SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Comparative
study
between
lateral
decubitus
and
traction
table
for
treatment
of
pertrochanteric
fractures
with
cephalomedullary
nails
夽
Eric
Fernando
de
Souza
∗,
José
Octávio
Soares
Hungria,
Lucas
Romano
Sampaio
Rezende,
Davi
Gabriel
Bellan,
Jonas
Aparecido
Borracini
HospitalMunicipaldoCampoLimpoDr.FernandoMauroPiresdaRocha,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP, Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11November2015 Accepted18April2016
Availableonline14December2016
Keywords: Bonenails Bonescrews Femuralfractures
a
b
s
t
r
a
c
t
Objective:Toperformaretrospectiveradiographicassessmentofthereductionandimplant position in the femoral head in patients with pertrochanteric fractures treated with cephalomedullarynailinginthelateralpositionversustractiontable.
Methods:Radiographsofpatientswithpertrochantericfractureofthefemurtreatedwith cephalomedullarynailinginthelateralpositionandtractiontablewereretrospectively eval-uated.Fortheevaluationweusedtheanteroposteriorradiographicviewofthepelvisandthe lateralviewoftheaffectedside.Thecervicodiaphysealangle,thetip-apexdistance(TAD), andthespatialpositionofthecephaliccomponentintheheadweremeasured.Twopatient groupswerecreated,onegroupoperatedonthetractiontableandanothergroupoperated inthelateralposition.
Results:Regardingthe cervicodiaphysealangleobservedinthetractiontablegroup,the resultsof11patients(61.1%)wereoutsidetheacceptableparametersproposedinthepresent study.BothgroupswereequivalentregardingTADandthepositionofthecephalic compo-nentinthehead.
Conclusion:Adifferenceinthecervicodiaphysealanglewasobserved;thegroupoperatedon thetractiontablehad11patients(61.1%)whosemeasurementswereoutsidetheacceptable parameters.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheHospitalMunicipaldoCampoLimpoDr.FernandoMauroPiresdaRocha,DepartamentodeOrtopediae Traumatologia,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](E.F.Souza). http://dx.doi.org/10.1016/j.rboe.2016.04.009
Estudo
comparativo
entre
decúbito
lateral
e
mesa
de
trac¸ão
para
tratamento
de
fraturas
pertrocantéricas
com
hastes
cefalomedulares
Palavras-chave: Pinosortopédicos Parafusosósseos Fraturasdefêmur
r
e
s
u
m
o
Objetivo: Fazerumaavaliac¸ãocomparativaradiográficaretrospectivadareduc¸ãoeposic¸ão doimplantenacabec¸afemoralempacientescomfraturaspertrocantéricastratadoscom hastecefalomedularemdecúbitolateralouemmesadetrac¸ão.
Métodos: Foramavaliadasretrospectivamenteradiografiasdepacientescomdiagnósticode fraturapertrocantéricadofêmurtratadoscomhastecefalomedularemdecúbitolateralou emmesadetrac¸ão.Paraavaliac¸ãoradiográficaambulatorialusamosasincidências antero-posteriordapelveeoperfildoladoafetado.Aferimosoângulocervicodiafisário,atip-apex distance(TAD)eaposic¸ãoespacialdoelementocefáliconacabec¸a.Foramcriadosdoisgrupos depacientes,umoperadonamesadetrac¸ãoeoutroemdecúbitolateral.
Resultados:Comrelac¸ ¯aoaoângulocervicodiafisário,observamosnogrupodamesadetrac¸ão 11pacientes(61,1%)foradosparâmetrosaceitáveispropostosemnossotrabalho.ParaaTAD eaposic¸ãodoelementocefáliconacabec¸a,osdoisgrupossemostraramequivalentes. Conclusão: Observamosdiferenc¸acomrelac¸ãoaoângulocervicodiafisário,noqualogrupo operadoemmesadetrac¸ãoapresentou11pacientes(61,1%)foradosparâmetrosaceitáveis. ©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Pertrochantericfracturesarecommonintheelderly,dueto osteoporosis,andtheirincidencehasincreasedsignificantly becauseofthelongerlifeexpectancyofthepopulation.Their incidenceisexpectedtodoubleinthenext25years.1,2
Cur-rently,thereisaconsensusthatpertrochantericfracturesof thefemurshouldbetreatedsurgically.3,4Thetechniquesfor
fixationofthese fractureswith cephalomedullarynails are bestconductedwithatractiontable.However,intheabsence orimpossibilityofits use, it isnecessarytoadoptanother position,suchaslateraldecubitus.5Inanearlierstudy
con-ductedinthepresenthospitalbydeOliveiraetal.,6conditions
thatcouldinfluencetheefficiencyofthe reductionandthe positioningofthecephalic elementinthe femoralhead in pertrochantericfractures,whenfixatedinlateral decubitus, wereassessed.Giventheencouragingresultsofthatstudy,6
thepresentauthorsconductedacomparativestudytoassess theresultsregardingthereductionandthespatialpositioning ofthecephalicelement(CE)inthefemoralhead (cervicodia-physealangle),tip-apexdistance(TAD),andspatialpositionof theCEinthefemoralhead(circleofBaumgaertneretal.7)in
pertrochantericfracturestreatedonatractiontable.Thegoal wastoassesswhetherthereductionandpositioningofthe cephalicelementinbothpositioningmethodswere equiva-lent.
Thepresent study aimedtoevaluate whetherthere are differencesinthequalityofreductionandinthespatial posi-tioningoftheCEofcephalomedullarynailsinpertrochanteric fracturestreatedwiththesenailsinlateraldecubitusandon atractiontable.
Patients
and
methods
Patients
Between January 2014 and June 2015, 35 patients diag-nosed with pertrochanteric femoral fracture were treated withcephalomedullarynailonatractiontableinateaching hospitalinalargeurbancenter.Ofthose,18attendedthe ret-rospectivefinalassessment,14couldnotbelocated,andthree died,oneinthehospitalandtwopostoperatively.Five(27.8%) werefemaleand13(72.2%)weremale,withameanageof65 years(range41–91years).Regardingthetraumamechanism, tenhadaground-levelfall;two,afallfrombed;two,afallfrom stairs;onehadsufferedabeating;one,afallfromtheroof; one,amotorcycleaccident;andone,afractureaftertheuseof ReamerIrrigatorAspiration®(RIA).Fivepatientshadfracture oftheleftsideand13,ontherightside.Twenty-ninefractures treatedinthe lateraldecubituspositionbetweenJune2012 andNovember2013wereassessed.Ofthose,19attendedthe retrospectivefinalassessment,eightcouldnotbelocated,and twodiedinthehospital,duetopostoperativetrauma compli-cations;11werefemaleand eightmale,mean age60years (range18–87years).Themechanismsoftraumawere ground-levelfallsin13patients;motorcyclefalls,infour;injuryby firearm,inone;andbicyclefall,inone.Elevenpatients pre-sentedfractureoftheleftsideandeightontheright.6
Ofthepreoperativeradiographsanalyzedfrom Group2, six(33.3%)patientspresentedtheA1pattern;seven(38.9%), A2;andfive(27.8%),A3.Theminimumtimeofpostoperative evaluationforthatgroupwasonemonth.Inturn,inGroup 1one(5.3%)patientpresentedtheA1pattern,11(57.9%),A2; andseven(36.8%),A3.Theminimumtimeofpostoperative evaluationforthatgroupwassixmonths.
Methods
Toclassifythefractures,authorsusedpelvicradiographsof theaffectedhipinanteroposterior(AP)andlateral(L)views, andappliedtheAOratingforpertrochantericfractures (31-):A1aresimple,two-partfractureswithgoodbonesupport inthemedialcortical;A2are multifragmentaryfracturesin whichthemedialanddorsalcortices(lessertrochanter)are brokenondifferentlevels,butthelateralcortexisintact;in A3fractures,thelateralcortexisalsobroken(reverseoblique fractures).8
To perform the surgical procedure on a traction table, patientwasplacedundergeneralorspinalanesthesiainthe supinepositioninanorthopedicsurgicaltablewithmounted traction boots, properly positioned; the non-fractured limb wasplacedinaflexedandabductedpositiontoprovidemore roomforthe C-arm. Closedreductionofthe fracture, with tractionandinternalorexternalrotation,dependingonthe fracturepattern,wasconfirmedbyradioscopy.Then,surgical sitewaspreppedfromtheiliaccresttothefootoftheaffected side.Cephalomedullarynails(GammaTMnail®orTFN®)were
used,adoptingthestandardtechniqueforinternalfixationof fractures.9Fortheproximalfixation,itwassoughttoposition
thecephalicfixationelement onthecenterofthehead, at 1-cmfromthesubchondralboneinnormalboneandat 0.5-cminporoticboneinAPandL.Distalfixationwasperformed withaguidewhenastandard-sizecephalomedullarynailwas used,orfreehandwhenalongnailwasused.Radioscopic con-trolwasperformedinbothAPandLateverystep.Allcases wereoperatedbyathirdyearresident,overseenbythesame attendingphysician.
Inthegroupinwhichosteosynthesiswasperformedinthe lateralposition, patientwasplacedinthe lateraldecubitus positionwiththeaidofcushionsonthebackandabdomen;AP andLradiographsweremadetoassessthecorrect visualiza-tionoftheentirefemurandpelvisintwoplanes,asdescribed byOliveiraetal.6
Foroutpatientradiographicevaluation,theAPviewofthe pelviswasused,withthepatientinthesupineposition;the incidentraywaspositionedonthemidlineofthepubic sym-physis,withthefeet internallyrotatedat15◦–20◦ usingthe standardtechnique.TheLviewwasalsoused,withthepatient positionedinsupine,theaffectedhipat45◦flexionand20◦ abduction,and the incident ray was centered verticallyon thehipjoint,followingthestandardtechnique.10 For these
incidences,thefollowingvariableswereevaluated:
Cervicodiaphysealangle:anglebetweentwolines,onethat crossesthecenterofrotationofthefemoralheadandthe longitudinalaxisofthefemoralneckandtheother,thelong axisofthefemoralshaft.11 Valuesbetween130◦ and135◦ wereconsideredasnormal.
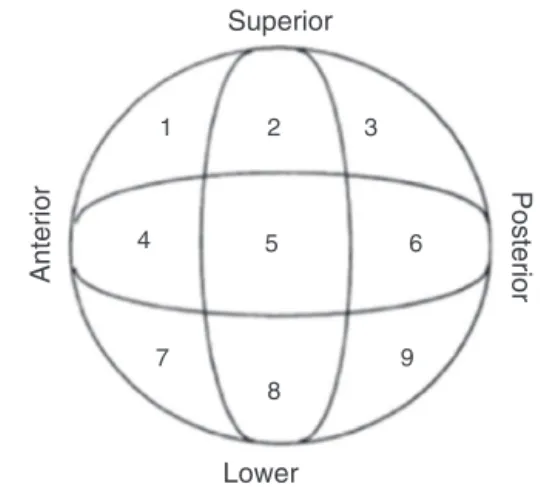
Anterior
Superior
Lower
1 2 3
6 5
4
7
8
9
Posterior
Fig.1–Arrangementofthequadrantsinninezones.
TAD:definedinaccordancewithBaumgaertneretal.7;
dis-tancesshorterthan25mmfromthesubchondralboneinthe centralportionofthefemoralheadtotheendofthecephalic pinofthenailareideal.
SpatialpositionoftheCEinrelationtothehead:thefemoral headisdividedintonineseparateareasinwhichtheCEis located.Theseare:superior-,middle-,andlower-thirdinthe APradiographandanterior-,center-,andposterior-thirdin theLradiograph.7Thecentral-centralzoneinquadrant5was
consideredideal(Fig.1),andquadrantswithincreasedrisk ofcut-outwereavoided.
Twogroupsofpatientswerecreated,separatedbythe posi-tioningandreductionmethodusedinthesurgicaltreatment offractures.Tocomparethem,threeparameterswereused: cervicodiaphysealangle,TAD,andspatialpositionoftheCE. Thequantitativecharacteristicsofthegroupsweredescribed as mean, standard deviation, median, and minimum and maximum,andcomparedwithStudent’st-test.The qualita-tivecharacteristicsofthegroupsweredescribedbyabsolute andrelativefrequencies;theassociationsbetweenthegroups wereverifiedusingthechi-squaredtest,Fisher’sexacttest,or thelikelihoodratios.12
A5%significancelevelwasadopted.
Results
Thedatacollectedfrombothgroupsweretabulated.Patient characteristics,suchasage,sex,weight,andheight,were cho-senforanalysis.Fracturecharacteristicsanalyzedwereside, AOclassification,andmechanismofinjury,asdescribedin Table1.
Table1showsthatpatientsoperatedinthelateral decu-bitus position and on the traction table showed similar characteristics(p>0.05).
Similarly, toassessthe resultsofsurgerybythe criteria setforthinthepresentstudy,theresultsofbothgroupswere organizedanddescribedinTable2.
Table1–Descriptionofthepersonalcharacteristicsandtheprocedurebygroupsandresultsofstatisticaltests.
Variable Group Total(n=37) p
Lateraldecubitus(n=19) Tractiontable(n=18)
Sex,n(%) 0.65
Female 11(57.9) 5(27.8) 16(43.2)
Male 8(42.1) 13(72.2) 21(56.8)
Age(years) 0.340a
Mean(SD) 60(20.9) 65.9(16.4) 62.9(18.8)
Median 64(18;87) 64(41;91) 64(18;91)
Weight(kg) 0.788a
Mean(SD) 68.2(21.4) 66.6(11.7) 67.4(17.2)
Median 67.8(40;121) 67(50;90) 67.8(40;121)
Height(m) 0.433a
Mean(SD) 1.62(0.11) 1.65(0.07) 1.64(0.09)
Median 1.62(1.45;1.85) 1.65(1.55;1.79) 1.65(1.45;1.85)
Side,n(%) 0.65
Right 8(42.1) 13(72.2) 21(56.8)
Left 11(57.9) 5(27.8) 16(43.2)
Classification,n(%) 0.076b
A1 1(5.3) 6(33.3) 7(18.9)
A2 11(57.9) 7(38.9) 18(48.6)
A3 7(36.8) 5(27.8) 12(32.4)
Traumamechanism,n(%) 0.420
Ground-levelfall 13(68.4) 10(55.6) 23(62.2)
Others 6(31.6) 8(44.4) 14(37.8)
Chi-squaredtest.
a Student’st-test. b Likelihoodratiotest.
Table2–Descriptionofthesurgicalevaluationcriteriaaccordingtogroupsandresultsofstatisticaltests.
Variable Group Total(n=37) p
Lateraldecubitus(n=19) Tractiontable(n=18)
Positionofcephalicimplant,n(%) 0.823
Quadrant5 7(36.8) 6(33.3) 13(35.1)
Otherquadrants 12(63.2) 12(66.7) 24(64.9)
TAD,n(%) 0.660a
Normal 17(89.5) 15(83.3) 32(86.5)
Altered 2(10.5) 3(16.7) 5(13.5)
Cervicodiaphyseal,n(%) <0.001
Normal 18(94.7) 7(38.9) 25(67.6)
Altered 1(5.3) 11(61.1) 12(32.4)
Chi-squaredtest.
a Fisher’sexacttest.
performedinthe lateraldecubitus position(p<0.001).Both groupsweresimilarregardingTADandimplantpositioning.
Discussion
Therearesomeoptionsforreductionandpatientpositioning inthetreatmentofpertrochantericfractures.13 Thepresent
hospitaldidnotusetohaveatractiontable,sopatientswere treatedinthelateralposition,amethodthatwasshownto beeffectiveinthisserviceregardingspatialpositioningofthe
CE,TAD,andcervicodiaphysealangle.Thehospitalnowhas atractiontable,andithasbecomethemethodofchoicefor thetreatmentofthesefractures.Therefore,most profession-alshavestartedtoperformthistypeofosteosynthesisinthe present hospital,asthe methodiswidelydescribedamong orthopedic surgeons and the procedure requires a smaller team.Incontrast,thelateraldecubituspositioningisamore meticuloustechniquethatrequiresexperienceandexpertise onthepartofthesurgeonandalarger,trainedteam.
lateraldecubitustechnique,thisiscontrolledbythesurgeons themselves,whocanhavemoreprecisecontrolofthe reduc-tionateachstageofosteosynthesis.Withthetractiontable, thisadjustmentismadeattheinitialpositionandisdifficultto makeinotherstagesofosteosynthesis,asthefineadjustment ismadewithanon-steriledevice.
Consideringbothgroupsofpatients(one treatedonthe tractiontableandtheotherinlateraldecubitus),theresultsof bothmethodswereassessed,aimingtoreconstructthe nor-malcervicodiaphysealanglebetween130◦ and135◦,sothat theimplantcouldbeproperlypositioned,avoidingreductions invarus.14,15Fortheproximalfixation,itwassoughtto
posi-tionthecephalicfixationelementonthecenterofthehead, inAPandLat1-cmfromthe subchondralboneinnormal boneand at 0.5-cminporotic bone, followingthe concept introducedbyBaumgaertneretal.7
Inbothgroups,theparametersweresuccessfullyachieved. RegardingtheTAD(describedforosteosynthesiswithdynamic hipscrews,itcan beusedtoassessthecorrectpositioning ofcephalomedullarynails)15,16andthespatialpositionofthe
cephalicfixationelement,thesafestquadrantswerealways obtained,avoidingthosewithhighercutoutrisk.5,7
Asforthecervicodiaphysealangle,unsatisfactoryresults were observedin thecases operatedon the tractiontable; 61.1%ofcasesdidnotfallwithinthestipulatedstandard.In thepatientsoperatedinlateraldecubitus,onlyone(5.3%)was foundtobe outside the acceptedstandards inthe present study.
Conclusion
Astatisticallysignificant differencewasobservedregarding thecervicodiaphysealangle(p-value<0.001);thegroup oper-atedonthetractiontablepresented11patients(61.1%)outside theacceptableparameters.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. HaidukewychGJ.Intertrochantericfractures:tentipsto improveresults.JBoneJointSurgAm.2009;91(3):712–9.
2.UlianaCS,AbaggeM,MalafaiaO,KalilFilhoFA,CunhaLAM. Fraturastranstrocantéricas–Avaliac¸ãodosdadosda admissãoàaltahospitalar.RevBrasOrtop.2014;49(2): 121–8.
3.ButlerM,ForteML,JoglekarSB,SwiontkowskiMF,KaneRL. Evidencesummary:systematicreviewofsurgicaltreatments forgeriatrichipfractures.JBoneJointSurgAm.
2011;93(12):1104–15.
4.CantoRS,SakakiM,SusukiI,TucciP,BelangeroW,KfuriMJr, etal.Fraturatranstrocanteriana.SãoPaulo:Sociedade BrasileiradeOrtopediaeTraumatologia;2007.Projeto Diretrizes.
5.BucholzRW,Court-BrownCM,TornettaP3rd.Fraturasem adultosdeRockwoodeGreen.7aed.Barueri:Manole;2013. 6.deOliveiraEJ,HungriaJO,BellanDG,BorraciniJA.Decúbito lateralparatratamentodasfraturaspertrocantéricacom hastescefalomedulares.RevBrasOrtop.2015;40(4): 409–15.
7.BaumgaertnerMR,CurtinSL,LindskogDM,KeggiJM.The valueofthetip-apexdistanceinpredictingfailureoffixation ofperitrochantericfracturesofthehip.JBoneJointSurgAm. 1995;77(7):1058–64.
8.RüediTP.PrincípiosAOdotratamentodefraturas.2a
ed.Porto Alegre:Artmed;2009.
9.CanaleST.Campbell’soperativeorthopaedics.12thed.St. Louis:Mosby;2013.
10.PoleselloGC,NakaoTS,QueirozMC,DaniachiD,RicioliWJr, GuimarãesRP,etal.Propostadepadronizac¸ãodoestudo radiográficodoquadriledapelve.RevBrasOrtop. 2011;46(6):634–42.
11.GiordanoV,DiasMC,SantosGF,CabralS,AmaralNP, AlbuquerqueRP.Estudoradiográficodaextremidade proximaldofêmurparaavaliac¸ãodoriscodefratura osteoporótica.RevBrasOrtop.2007;42(4):88–96.
12.KirkwoodBR,SterneJA.Essentialmedicalstatistics.2nded. Massachusetts,USA:BlackwellScience;2006.
13.OzsoyMH,BasarirK,BayramogluA,ErdemliB,TuccarE, EksiogluMF.Riskofsuperiorglutealnerveandgluteus mediusmuscleinjuryduringfemoralnailinsertion.JBone JointSurgAm.2007;89(4):829–34.
14.GuimarãesJA,GuimarãesAC,FrancoJS.Avaliac¸ãodo empregodahastefemoralcurtanafraturatrocantérica instáveldofêmur.RevBrasOrtop.2008;43(9):
406–7.
15.BorgerRM,LeiteFA,AraújoRP,PereiraTF,QueirozRD. Avaliac¸ãoprospectivadaevoluc¸ãoclínica,radiográficae funcionaldotratamentodasfraturastrocantéricasinstáveis dofêmurcomhastecefalomedular.RevBrasOrtop. 2011;46(4):380–9.