatall)
1 2 3 4
(Verywell) Doyouthinkyourfriendslikeyournose? 0
(Notatall)
1 2 3 4
(Always) Doesyourownnoserestrictyoursocialand
professionalactivity?
0 (Always)
1 2 3 4
(Never) Doyouthinkthatyournoseisasgoodas
possible?
0
(Notatall)
1 2 3 4
(Yes) Doyouwanttochangeyournoseappearance
andfunctionviaanoperation?
0
(Absolutely)
1 2 3 4
(No)
elevated toobtain a better surgical view. After resection ofthedeviated partoftheseptalcartilageandbony sep-tum,CSEGharvestedfromtheseptalcartilagewasplacedon thecaudalendoftheseptumbetweenthemedialcruraof thelowerlateralcartilageandstitchedwith4/0long-lasting absorbablemonofilamentmaterial(Monocryl;Figs.2---4).A siliconnasalsplintwasusedfornasalpacking.
Endonasalseptoplastywasalsoperformed bythesame surgeon (K.Y.). After elevating all four mucoperichon-drial/mucoperiostealflaps, thedeviated partof thenasal septum(bonyandcartilage)wasresected.Afterseptoplasty was performed, the mucopercondrial flaps were stitched with 4/0 short-lasting absorbable monofilament material (RapideVicryl);asintheCSEGgroup,asiliconnasalsplint wasusedfornasalpacking.
Figure 2 Application of caudal septal extension graft (CSEG).
Statisticalanalysis
Data were analyzed using SPSS v. 21 (SPSS Inc., Chicago, IL, United States). Agedistribution of thesubjects in the groups wasanalyzed with Student’s t-test and sex distri-butionanalysisutilizedthe chi-squared test.Comparative analysisofaveragescoresforMCA1,VOL1,andtheresults ofthequestionnaireevaluatingnasalobstructionand rhino-plasty outcome as assessedby the NOSE andROE scoring systemswascarriedoutusingtheWilcoxontest. Postopera-tiveaverageMCA1andVOL1valuesinthedifferentgroups wereanalyzed withtheMann---WhitneyUtest. Changes in thenasolabialanglesofthepatientsweremeasuredbased onlateral photographsof the patientsin differentgroups andanalyzed usingStudent’st-testfor dependentgroups. Alldifferencesassociatedwithachanceprobabilityof0.05 orlesswereconsideredtobestatisticallysignificant.
Figure 4 Application of caudal septal extension graft (CSEG).
Results
The Study Group included 20 patients (15 males, five females)withameanageof31.7±8.8years(range,23---40) andtheControlGroupincluded20patients(12males,eight females)withameanageof34.7±8.3years(range,26---43). Bothgroupsdidnotdifferfromeachotherregardingageand gender(p=0.500andp=0.281,respectively).
Postoperative MCA1 values were better than preoper-ative MCA1 values at the deviation (convex) side in both groups (p<0.001),without anystatistically significant dif-ferencebetweenStudyandControlGroups(p=0.093;Fig. 5).Inbothgroups,VOL1valueswerebetteratthedeviation sideafterdecongestionandsurgery(p<0.001)withoutany significantdifferencebetweengroups(p=0.432;Fig.6).
In both groups, postoperative NOSE scale scores were better than preoperative scores (p<0.001). Postoperative
Control group CSEG group
I-Concave side, preoperative, pre topical decongestant.
I-Concave side, preoperative, post topical decongestant.
I-Concave side, postoperative, pre topical decongestant.
I-Concave side, postoperative, post topical decongestant.
I-Convex side, preoperative, pre topical decongestant.
I-Convex side, preoperative, post topical decongestant.
I-Convex side, postoperative, pre topical decongestant.
I-Convex side, postoperative, post topical decongestant.
1.2
1.0
0.8
MCA
(Ort.
±
SS
)
0.6
0.4
0.2
Figure5 Averageminimalcross-sectionarea(MCA1) values ofthestudyandcontrolgroup.
resultswerebetterintheStudyGroupwhencomparedwith theControlGroup(p<0.001)(Table3).Inthefirst,fourth, fifth,andsixthquestions,postoperativeresultswere statis-ticallysignificantlybetterthanthepreoperativeonesinboth theStudyandControlGroups(p=0.049,p=0.001,p=0.001, andp=0.038,respectively;Table4).
Postoperativenasolabial anglevaluesweresignificantly better than the preoperative values in the study group (p<0.001;Table5).
Postoperative MCA1 values were better than preoper-ative MCA1 valuesat the deviation (convex) side in both groups (p<0.001), without any (statistically) significant differencebetweentheStudyandControlGroups(p=0.093;
Fig. 5). In both groups, VOL1 values were better at the deviation side after decongestion and surgery (p<0.001),
Table3 NasalObstructionSymptomEvaluationquestionnaireresultsofthecontrolandstudygroup.
Control CSEG Control-studycomparison
Preop. Postop. p Preop. Postop. p Preop. Postop.
Control group CSEG group
I-concave side, preoperative, pre topical decongestant.
I-concave side, preoperative, post topical decongestant.
I-concave side, postoperative, pre topical decongestant.
I-concave side, postoperative, post topical decongestant.
I-convex side, preoperative, pre topical decongestant.
I-convex side, preoperative, post topical decongestant.
I-convex side, postoperative, pre topical decongestant.
I-convex side, postoperative, post topical decongestant.
Vol1(ort.
±
SS)
2.50
2.25
2.00
1.75
1.50
Figure6 Averagenasalcavity volume(VOL1) valuesofthe
studyandcontrolgroup.
without any statistically significant difference between groups(p=0.432;Fig.6).
Discussion
Caudalseptaldeviationsarefrequentlyencountered, chal-lengingpathologiesofthenose.Patientswithcaudalseptal
deviation,shortnasalseptum,andweaknasaltipsupport suffer fromnasal obstruction becauseof deterioration of nasalairflowduetoacutenasolabialangle.
Patients with acute nasolabial angle also suffer from abnormalshapeofthenosebecauseofunsatisfactorynasal tipprojection.1,2,4
Satisfactory nasal tip support may be achieved with columellar strutimplantsplaced via external approach in patientswhohaveshortnasalsepta.However,inthe pres-enceofcaudalseptaldeviationassociatedwithshortnasal septum,implantationofcolumellarstrutalonemaybe insuf-ficient.CSEGmaybeusedtostrengthenthenasaltipand correctthecaudalseptaldeviationviaendonasalincision.
Septalcartilageisagoodsource ofCSEG,butauricular orcostalcartilagesmaybealternativesourcesifseptal car-tilageisinsufficientandthepatientconsentstoadditional incisionforharvesting. Sinceauricularcartilage iselastic, septaland costalcartilagesareconsidered tobe superior for preparationof CSEG.In the present study,septal car-tilage waspreferredasfirstline source sinceit is easyto harvest.
Externalapproachviatrans-columellarincisionmayalso beusedforCSEG.Inthepresentstudy,theauthorspreferred endonasal hemitransfixion incision because of its shorter operation time,lesserexternal scar tissue,lowerrates of flap-relatedcomplications,andfasterhealingprocess. Long-lastingabsorbablesuturematerialinsteadofnon-absorbable material was preferred to avoid extrusion of the suture materialoutofthenasalvestibularskin.Mattressstitches wereusedtoinordertoobtainamorestablenasaltipand tocorrectthecaudaldeviationofthenasalseptum.
PostoperativeMCA1and VOL1valueswere significantly betterthanthepreoperative valuesinboth thestudyand thecontrolgroups(p<0.05).However,postoperativeMCA1 andVOL1valuesweresignificantlybetterinboththestudy andthe controlgroups, without anysignificant intergroup difference(p>0.05).
NOSEandROEscalescoreswerebetterinthe postopera-tiveperiodinboththestudyandcontrolgroups(p<0.05).
Significantly better outcomes were achieved in both groups, notonlyin laboratory evaluation(MCA1 andVOL1 measurement),butalsoinclinicalevaluation(NOSEandROE questionnaire), which indicated that classical septoplasty maybealsoaneffectivesurgicalprocedure inashortand deviatednasalseptum.
However,accordingtotheseresults,patientswhohave ashort,caudalseptaldeviationandseekamoreprojected
Table4 RhinoplastyOutcomeEvaluation(ROE)questionnaireresultsofthegroups.
Control CSEG Control-Studycomparison
Preop. Postop. p Preop. Postop. p Preop. Postop.
Table5 Nasolabialanglesofthestudyandcontrolgroup.
Preop. Postop. p
Nasolabialangleofthestudygroup(NLA) 78.15±4.246 90.70±2.386 <0.001 Nasolabialangleofthecontrolgroup 76.254±3.954 76.853±4.025 >0.001
nasaltiparegoodcandidatesfor endoscopicimplantation ofCSEG.
Conclusion
CSEGisaneffective andsimple surgicalprocedureto cor-rectcaudalseptaldeviationsandstrengthen thenasaltip support. However, ifa patient witha caudal septal devi-ation desiresto have better tipprojection, CSEGmay be a good alternative. Only endonasal septoplasty results in similarfunctionaloutcomes,andanadditionalendoscopic CSEGimplantationdoesnotimproveMCA1,VOL1,andNOSE scores.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgment
TheEnglishinthisdocumenthasbeencheckedbyatleast twoprofessionaleditors,bothnativespeakersofEnglish.
References
1.WeeJH, LeeJE, Cho SW, JinHR. Septal battengraft to cor-rect cartilaginous deformities in endonasal septoplasty. Arch OtolaryngolHeadNeckSurg.2012;13:457---61.
2.Kim JH, Kim DY, Jang YJ. Outcomes after endonasal septo-plastyusingcaudalseptalbattengrafting.AmJRhinolAllergy. 2011;25:66---70.
3.Byrd HS, Andochick S, Copit S. Septal extension grafts: a methodofcontrollingtipprojectionshape.PlastReconstrSurg. 1997;100:999---1010.