SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
A
comparison
study
of
radiographic
and
computerized
tomographic
angles
in
slipped
capital
femoral
epiphysis
夽
Iberê
Pereira
Datti
∗,
Bruno
Sérgio
Ferreira
Massa,
Leandro
Ejnisman,
Nei
Botter
Montenegro,
Roberto
Guarniero,
Kodi
Edson
Kojima
UniversidadedeSãoPaulo,FaculdadedeMedicina,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19June2016 Accepted26July2016
Availableonline30August2017
Keywords:
Slippedcapitalfemoral epiphyses/radiography X-raycomputedtomography Hipjoint/radiography
a
b
s
t
r
a
c
t
Objective:To compareproximalfemur radiologicangles inpatientswith slippedcapital femoralepiphysisandtoanalyzewhethercomputerizedtomographymaymodifythe treat-ment.
Methods:Cross-sectionalstudycomparingandanalyzingthesimilaritybetweenanglesand radiologicclassificationofinterestinslippedcapitalfemoralepiphysis(SCFE).
Results:Itwasobservedthatthetherapeuticmanagementinslippedcapitalfemoral epiph-ysismightbemodifieddependingontheclassificationandradiologicacquisitionmethod adopted.
Conclusion:Multiplanarassessmentofproximalfemoraldeformityinpatientswithslipped capitalfemoralepiphysisisaviableoption,withthepotentialtomodifythedisease classi-ficationand,consequently,thetherapeuticmanagement.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Estudo
comparativo
dos
ângulos
radiográficos
e
tomográficos
na
epifisiolistese
do
fêmur
proximal
Palavras-chave:
Escorregamentodasepífises proximaisdofêmur/radiografia Tomografiacomputadorizadapor raiosX
Articulac¸ãodoquadril/radiografia
r
e
s
u
m
o
Objetivo:Compararângulosradiológicosdofêmurproximalempacientescom escorrega-mento proximal da cabec¸a do fêmur (EPCF) e analisar se a avaliac¸ão por tomografia computadorizadapodemodificaraconduta.
Método:Estudo transversal que comparou e analisou a concordância entre ângulos e classificac¸õesradiológicasdeinteressenoescorregamentoproximaldacabec¸adofêmur (EPCF).
夽
PaperdevelopedatUniversidadedeSãoPaulo,FaculdadedeMedicina,HospitaldasClínicas,DepartamentodeOrtopediae Trauma-tologia,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](I.P.Datti).
http://dx.doi.org/10.1016/j.rboe.2017.08.011
Resultado: Observou-sequeacondutaterapêuticanaEPCFpodesermodificadaadepender daclassificac¸ãoadotadaedométododeaquisic¸ãodeimagensradiológicas.
Conclusão: Aavaliac¸ãomultiplanardadeformidadedofêmurproximalempacientescom escorregamentoproximaldacabec¸adofêmuréumaopc¸ãoviávelecompotencialde mod-ificaraclassificac¸ãodadoenc¸anospacientese,porconseguinte,amodalidadeterapêutica. ©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Slippedcapitalfemoralepiphyses(SCFE)isthemostprevalent hipdiseaseinadolescence.1Itischaracterizedbya disturb-ancein the physis, causing anterior slipping and external rotationofthefemoralneckinrelationtothefemoralhead, which remains in the acetabulum.2 The etiology is multi-factorial,withobesitybeingconsideredthemainetiological factor.1,3
Earlydiagnosisandappropriatetreatmentmayreducethe incidenceofcomplicationsand functionalloss.4–11 Imaging testsareindispensabletoconfirmthediagnosisandclassify thedisease.Anteroposteriorhip X-rayand Lauenstein-type profileX-rayareusuallysufficientfordiagnosticconfirmation andclassification.Computedtomography(CT)andmagnetic resonanceimaging(MRI)areusefulinseverecasesto deter-mine physisclosure, angular andtorsional deviations, and indicationofosteotomies.12,13
Mild cases are treated by the in situ percutaneous fixation technique with a cannulated screw.14 However, recent literature has favored more aggressive treatment measures. Moderate and severe slipping can be treated with several techniques, such as slipping reduction fol-lowedbyfixation,orcorrectiveosteotomiesintheproximal femur.15–19
Thetherapeuticmanagementdependsontheradiological classificationoftheseverityofthedisease.Important radio-logical ratings include the Southwick16 slip angle and the head–neckangledescribedbyCohenetal.20Cooperetal.21 recentlydemonstratedthatthethree-dimensionaldeformity causedbySCFEcanbebetterdeterminedwiththeevaluation ofthedeformityintheoblique plane.Anoptionalmethod, whichconsiderstheslippercentagebetweenthefemurhead andneck,wasproposedbyWilson,22moreindicatedforsmall deviations.
The authors’ clinical experience is in accordance with the findings by Monazzam et al.13 and Tins et al.,12 whodescribedthatbiplanarradiographsunderestimatethe severity of SCFE when compared to CT. Richolt et al.23 suggestthattheradiographicevaluationoverestimates angu-lardeviationsandunderestimatestorsionaldeviations.The hypothesis of the present study is that the evaluation of SCFE through CT may alter the slip classification and interfere with therapy. Our objective was to compare the angles obtained by the plain X-ray and CT, and to evalu-atewhetherCTwouldalterthetherapeuticmanagementin SCFE.
Material
and
methods
Afterapprovalbythe ethicscouncil, aretrospectivesurvey was performed of patients who were diagnosedas having high SCFE (ICD M93) between January2011 and May 2014. Duringthis period,itbecameroutinetoorderatour medi-calfacilitypreoperativeCTandX-rayforpatientsadmitted withthediagnostichypothesisofSCFE,candidatesforDunn osteotomy.Next,theradiologicalimagesstoredinthe hospi-talimagesystemweresurveyed.Patientswhodidnothavea CTorX-rayavailableinthesystemwereexcluded. Measure-mentsoftheanglesofinterestweretakenbyanorthopedic hipspecialist,blindedtothepatient’sidentificationand clin-icaldata.Radiographicandtomographicmeasurementswere takenseparately.
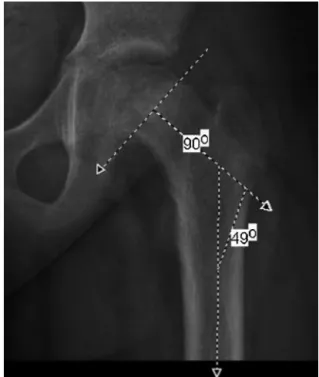
Southwickangle(femoralhead-diaphysisangle–HDA)
The Southwick angle is measured between a perpendicu-larline ofthe line tangenttothe proximalfemoralphysis superiorly and inferiorly and the anatomical axis of the femoraldiaphysis16(Fig.1).FormeasuringtheFHDAinthe tomographic images we adopted the method proposed by Southwickthathasasstandardthecoronalandsagittal sec-tions, perpendicularto eachother. Toevaluatethe coronal plane,thesectionwiththelargestsubtrochantericdiameter wastakenasthereferenceimage,andtwosectionsoftheCT weresuperimposedtoevaluatethesagittalplane,onewiththe largest physisdiameterand theotherwiththelargest sub-trochantericdiameter (Fig. 2). Afterobtainingtheanglesin bothplanes,thethree-dimensionaldeviationofthefemoral diaphysisinrelationtothefemoralheadwasestimatedby trigonometry24(Fig.3).
Cooper’sobliqueplane(femoralhead–neckangle–FHNA)
Fig.1–SouthwickangleonAPX-ray.
Fig.2–Southwickangle(femoralhead-shaftangle–FHSA) throughtheCTsagittalplane.
a) FHSA - 3D = tan-1 Ö tan2 FHSA coronal plane + tan2 FHSA sagital plane
b) FHNA - 3D = tan-1 Ö tan2 FHNA coronal plane + tan2 FHNA axial plane
c) WHNS = 1 - (WHNS axial plane x WHNS coronal plane)
Fig.3–(a)Trigonometricformulatodetermine three-dimensionalfemoralhead–shaftangle;(b) trigonometricformulatodeterminethree-dimensional femoralhead–neckangle;(c)trigonometricformulato determinethree-dimensionalWilson’shead–neckslip.
Fig.4–Femoralhead–neckangle(FHNA)throughaCT coronalsection.
measurement inthecoronalsectionistheonewiththelargest femoral neckarea.Afterobtainingthe uniplanar measure-ments,thethree-dimensionaldeviationwasdeterminedby trigonometricmeans(Fig.3b).
Wilson’shead–neckslip(WHNS)
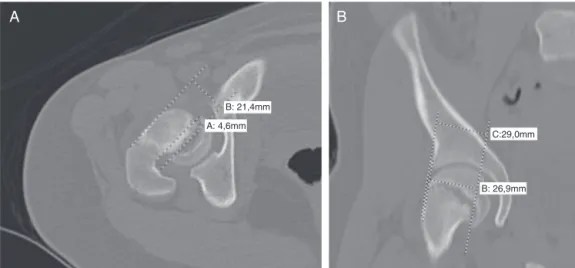
TheslipgradationproposedbyWilsonconsistsofthe rela-tion between the distance from the upper margin of the femoralnecktothe uppermarginofthefemoralheadand thediameterofthefemoralneck.Theslipwasdetermined in a three-dimensional manner. The percentage of head-to-neck contact in the axial (Fig. 6A) and coronal planes (Fig. 6B) was estimated, and the section with the largest femoral neck area was taken as standard.After obtaining thesedata,theresultbetweenthemwasobtainedto deter-minethethree-dimensionalcontact.Thethree-dimensional slipisthecomplementarynumberneededtoreach1(100%) (Fig.3cand7).
Imagingassessmentandstatisticalanalysis
DatawereanalyzedwithstatisticalsoftwareSTATA11(Stata Corporation,CollegeStation,USA).Theconcordancebetween thecategoricalvariableswasmadewiththeKappatest.The continuousvariableswereevaluatedwithpairedt-test,after confirmingnormalitywiththeKolmogorov–Smirnovtest.The limitofstatisticalsignificanceusedwas0.05.
TheevaluationoftheSouthwickangleswasdonethrough: 1.Categoricalclassificationinthreegroupsaccordingtothe differencebetweentheanglefoundandthenormalpattern: mildslip(0–30◦),moderateslip(30–50◦),severeslip(greater than 50◦)13,26; 2. Continuousclassification accordingto the measuredangle.Thevaluesconsiderednormalare145◦inthe APX-rayand10◦intheProfileX-ray.27
Fig.5–Femoralhead–neckangle(FHNA)throughaCTaxial section.
totheanglefound:mildslip(lessthan50◦),severeslip(greater than50◦).21
ThedifferencesobtainedfortheWHNSwerecontinuously andcategoricallyclassified.Thecategoricalclassificationas proposedbyWilsonetal.28:mild(0–33%),moderate(33–50%) andsevere(greaterthan50%)slip.
WHNS = 1 – (WHNS axial plane x WHNS coronal plane)
WHNS= 1 – [(4.6/21.4) × [(26.9/29)]
WHNS = 1 – [0.21 × 0.92]
WHNS= 1 – 0.19
WHNS= 0.81= 81%
Fig.7–Mathematicalmethodtothree-dimensionally determineWilson’sslip.
Results
Twenty-sixhipswereevaluatedin21patients(Tables1–6).
Cooper’sobliqueplane
There was nosignificant difference betweenthe two com-paredmethods(p=0.59)and bothshowed good correlation (r=0.93)andgoodconcordance(kappa=0.81).Onlyonecase ofthe26evaluatedhadtheclassificationchangedfromsevere tomildwhentheCTcoronalplanewaschosenasmeasuring method.
Wilson’sslip
Theslips obtainedinthe three-dimensional evaluation[85 (71.2–98.8) %] are significantly higher (p<0.001)than those found in the AP X-rays [31.3 (20.2–42.4) %] and Profile X-ray [44.2 (34.1–54.3) %]. The concordance between the classificationby CTand X-ray wasweak (kappa=0.216). In the cases considered mild or moderate in the uniplanar evaluation, 80% were classified as severe by the biplanar evaluation.
Southwickangle
Theangles foundin the APX-ray[19.5 (9.7–29.3)◦] are sig-nificantly (p<0.001) lower than those found in the Profile
B: 21,4mm
C:29,0mm
B: 26,9mm A: 4,6mm
A
B
Table1–Descriptiveanalysis.
Gender
Male 14
Female 7
Laterality
Right 14(53.8%)
Left 12(42.2%)
Bilateralinvolvement 5
Boys 4(28.57%)
Girls 1(14.28%)
Age 13.7(12.9–14.5)
years
Boys 13.9(13.1–14.8)
years
Girls 13.2(11.1–15.3)
years
Cooper’sobliqueplane
APX-ray/axialCT 70.3(62.5–78.0)◦
CoronalCT/axialCT 71.0(64.3–77.7)◦
Wilson’sneck-headslip
CT(3D) 85.0(71.2–98.8)%
APX-ray 31.3(20.2–42.4)%
ProfileX-ray 44.2(34.1–54.3)%
Southwickangle
CT(3D) 47.9(38.0–57.8)◦
APX-ray 19.5(9.7–29.3)◦
ProfileX-ray 51.5(43.8–59.2)◦
Table2–Descriptiveanalysis.
Mild Moderate Severe
Classificationthrough Cooper’sobliqueplane
–
APX-ray/axialCT 3 – 23
CoronalCT/axialCT 4 – 22
Wilson’sclassification
CT(3D) 1 2 23
X-ray 5 10 11
Southwickclassification
CT(3D) 8 6 12
X-ray 3 6 17
X-ray[51.5(43.8–59.2)◦]andbytomographicevaluationinthree dimensions[47.9(38.0–57.8)◦].There wasnosignificant dif-ference(p=0.28)betweenmeasurementstakenintheprofile X-rayand3DCT.However,therewasatendencytoclassify casesashavinglowerseveritybythethree-dimensionalCT
methodwhenconfrontedwiththeradiographicmethod.The
concordancebetweenthethree-dimensionalCTandthe bipla-narX-rayevaluationwasweak(kappa=0.306).
Table3–Cooper’sobliqueplaneconcordance.
ClassificationofCooper’s obliqueplanewithcoronal
CT
Mild Severe Total
Cooper’sOblique PlaneClassification usingAPX-ray
Mild 3 0 3
Severe 1 22 23
Total 4 22 26
Kappa=0.83;p<0.001.
Table4–ConcordanceofWilson’sclassificationthrough CT(3D)andX-ray.
Wilson’sClassification throughCT(3D)
Mild Moderate Severe Total
Wilson’s classification throughX-ray
Mild 1 0 4 5
Moderate 0 2 8 10
Severe 0 0 11 11
Total 1 2 23 26
Kappa=0.216;p=0.018.
Table5–ConcordanceofSouthwickclassification throughCT(3D)andX-ray.
Southwickclassification throughCT(3D)
Mild Moderate Severe Total
Southwick classification throughX-ray
Leve 3 0 0 3
Moderate 4 1 1 6
Severe 1 5 11 17
Total 8 6 12 26
Kappa=0.306;p=0.020.
Concordancebetweenthedifferentclassifications
Theconcordancebetweentheclassicallyusedclassifications,
Southwick-X-ray,Wilson-X-ray,andCooper,wasweak,with
kappaof0.05–0.15.
Discussion
The literatureon SCFEstill lacksstandardizationto evalu-atetheseverityofthediseaseandthetherapyproposal.In
Table6–Concordancebetweendifferentclassifications.
Classificationthrough Cooper’sobliqueplane
Classificationthrough Wilson’sslipwithX-ray
Classificationthrough Wilson’sslip–X-ray
Kappa:0.107
p:0.08 Classificationthrough
Southwickangle–X-ray
Kappa:0.152 Kappa:0.058
addition, thefew articlesaimedatanalyzingthe intraand interobserverconcordancesoftheuniplanarmethodssuggest low values,29 whereas multiplanar evaluations have better concordance.13,21,23Thereareseveralarticleswiththeirown proposalsforclassificationofthedisease,butfewofthem con-siderthemultiplanarnatureofthedeformity.Webelievethat thethree-dimensionalevaluationallowsbetterdetermination of the actual proximal femur deformity and intra and interobserveragreement.Inaddition,thethree-dimensional evaluationcan modifythe therapeutic management. How-ever,three-dimensionalhipdeformitiescannotbeadequately measuredbyradiographicmeans,becauseitisnotpossible toguaranteetheperpendicularityofraysbetweenthe antero-posteriorandprofileincidences.Therefore,theuseofmethods thatallowthree-dimensionalevaluation,suchasCTand mag-neticresonanceimaging,isnecessary.
Asinitiallyexpected,thereislittledifferencebetween eval-uatingCooper’sobliqueplanewithCTaxialsection andAP X-ray,orusingtheaxialandcoronalCTsections.Amongthe mostwidespreadmethods,thisisoneofthefewthatevaluates thethree-dimensional deformity,but thereare stillstudies thatsupportthe50◦-limitadoptedbyCooperetal.21for mod-ifying thetherapeuticapproach. Thisauthor, based onthe obliqueplane,suggeststhatdeviationssmallerthan50◦ are treatedwithinsitufixationanddeviationsgreaterthan 50◦ withdislocationfollowedbyanatomicalreductionofthehip. Thethree-dimensionalevaluationofWilson’sslipshowed significantlyhigher valuesthan theX-rayevaluation.Thus, 80%ofmildcaseswouldhaveitsmanagementaltered;more complexsurgicalproceduresareadoptedwhenthediseaseis biplanarlyclassified.Ontheotherhand,Southwick’s classifi-cationthroughCTunderestimatedthevaluesfoundbyX-ray; 66%of thecases classifiedas moderatein anX-raywould havethetherapychangedtolessinvasiveproceduresifthe3D classificationwasadopted,inagreementwiththepreviously reportedfindingsbyRicholtetal.23
Another important aspect to consider is the lack of agreement between the different classifications that are commonlyused:Southwick-X-ray,Wilson-X-ray,andCooper. Whenevaluatedsimultaneouslybythethreemethods,eight of the 26 hips analyzed (30.79%) could have the thera-peutic management changed, depending on the reference classification.Noneofthecaseswereclassifiedasmild simul-taneously by all methods, while only 33.3% (8/24) of the caseswere consistently considered severe byall classifica-tions.
Three-dimensional evaluations may be the best way to guide therapeutic management, since they allow estimat-ing the deformityinherentto the disease ina waythat is closer to reality and with better reproducibility. The best three-dimensionalevaluationmethodisamatterthatneeds tobe deepened, but we see the three-dimensional evalua-tionofWilson’sslipand theSouthwickangleaspromising options,sincetheyareadaptationsoftwowidelyused mod-els with a wide series of cases previously studied in the literature.10,15–17,22,26,28
Alimitation of the present article isthe initialseverity of the disease in the individuals studied. Future research mayevaluatethedifferencebetweenradiographicand tomo-graphicfindingsinpatientswithmilderSCFE.Inaddition,the
lackofacontrolgroup(whichcouldbeformed,forexample, byanasymptomaticpopulation),limitstheconclusionofthe differenceinradiographicandtomographicfindings.
TheauthorsbelievethatimprovingpatientcarewithSCFE dependsonbetterstandardizationofdeformitygradationand therapeuticmanagement.Todothis,wemust:1)definethe roleofradiologicalmethodsthatallowathree-dimensional evaluationofthe deformity,suchascomputed tomography andmagneticresonanceimaging;2)tostandardizetheideal therapeuticindicationaccordingtothedeformity,infaceof newdiagnosticoptions.
Conclusion
ThepresentstudyfounddifferencesinSCFEanglesbetween measurements taken by radiography and computed tomo-graphy. A multiplanar evaluation of the proximal femoral deformityisaviableoptionwiththepotentialtochangethe classification ofthe disease in the patientsand, therefore, therapeuticmanagement.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LoderRT.Thedemographicsofslippedcapitalfemoral epiphysis.Aninternationalmulticenterstudy.ClinOrthop RelatRes.1996;322:8–27.
2.SharmaV,OddyMJ.Slippedcapitalfemoralepiphysis:a review.BrJHospMed(Lond).2014;75(3):155–61.
3.MurrayAW,WilsonNI.Changingincidenceofslippedcapital femoralepiphysis:arelationshipwithobesity?JBoneJoint SurgBr.2008;90(1):92–4.
4.RahmeD,ComleyA,FosterB,CundyP.Consequencesof diagnosticdelaysinslippedcapitalfemoralepiphysis.J PediatrOrthopBr.2006;15(2):93–7.
5.LoderRT.Whatisthecauseofavascularnecrosisinunstable slippedcapitalfemoralepiphysisandwhatcanbedoneto lowertherate?JPediatrOrthop.2013;33Suppl.1:S88–91.
6.MullinsMM,SoodM,Hashemi-NejadA,CatterallA.The managementofavascularnecrosisafterslippedcapital femoralepiphysis.JBoneJointSurgBr.2005;87(12):1669–74.
7.YarbroughR,GrossR.Chondrolysis:anupdate.JPediatr Orthop.2005;25(5):702–4.
8.IngramAJ,ClarkeMS,ClarkeCSJr,MarshallWR.Chondrolysis complicatingslippedcapitalfemoralepiphysis.ClinOrthop RelatRes.1982;(165):99–109.
9.HosalkarHS,PandyaNK,BomarJD,WengerDR.Hip
impingementinslippedcapitalfemoralepiphysis:achanging perspective.JChildOrthop.2012;6(3):161–72.
10.HanssonG,BillingL,HogstedtB,JerreR,WallinJ.Long-term resultsafternailinginsituofslippedupperfemoral
epiphysis.A30-yearfollow-upof59hips.JBoneJointSurgBr. 1998;80(1):70–7.
12.TinsB,Cassar-PullicinoV,McCallI.Theroleofpre-treatment MRIinestablishedcasesofslippedcapitalfemoralepiphysis. EurJRadiol.2009;70(3):570–8.
13.MonazzamS,DwekJR,HosalkarHS.MultiplanarCT assessmentoffemoralheaddisplacementinslippedcapital femoralepiphysis.PediatrRadiol.2013;43(12):1599–605.
14.LoderRT,AronssonDD,WeinsteinSL,BreurGJ,GanzR, LeunigM.Slippedcapitalfemoralepiphysis.InstrCourse Lect.2008;57:473–98.
15.SankarWN,VanderhaveKL,MatheneyT,Herrera-SotoJA, KarlenJW.ThemodifiedDunnprocedureforunstableslipped capitalfemoralepiphysis:amulticenterperspective.JBone JointSurgAm.2013;95(7):585–91.
16.SouthwickWO.Osteotomythroughthelessertrochanterfor slippedcapitalfemoralepiphysis.JBoneJointSurgAm. 1967;49(5):807–35.
17.DunnDM,AngelJC.Replacementofthefemoralheadbyopen operationinsevereadolescentslippingoftheupperfemoral epiphysis.JBoneJointSurgBr.1978;60B(3):394–403.
18.KramerWG,CraigWA,NoelS.Compensatingosteotomyat thebaseofthefemoralneckforslippedcapitalfemoral epiphysis.JBoneJointSurgAm.1976;58(6):796–800.
19.BarmadaR,BruchRF,GimbelJS,RayRD.Baseoftheneck extracapsularosteotomyforcorrectionofdeformityin slippedcapitalfemoralepiphysis.ClinOrthopRelatRes. 1978;132:98–101.
20.CohenMS,GelbermanRH,GriffinPP,KasserJR,EmansJB, MillisMB.Slippedcapitalfemoralepiphysis:assessmentof epiphysealdisplacementandangulation.JPediatrOrthop. 1986;6(3):259–64.
21.CooperAP,SalihS,GeddisC,FosterP,FernandesJA,Madan SS.Theobliqueplanedeformityinslippedcapitalfemoral epiphysis.JChildOrthop.2014;8(2):121–7.
22.WilsonPD.Thetreatmentofslippingoftheupperfemoral epiphysiswithminimaldisplacement.JBoneJointSurg. 1938;20:379–99.
23.RicholtJA,HataN,KikinisR,ScaleD,MillisMB.Quantitative evaluationofangularmeasurementsonplainradiographsin patientswithslippedcapitalfemoralepiphysis:a
3-dimensionalanalysisofcomputedtomography-based computermodelsof46femora.JPediatrOrthop. 2008;28(3):291–6.
24.SabharwalS.Pediatriclowerlimbdeformities:principlesand techniquesofmanagement.SpringerInternational
Publishing;2016.
25.WeinerDS,CookAJ,HoytWAJr,OravecCE.Computed tomographyinthemeasurementoffemoralanteversion. Orthopedics.1978;1(4):299–306.
26.BoyerDW,MickelsonMR,PonsetiIV.Slippedcapitalfemoral epiphysis.Long-termfollow-upstudyofonehundredand twenty-onepatients.JBoneJointSurgAm.1981;63(1): 85–95.
27.HerringJA,TachdjianMO.Tachdjian’spediatricorthopaedics: fromtheTexasScottishRiteHospitalforChildren.5thed. Philadelphia:Elsevier/Saunders;2014.
28.WilsonPD,JacobsB,SchecterL.Slippedcapitalfemoral epiphysis:anend-resultstudy.JBoneJointSurgAm. 1965;47:1128–45.