w w w . r e u m a t o l o g i a . c o m . b r
REVISTA BRASILEIRA DE
REUMATOLOGIA
Original article
Intra-articular injection in patients with juvenile
idiopathic arthritis: factors associated with a good
response
Ana Luiza Garcia Cunha
a,∗, Vanessa Bugni Miotto e Silva
a,b, Fabiane Mitie Osaku
a,
Luísa Brasil Niemxeski
b, Rita Nely Vilar Furtado
c, Jamil Natour
c,
Maria
Teresa
de
Sande
e
Lemos
Ramos
Ascensão
Terreri
a,baUniversidade Federal de São Paulo (UNIFESP), Departamento de Pediatria, Disciplina de Alergia, Imunologia Clínica e Reumatologia,
São Paulo, SP, Brazil
bUniversidade Federal de São Paulo (UNIFESP), São Paulo, SP, Brazil
cUniversidade Federal de São Paulo (UNIFESP), Departamento de Medicina, Disciplina de Reumatologia, São Paulo, SP, Brazil
a r t i c l e
i n f o
Article history:
Received 24 September 2014 Accepted 30 August 2015 Available online 26 February 2016
Keywords:
Intra-articular injection Juvenile idiopathic arthritis Triamcinolone hexacetonide Treatment and uveitis
a b s t r a c t
Introduction:Intra-articular injection of corticosteroids (IIC) for treatment of patients with
juvenile idiopathic arthritis (JIA) is increasingly used in Pediatric Rheumatology.
Objectives:To describe the clinical course of patients undergoing IIC in our Pediatric
Rheuma-tology Unit.
Methods:Retrospective study of patients with JIA undergoing IIC from January 2008 to
December 2012, with a minimum follow-up of six months after the injection. Good response to IIC was set as the presence of inactivity on the infiltrated joint by at least six months.
Results:Eighty-eight patients underwent a total of 165 IICs. Of these, 75% were girls and
35.2% had persistent oligoarticular JIA. The mean age at diagnosis was 6.8 years, and when IIC was carried out, 12.2 years. Regarding patients, younger age at diagnosis (p= 0.037) and the occurrence of uveitis in the course of the disease (p= 0.015) were associated with good response to IIC. From 165 IICs, 63% had a good response and joints remained inactive for a median of 18.1 months. The type of joint injection (p= 0.001), lesser values stated in the overall visual analog scale by the physician (p= 0.015) and by parents/patient (p= 0.01) have been associated with a good response to IIC. Nine adverse events (5.4%) were observed.
Conclusion:In our study, more than half of the joints showed a good response to IIC. Younger
patients at diagnosis and uveitis during the course of the disease had good response to IIC. Knees, wrists and elbows were the joints that best responded to IIC. IIC proved to be a safe procedure.
© 2016 Elsevier Editora Ltda. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Corresponding author.
E-mail:[email protected](A.L.G. Cunha). http://dx.doi.org/10.1016/j.rbre.2016.01.001
Infiltrac¸ão
intra-articular
em
pacientes
com
artrite
idiopática
juvenil:
fatores
associados
à
boa
resposta
Palavras-chave:
Infiltrac¸ãointra-articular Artriteidiopáticajuvenil Hexacetonidodetriancinolona Tratamentoeuveíte
r
e
s
u
m
o
Introduc¸ão:Ainfiltrac¸ãointra-articulardecorticosteroides(IIC)paratratamentodepacientes
comartriteidiopáticajuvenil(AIJ)écadavezmaisusadaemreumatologiapediátrica.
Objetivos: Descreveraevoluc¸ãoclínicadospacientessubmetidosàIICemnossosetorde
reumatologiapediátrica.
Métodos: EstudoretrospectivodepacientescomAIJsubmetidosà IICdejaneiro/2008a
dezembro/2012,comseguimentomínimodeseismesesapósainfiltrac¸ão.Boaresposta àIICfoidefinidacomoinatividadenaarticulac¸ãoinfiltradapor,nomínimo,seismeses.
Resultados: Foramsubmetidosa88pacientesa165IICs.Desses,75%erammeninase35,2%
apresentavamAIJoligoarticularpersistente.Amédiadeidadeaodiagnósticofoide6,8anos eàIICde12,2anos.Emrelac¸ãoaospacientes,amenoridadeaodiagnóstico(p=0,037)ea ocorrênciadeuveítenocursodadoenc¸a(p=0,015)foramassociadosàboarespostaàIIC. Das165IICs,63%apresentaramboarespostaeasarticulac¸õespermaneceraminativaspor umtempomédiode18,1meses.Otipodearticulac¸ãoinfiltrada(p=0,001),menoresvalores naescalavisualanalógicaglobaldomédico(p=0,015)edospais/paciente(p=0,01)foram associadosaumaboarespostaàIIC.Noveefeitosadversos(5,4%)foramobservados.
Conclusão: Emnossoestudo,maisdametadedasarticulac¸õesmostrouboarespostaàIIC.
Ospacientescommenoridadeaodiagnósticoeuveíteduranteocursodadoenc¸ativeram boarespostaàIIC.Osjoelhos,punhosecotovelosforamasarticulac¸õesquemaisbem responderamàIIC.AIICmostrouserumprocedimentoseguro.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Juvenileidiopathicarthritis(JIA)isachronicrheumatic dis-easemostcommoninchildhood,beingasignificantcauseof disabilityandreducedqualityoflife.1
The goal of JIA treatment is to control inflamma-tion and prevent a premature loss of cartilage and joint function. JIA can be treated with a combination of non-steroidal anti-inflammatory drugs (NSAIDs), disease-modifying antirheumatic drugs (DMARDs), biologic drugs, systemiccorticosteroids,intra-articularinjectionsof cortico-steroids(IIC)andphysiotherapy.1–4
IICisoftenusedtotreatJIA.5,6 Currentlythisprocedure
isinusenotonlyinpatientswiththeoligoarticularsubtype (i.e.thosewithapoorresponsetoNSAIDsandasafirst-line therapy),butalsointhosesufferingalengthyorcomplicated arthritis(accompaniedbyjointcontracturesandgrowth dis-orders),oreveninthosecaseswhereoneisawaitingbythe therapeuticeffectofDMARDs.2,7–10
Althoughthelong-termefficacyand thepotentialeffect onactivityandprogressionofJIAstillneedmorestudies,IIC canpromotesignificantpainrelief,functionaljoint improve-ment,andanincreasedlikelihoodofdeformitycorrectionand ofadaptationofbonegrowth.Inaddition,IICisconsidered asasafeandeffectivemethodtotreataffectedjoints.1,11–16
Furthermore, this procedure allows an early rehabilitation and a reduction – or even discontinuation – of systemic medications.16,17
Mostofourknowledgeonjointinjectioncomesfrom stud-iesinadults,withfewreportsinchildren.Thisstudydescribes
theclinicaloutcomeofpatientsundergoingIICinaPediatric RheumatologyUnitatUNIFESPoveraperiodoffiveyears,and alsoevaluatesfactorsassociatedwithagoodresponsetothis therapy.
Patients
and
methods
Thisisaretrospective studyofmedicalrecordsofpatients withJIA,who werefollowed atthe PediatricRheumatology unitofUNIFESPandsubmittedtoIICintheperiodfrom Jan-uary1,2008toDecember31,2012.Theirinclusioncriterion wasaminimum6-monthfollow-upafterthejointinjection. PatientswithIICsproceduresperformedinotherunitswere excluded.
Demographic and clinical data of each patient were assessed, and a preliminaryclassification and evolutionof JIAwascarriedoutaccordingtothecriteriaofthe Interna-tionalLeagueofAssociationsforRheumatology(ILAR)18:the
presenceofuveitisinthecourseofdisease,thepresenceof autoantibodies(antinuclearantibody–ANA–consideredas positiveforchildrenwithtitles≥1:160,andrheumatoidfactor –RF)andofhumanleukocyteantigen(HLA)B27.
visualanalogscale(VAS,0–10)valueassignedbythephysician andbyparents/patient,C-reactiveprotein(CRP),and erythro-cytesedimentationrate(ESR)atthetimeofinjection.Adverse eventswererecordedaftereachinjection.
IICswereperformedbyasinglepediatricrheumatologist trainedaccordingtoprotocolsspecificforeachtypeofjoint.19
Injections were performed under localanesthesia with 2% lidocainewithoutvasoconstrictor.Theonlymedicationused was triamcinolone hexacetonide in doses of 1–2mg/kg for largejoints,0.5–1mg/kgformediumjoints,and4–10mgfor smalljoints,withamaximumdoseof100mg.Thepatients wereaskedtoresttheirjointaftertheprocedureforaperiod of48h.
Weconsideredajointasinactiveintheabsenceofarthritis checkedbyclinicalexaminationand/orUS.Thepatientwas consideredaswithagoodresponsetoIICwhenallinjected joints remained inactive forat leastsix months(complete response)orwhensomeofinjectedjointsremainedinactive foratleastsixmonths(partialresponse).Poorresponsewas definedaswhenallinfiltratedjointsremainedactiveor exhib-itedreactivationwithinaperiodundersixmonthsafterIIC. TheanswertoIICineachjointwasrankedas“goodresponse” (theinfiltratedjointremainedinactiveforatleastsixmonths) and“poorresponse”(theinfiltratedjointdidnotanswer,orits reactivationoccurredinlessthansixmonths).
Demographicand clinicalcharacteristics were described inabsoluteandrelativefrequencies,means±standard devi-ation,andminimumandmaximumvalues,accordingtothe natureofthevariables.Tocomparethedistributionsof con-tinuous variables between two groups, Student’s t test or Mann–Whitneytestwasused,takinginto accountthe data normality.Categoricalvariables betweengroups were com-paredusingtheChi-squaredtestorFisher’sexact test.The statisticalsignificancewassetat5%.
ThisstudywasapprovedbytheResearchEthicsCommittee oftheUniversidadeFederaldeSãoPaulo(OpinionNumber: 326891).
Results
FromJanuary2008toDecember2012,88patientswithJIAwere subjectedtoatotalof165IICs,withameanof1.87(range,1–6) injectionsperpatient.Themeanlengthoffollow-upwas7.1 (0.8–17.1)years.
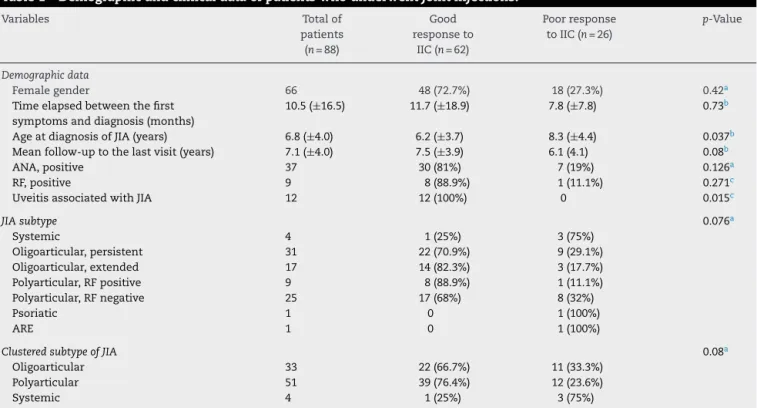
Sixty-twopatients(70.4%)hadagoodresponsetoIIC,39 (44.3%)patientsachievedacompleteresponse,23(26.1%)were benefitedwithapartialresponsetoIIC,and26patients(29.5%) exhibitedapoorresponsetoallIICstowhichtheywere sub-jected.Forthesakeofourstatisticalanalysis,subtypesofJIA weregroupedaccordingtothecourseofthediseasein: oligoar-ticular–37.5%(persistentoligoarticularJIA,enthesitis-related arthritis[ERA],andpsoriaticJIA[patientswithamaximumof4 affectedjoints]),polyarticular–58%(polyarticularRF-positive JIA,polyarticularRF-negativeJIA,andextended oligoarticu-larJIA) and systemic – 4.5%.Regarding our evaluationper patient,agoodresponsetoIICwasassociatedwithyounger ageatdiagnosisofJIA(p=0.037)andalsoforthosepatients withuveitisoccurringatanytimeinthecourseofthedisease (p=0.015).Of21patientswithuveitis,13wereANApositive.
ElevenpatientswereinvestigatedforthepresenceofHLA-B27 andallofthemwerenegative.Table1listsdemographicand clinicaldataforthegroupofpatients.
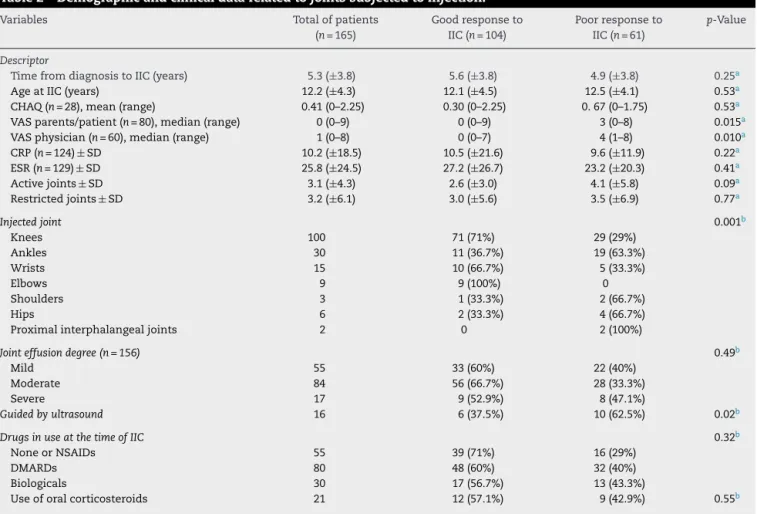
Regardingthe165jointsinjected,104(63%)showedgood responsetoIIC,whichwasassociatedwithlowerVASvalues assigned bythephysician(p=0.015)andbyparents/patient (p=0.010).ThelowestvaluesofVASwereassociatedwitha better generalconditionofthe patientwithgood response toIIC,andwithlesspainandinflammatoryactivity. Further-more,thetypeofjointsubmittedtoinjection(p=0.001),also was associatedwith agood response toIIC; knees, wrists, andelbowswerethosejointsshowingbetterresponsetoIIC. Table2listsdatarelatingtointra-articularinjections.
Generally,US-guidedinjectionsinthissmallsampleof16 patientswithlongerdiseasedurationandpreviousinjections showedpoorresponsetoIICs(p=0.02);thisfactisassociated withhighervaluesofCHAQ(p=0.03),highernumberof injec-tionswithpoorresponse(p=0.01)andashortertimetorelapse (p=0.02)comparedtopatientssubmittedtoblindlyperformed procedures.DatarelatedtoUS-guidedinjectionsareshownin Table3.
ThejointsthatrespondedfavorablytoIICremained inac-tiveforameanof18.1±13.2months.Ontheotherhand,in thosejointswithpoorresponse,therewasrecurrenceaftera meanperiodof2.6±2.1months.
Ofthe165injectionscarriedout,43(26.1%)wereapplied in17patientswhosejointswereinfiltratedinmorethanone occasion(14knees,3ankles,and2hips),withameanof2.26 (range,2–3)IICsperjoint.Amongthesejoints,24(55.8%)hada goodresponsetoIIC,withameantimeof12.3monthsofjoint inactivityaftertheprocedure.
Takinginto accountthetotalnumberofIICsperformed, nine(5.4%)adverseeffectsoccurredinninepatients:fivecases ofperiarticularhypotrophyandfourcasesofhypochromiaat thesiteofinjection.
Discussion
Inthisstudy,weobservedagoodresponsetoIICinmorethan halfofpatients,especiallythoseyounger-agedatthe diagno-sisofJIA,andpatientspresentinguveitisduringthecourse ofthedisease.Additionally,thetypeofinjectedjoint(knees, wrists, andelbows) and lowvaluesofVASassigned bythe physicianandbytheparents/patientwereassociatedwitha goodresponsetoIIC.TheuseofUStoguidetheprocedures wasassociatedwithworseresponsestoIIC.
OfthetotalnumberofIICsperformedout,morethanhalf presentedinactivityofarthritisformorethan6months,with ameandurationofaboutoneandahalfyears.Theinactivity ratesaftertheinjectionvariesdependingonthestudy:around 56.1–82% aftersixmonths,42–80%after1year,and30–63% after2years.5,10,12–14,20–22Theliteraturerevealsawide
varia-tionamongstudieswithrespecttomeanresponseduration timeinpatientswithJIA,rangingfrom6to23.5months.7,23–25
Among the potential factors associated with a good responsetoIICdescribedintheliterature,wefoundabsence ofANA,11,23presenceofHLA-B27,23absenceofatrophyinthe
localofinjection,23concomitantuseofMTX,7,10,23
Table1–Demographicandclinicaldataofpatientswhounderwentjointinjections.
Variables Totalof
patients (n=88)
Good responseto
IIC(n=62)
Poorresponse toIIC(n=26)
p-Value
Demographicdata
Femalegender 66 48(72.7%) 18(27.3%) 0.42a
Timeelapsedbetweenthefirst symptomsanddiagnosis(months)
10.5(±16.5) 11.7(±18.9) 7.8(±7.8) 0.73b
AgeatdiagnosisofJIA(years) 6.8(±4.0) 6.2(±3.7) 8.3(±4.4) 0.037b
Meanfollow-uptothelastvisit(years) 7.1(±4.0) 7.5(±3.9) 6.1(4.1) 0.08b
ANA,positive 37 30(81%) 7(19%) 0.126a
RF,positive 9 8(88.9%) 1(11.1%) 0.271c
UveitisassociatedwithJIA 12 12(100%) 0 0.015c
JIAsubtype 0.076a
Systemic 4 1(25%) 3(75%)
Oligoarticular,persistent 31 22(70.9%) 9(29.1%)
Oligoarticular,extended 17 14(82.3%) 3(17.7%)
Polyarticular,RFpositive 9 8(88.9%) 1(11.1%)
Polyarticular,RFnegative 25 17(68%) 8(32%)
Psoriatic 1 0 1(100%)
ARE 1 0 1(100%)
ClusteredsubtypeofJIA 0.08a
Oligoarticular 33 22(66.7%) 11(33.3%)
Polyarticular 51 39(76.4%) 12(23.6%)
Systemic 4 1(25%) 3(75%)
IIC,intra-articularinjectionofcorticosteroids;ANA,antinuclearantibody;RF,rheumatoidfactor;JIA,juvenileidiopathicarthritis;ARE,arthritis relatedtoenthesitis.
a Chi-squaredtest. b Mann–Whitneytest. c Fisher’sexacttest.
presenceofANA,useofDMARDs,andJIAsubtypewerenot associatedwithabetterorworseresponsetoIIC.Amongour patients,nonewasHLAB-27-positiveandinnoneofthemIIC wasperformedundersedation,whichpreventedthe assess-mentofthesefactors.
The literature also describes as indicators of worse response: absence of ANA (contrary to the studies cited above),7,10increasesinCRPandESR,7,10,22systemicand
pol-yarticularJIAsubtypes,7,10,20,25andelbowinfiltration.10Inour
studywefoundagoodresponsetoelbowinjection.Despitethe smallnumberofpatientswithsystemicJIAinthisstudy,and takingintoaccountthatnostatisticalsignificancewasfound, wealsonotedworseresponsestoIICinpatientswithsystemic JIA,showingthattheprocedureinthisdiseasesubtypeshould beevaluatedindividually.
No association was observed between the occurrence of uveitis and a better response to IIC in the study con-ducted by Marti et al.,23 contrary to our study, where the
occurrenceofuveitiswasassociatedwithabetterresponse toIIC.
ComparedtoVASvaluesassignedbythephysicianandby parents/patient,theseparameterswerenotassociatedwith responsetoIICinthestudybyRavellietal.22 Ontheother
hand,thestudybyMorettietal.26 showedthatalowerVAS
value assigned by the physician was a good predictor of responsetoIICinpatientswiththeoligoarticularsubtype.In ourstudy,higherprocedurevaluesofVAS,bothassignedby thephysicianandthepatient,wereassociatedwithaworse responsetoIIC.
Studies suggestthatthebesttimeforthecompletionof anIICprocedureisasearlyaspossibleinthecourseofthe disease–andthisisafactorofgoodresponsetoIIC.11,16 In
ourstudy,wefoundthatyounger-agedpatientsatdiagnosis showedagoodresponsetoIIC.Thismayberelatedtothemost commonsubtypeinthisagegroup,whichistheoligoarticular subtype;butalsodemonstratesthat,bybeingyounger,these patientscouldbeinanearlierstageofthedisease,whichisin linewithliteraturefindings.
One may obtain a long-lasting answer to IIC when using hexacetonide triamcinolone versus acetonide triamcinolone.5,21,23,27,28Thus,wechosetousehexacetonide
triamcinoloneinallofourinjections.
ThereisevidenceinfavorofabetterresponsetoIICwhen theprocedureisguidedbyanimagingtechnology(ultrasound orMRI),especiallyinthewrist,ankleandhip.3,29,30Contrary
tothis,wefoundapoorresponsetoUS-guidedIICinjection. Thisfindingmaybeduetothefactthat,inourstudy,guided injectionswereperformedonjointsthathadalreadyshowed apoorresponsetoblindly-conductedIIC,andislikelythatthis playedaroleinourresults.Prospectivestudiesinjointsnever subjectedtoinjectionshouldbeconducted,inordertobetter assesstheutilityofUStoguideIICinchildren.
Table2–Demographicandclinicaldatarelatedtojointssubjectedtoinjection.
Variables Totalofpatients
(n=165)
Goodresponseto IIC(n=104)
Poorresponseto IIC(n=61)
p-Value
Descriptor
TimefromdiagnosistoIIC(years) 5.3(±3.8) 5.6(±3.8) 4.9(±3.8) 0.25a
AgeatIIC(years) 12.2(±4.3) 12.1(±4.5) 12.5(±4.1) 0.53a
CHAQ(n=28),mean(range) 0.41(0–2.25) 0.30(0–2.25) 0.67(0–1.75) 0.53a
VASparents/patient(n=80),median(range) 0(0–9) 0(0–9) 3(0–8) 0.015a
VASphysician(n=60),median(range) 1(0–8) 0(0–7) 4(1–8) 0.010a
CRP(n=124)±SD 10.2(±18.5) 10.5(±21.6) 9.6(±11.9) 0.22a
ESR(n=129)±SD 25.8(±24.5) 27.2(±26.7) 23.2(±20.3) 0.41a
Activejoints±SD 3.1(±4.3) 2.6(±3.0) 4.1(±5.8) 0.09a
Restrictedjoints±SD 3.2(±6.1) 3.0(±5.6) 3.5(±6.9) 0.77a
Injectedjoint 0.001b
Knees 100 71(71%) 29(29%)
Ankles 30 11(36.7%) 19(63.3%)
Wrists 15 10(66.7%) 5(33.3%)
Elbows 9 9(100%) 0
Shoulders 3 1(33.3%) 2(66.7%)
Hips 6 2(33.3%) 4(66.7%)
Proximalinterphalangealjoints 2 0 2(100%)
Jointeffusiondegree(n=156) 0.49b
Mild 55 33(60%) 22(40%)
Moderate 84 56(66.7%) 28(33.3%)
Severe 17 9(52.9%) 8(47.1%)
Guidedbyultrasound 16 6(37.5%) 10(62.5%) 0.02b
DrugsinuseatthetimeofIIC 0.32b
NoneorNSAIDs 55 39(71%) 16(29%)
DMARDs 80 48(60%) 32(40%)
Biologicals 30 17(56.7%) 13(43.3%)
Useoforalcorticosteroids 21 12(57.1%) 9(42.9%) 0.55b
IIC,intra-articularinjectioncorticosteroids;SD,standarddeviation;CHAQ,ChildhoodHealthAssessmentQuestionnaire;VAS,visualanalog scale;CRP,C-reactiveprotein,ESR,erythrocytesedimentationrate;NSAIDs,nonsteroidalanti-inflammatorydrugs;DMARDs,disease-modifying antirheumaticdrugs.
a Mann–Whitneytest. b Chi-squaredtest.
Table3–Comparisonbetweeninjectionguidedversusnotguidedbyultrasound(US).
Variables US-guidedinfiltrations
(n=16)
InfiltrationsunguidedbyUS (n=149)
p-Value
Descriptor
TimefromdiagnosistoIIC(years) 5.9(±3.4) 5.2(±3.7) 0.63a
AgeatIIC(years) 12.1(±5.2) 12.2(±4.2) 0.94a
CHAQ(n=28),mean(range) 1.6(1–2.25) 0.3(0–1.75) 0.03a
VASparents/patient(n=80),median(range) 5(1–6) 0(0–9) 0.42a
VASphysician(n=60),median(range) 1(1–4) 3(0–8) 0.46a
CRP(n=124)±SD 11(±17.5) 10(±18.6) 0.89a
ESR(n=129)±SD 25.3(±18.4) 25.8(±25.2) 0.73a
Activejoints±SD 4.5(±6.7) 2.9(±3.9) 0.55a
Restrictedjoints±SD 6.7(±12.8) 2.8(±4.8) 0.30a
Numberofinjectionswithpoorresponse 1.4(±0.8) 0.8(±0.8) 0.01a
Relapsetime(months) 6.5(±7.2) 13(±13.2) 0.01a
Jointeffusiondegree(n=156) 0.29b
Mild 7 48
Moderate 8 76
Severe 0 17
IIC,intra-articularinjectionofcorticosteroids;SD,standarddeviation;CHAQ,ChildhoodHealthAssessmentQuestionnaire;VAS,visualanalog scale;CRP,C-reactiveprotein,ESR,erythrocytesedimentationrate.
The most common adverse events are: local subcuta-neoustissueatrophyattheIIC site,5,7,10,21–23,25,29 localskin
hypopigmentation,25,29acuteonsetofpain(jointirritationby
crystals ofthe drug),27 local calcification,25 adverse effects
relatedtogeneral/localanesthesia,23 and possiblesystemic
effectsofcorticosteroids(facialflushing,increasedappetite, moodswings).23,25,29Post-injectioninfectionisarareeventin
adults,27andtherearenopublishedreportsofpediatriccases.
Inourstudy,weobservedalowrateofadverseevents,none ofwhichwascharacterizedasasevereevent.
Ourstudyshowed thatIIC isan effectiveandsustained therapeuticmodality;morethanhalfofourpatientspresented agoodresponsetotheprocedure.Furthermore,ICCisasafe methodwithalowrateofadverseevents.Tothebestofour knowledge,thisisthefirststudyinchildrenandadolescents withJIAinourpopulation,thatsoughttoassessthefactors associatedwithIICresponse.However,thisstudyhassome limitations,suchasitsretrospectivedesign,whichaffected datacollection.Andwealsodidnotincludedatafrom injec-tionsappliedtothesepatientsinotherunits,whichoccurred inafewcases.Moreprospectivestudiesareneededtobetter definetheprofileofpatientswithJIAwhomaybenefitfrom IICprocedures.
Ourstudyalsoshowedthatayoungerageatthediagnosis ofJIA,occurrenceofuveitisinthecourseofthedisease,aswell asknee,wristandelbowinjectionandlowerVASvaluesboth fromthephysicianandpatientwerefactorsassociatedwitha betterresponsetoIIC.IICisaneffectivetherapeuticmodality presentingasustainedresponse.Furthermore,itisalsoasafe procedurethatcancontributetoimprovingthequalityoflife ofpatientswithJIA.
Conflict
of
interests
Theauthorsdeclarenoconflictofinterests.
r
e
f
e
r
e
n
c
e
s
1. PettyRE,CassidyJT.Chronicarthritisinchildhood.In: CassidyJT,PettyRE,editors.Textbookofpediatric rheumatology.Philadelphia:WBSaunders;2011.p.211–34. 2. BeukelmanT,PatkarNM,SaagKG,Tolleson-RinehartS,Cron
RQ,DeWittEM,etal.AmericanCollegeofRheumatology recommendationsforthetreatmentofjuvenileidiopathic arthritis:initiationandsafetymonitoringoftherapeutic agentsforthetreatmentofarthritisandsystemicfeatures. ArthritisCareRes(Hoboken).2011;63:465–82.
3. KanJH,GrahamTB.Combinedpre-injectionwristandankle MRIprotocolandsteroidjointinjectionsinjuvenile idiopathicarthritis.PediatrRadiol.2011;41:1326–32. 4. HashkesPJ,LaxerRM.Medicaltreatmentofjuvenile
idiopathicarthritis.JAMA.2005;294:1671–84.
5. ZulianF,MartiniG,GobberD,AgostoC,GiganteC,Zacchello F.Comparisonofintra-articulartriamcinolonehexacetonide andtriamcinoloneacetonideinoligoarticularjuvenile idiopathicarthritis.Rheumatol.2003;42:1254–9.
6. BeukelmanT,GuevaraJP,AlbertDA,SherryDD,BurnhamJM. Usageofintra-articularcorticosteroidinjectionsforthe treatmentofjuvenileidiopathicarthritis:asurveyof
pediatricrheumatologistsintheUnitedStatesandCanada. ClinExpRheumatol.2008;26:700–3.
7.PapadopoulouC,KostikM,Gonzalez-FernandezMI,BohmM, Nieto-GonzalezJC,PistorioA,etal.Delineatingtheroleof multipleintra-articularcorticosteroidinjectionsinthe managementofjuvenileidiopathicarthritisinthebiologic era.ArthritisCareRes(Hoboken).2013;65:1112–20. 8.RuthNM,PassoMH.Juvenileidiopathicarthritis:
managementandtherapeuticoptions.TherAdv MusculoskeletDis.2012;4:99–110.
9.RavelliA,LattanziB,ConsolaroA,MartiniA.Glucocorticoids inpaediatricrheumatology.ClinExpRheumatol.2011;29 Suppl68:S148–52.
10.LanniS,BertaminoM,ConsolaroA,PistorioA,
Magni-ManzoniS,GalassoR,etal.Outcomeandpredicting factorsofsingleandmultipleintra-articularcorticosteroid injectionsinchildrenwithjuvenileidiopathicarthritis. Rheumatology(Oxford).2011;50:1627–34.
11.LeporeL,DelSantoM,MalorgioC,PresaniG,PerticarariS, ProdanM,etal.Treatmentofjuvenileidiopathicarthritis withintra-articulartriamcinolonehexacetonide:evaluation ofclinicaleffectivenesscorrelatedwithcirculatingANAandT gamma/delta+andBCD5+lymphocytepopulationsof synovialfluid.ClinExpRheumatol.2002;20:719–22. 12.ÜnsalE,MakayB.Intra-articulartriamcinoloneinjuvenile
idiopathicarthritis.IndianPediatr.2008;45:995–7. 13.BreitW,FroschM,MeyerU,HeineckeA,GanserG.A
subgroup-specificevaluationoftheefficacyofintraarticular triamcinolonehexacetonideinjuvenilechronicarthritis.J Rheumatol.2000;27:2696–702.
14.PadehS,PasswellJH.Intraarticularcorticosteroidinjectionin themanagementofchildrenwithchronicarthritis.Arthritis Rheum.1998;41:1210–4.
15.WallaceC.Intra-articularsteroidinjectionsinJIA. Reumatología.2002;18:111–4.
16.BroströmE,HagelbergS,Haglund-AkerlindY.Effectofjoint injectionsinchildrenwithjuvenileidiopathicarthritis: evaluationby3D-gaitanalysis.ActaPediatr.2004;93:906–10. 17.WeitoftT,RönnblomL.Randomisedcontrolledstudyofpost
injectionimmobilizationafterintra-articularglucocorticoid treatmentforwristsynovitis.AnnRheumDis.2003;62:1013–5. 18.PettyRE,SouthwoodTR,MannersP,BaumJ,GlassDN,
GoldenbergJ,etal.InternationalLeagueofAssociationfor Rheumatologyclassificationofjuvenileidiopathicarthritis: secondrevision,Edmonton,2001.JRheumatol.2004;31:390–2. 19.FurtadoR,NatourJ.Infiltrac¸õesnoaparelholocomotor:
técnicaspararealizac¸ãocomesemoauxíliodeimagem.1a
ed.PortoAlegre:Artmed;2011.
20.NeidelJ,BoehnkeM,KüsterRM.Theefficacyandsafetyof intraarticularcorticosteroidtherapyforcoxitisinjuvenile rheumatoidarthritis.ArthritisRheum.2002;46:1620–8. 21.ZulianF,MartiniG,GobberD,PlebaniM,ZacchelloF,Manners
P.Triamcinoloneacetonideandhexacetonideintra-articular treatmentofsymmetricaljointsinjuvenileidiopathic arthritis:adouble-blindtrial.Rheumatol.2004;43:1288–91. 22.RavelliA,ManzoniSM,ViolaS,PistorioA,RupertoN,Martini
A.Factorsaffectingtheefficacyofintraarticular corticosteroidinjectionofkneesinjuvenileidiopathic arthritis.JRheumatol.2001;28:2100–2.
23.MartiP,MolinariL,BoltIB,SegerR,SaurenmannRK.Factors influencingtheefficacyofintra-articularsteroidinjectionsin patientswithjuvenileidiopathicarthritis.EurJPediatr. 2008;167:425–30.
25.BloomBJ,AlarioAJ,MillerLC.Intra-articularcorticosteroid therapyforjuvenileidiopathicarthritis:reportofan experientialcohortandliteraturereview.RheumatolInt. 2011;31:749–56.
26.MorettiC,ViolaS,PistorioA,Magni-ManzoniS,RupertoN, MartiniA,etal.Relativeresponsivenessofconditionspecific andgenerichealthstatusmeasuresinjuvenileidiopathic arthritis.AnnRheumDis.2005;64:257–61.
27.ClearyAG,MurphyHD,DavidsonJE.Intra-articular
corticosteroidinjectionsinjuvenileidiopathicarthritis.Arch DisChild.2003;88:192–6.
28.EberhardBA,SisonMC,GottliebBS,IlowiteNT.Comparisonof theintraarticulareffectivenessoftriamcinolone
hexacetonideandtriamcinoloneacetonideintreatmentof juvenilerheumatoidarthritis.JRheumatol.2004;31:2507–12. 29.YoungCM,ShielsWE,ColeyBD,HoganMJ,MurakamiJW,
JonesK,etal.Ultrasound-guidedcorticosteroidinjection therapyforjuvenileidiopathicarthritis:12-yearcare experience.PediatrRadiol.2012;42:1481–9.