Pure Robotic Retrocaval Ureter Repair
Ashok K. Hemal, Ranjit Rao, Sachit Sharma, Rhys G. E. Clement
Department of Urology (AKH) , Wake Forest University Health Sciences, Winston-Salem, North Carolina, USA and Department of Urology (RR, SS, RGEC), All India Institute of Medical Sciences, New Delhi, India
ABSTRACT
Purpose:To demonstrate the feasibility of pure robotic retrocaval ureter repair.
Materials and Methods: A 33 year old female presented with right loin pain and obstruction on intravenous urography
ZLWKWKHFODVVLFDO³¿VKKRRN´DSSHDUDQFH6KHZDVFRXQVHOHGRQWKHYDULRXVPHWKRGVRIUHSDLUDQGHOHFWHGWRKDYHDURERW
assisted repair. The following steps are performed during a pure robotic retrocaval ureter repair. The patient is placed in a
PRGL¿HGÀDQNSRVLWLRQSQHXPRSHULWRQHXPFUHDWHGDQGSRUWVLQVHUWHG7KHFRORQLVPRELOL]HGWRH[SRVHWKHUHWURSHULWRQHDO VWUXFWXUHVLQIHULRUYHQDFDYDULJKWJRQDGDOYHLQULJKWXUHWHUDQGGXRGHQXP7KHUHQDOSHOYLVDQGXUHWHUDUHPRELOL]HG
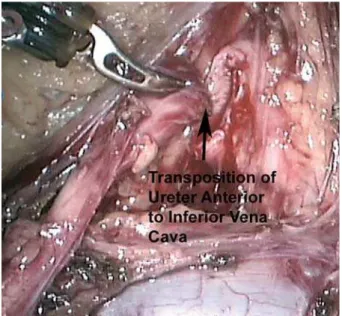
and the renal pelvis transected. The ureter is transposed anterior to the inferior vena cava and a pyelopyelostomy is per formed over a JJ stent.
Results:This patient was discharged on postoperative day 3. The catheter and drain tube were removed on day 1. Her JJ
VWHQWZDVUHPRYHGDWZHHNVSRVWRSHUDWLYHO\7KHSRVWRSHUDWLYHLQWUDYHQRXVXURJUDSK\DWPRQWKVFRQ¿UPHGQRUPDO
drainage of contrast medium.
Conclusion: 3XUHURERWLFUHWURFDYDOXUHWHULVDIHDVLEOHSURFHGXUHKRZHYHUWKHUHGRHVQRWDSSHDUWREHDQ\JUHDWDGYDQWDJH RYHUSXUHODSDURVFRS\DSDUWIURPWKHHUJRQRPLFHDVHIRUWKHVXUJHRQDVZHOOWKHVLPSOHULQWUDFRUSRUHDOVXWXULQJ
Key words: ureter; vena cava; abnormalities; laparoscopy; robotics Int Braz J Urol. 2008; 34: 734-8
INTRODUCTION
Retrocaval ureter is an unusual urological SUREOHPWKDWPD\UHTXLUHRSHUDWLYHUHSDLU)LJXUH 7KH¿UVWFDVHRIUHWURFDYDOXUHWHUUHSDLUZDVSXEOLVKHG LQE\$QGHUVRQDQG+\QHV7KHFODVVLFDO approach is an open technique of transposing the ureter anteriorly to the inferior vena cava followed by ureteroureterostomy. Laparoscopic retrocaval ureter repairs have also been performed but can be WHFKQLFDOO\ FKDOOHQJLQJ7KLV LV WKH ¿UVW FDVH RI D SXUHURERWLFUHSDLUWRRXUNQRZOHGJHSHUIRUPHGLQ an adult. We present our robotic technique of pure robotic retrocaval ureter repair.
SURGICAL TECHNIQUE
3DWLHQWSRVLWLRQ7KHSDWLHQWLVSRVLWLRQHG LQDPRGL¿HGÀDQNSRVLWLRQRYHUWKHNLGQH\EUHDN at a 45 degree angle. The patient is then adequately VHFXUHGZLWKVXSSRUWVDQGVWUDSSLQJDQGDOOSUHVVXUH areas are protected.
VXSHULRULOLDFVSLQHDQGXPELOLFXV$IXUWKHUPP port is inserted 3 cm below the camera port for the assistant to perform retraction and suction. The robot LVWKHQGRFNHG7KHZKROHSURFHVVRISQHXPRSHULWR QHXPSRUWLQVHUWLRQDQGGRFNLQJWDNHVPLQXWHV &RORQPRELOL]DWLRQ7KHKHSDWLFÀH[XUH DQGULJKWFRORQDUHPRELOL]HGPHGLDOO\WRSURYLGH H[SRVXUHWRWKHULJKWUHWURSHULWRQHDOVWUXFWXUHV ([SRVXUH RI UHWURSHULWRQHDO VWUXFWXUHV )LJXUH7KHULJKWUHQDOSHOYLVLQIHULRUYHQDFDYD ULJKWJRQDGDOYHLQULJKWXUHWHUDQGGXRGHQXPDUHDOO LGHQWL¿HG
0RELOL]DWLRQRIUHQDOSHOYLVDQGXUHWHU )LJXUH7KHULJKWUHQDOSHOYLVLVGLVVHFWHGIUHH IURP LWV VXUURXQGLQJ IDVFLDO OD\HUV7KH SUR[LPDO right ureter is dissected free where it can be seen to disappear superiorly under the inferior vena cava.
6. Transection of ureteropelvic junction: )LJXUH7KH UHQDO SHOYLV LV WUDQVHFWHG DQG WKH
Figure 1 – Pre-operative IVU.
Figure 2 – Exposure.
Figure 3 – Mobilization of renal pelvis and ureter.
ureteropelvic junction along with the retrocaval seg ment are transposed anterior to the inferior vena cava )LJXUHLQSUHSDUDWLRQIRUDS\HORS\HORVWRP\7KLV may not be possible for lower segment retrocaval ureters in which case ureteroureterostomy must be performed.
3\HORS\HORVWRP\)LJXUH3HUIRUPLQJD pyelopyelostomy is easier than a ureteroureterostomy DQGRQHLVOHVVOLNHO\WRSURGXFHVWULFWXUHIRUPDWLRQ due to the larger caliber structures as well as the bet ter blood supply as one goes more superiorly. This is SHUIRUPHGZLWKSRO\JDODFWLQVXWXUHPDWHULDOLQDQ interrupted fashion.
$QWHJUDGH--VWHQWLQVHUWLRQ)LJXUH 3ULRUWRFORVLQJWKHDQDVWRPRVLVD)--VWHQWLVLQ serted in an antegrade fashion. The stent with the wire is introduced via the 5 mm port. It is grasped using WKHURERWLFQHHGOHKROGHULQWURGXFHGLQWRWKHXUHWHU and passed down to the bladder.
'UDLQWXEHLQVHUWLRQ7KHURERWLVXQGRFNHG DQGDGUDLQWXEHLVLQVHUWHGYLDWKHPPSRUW7KH mm port is closed in standard fashion and an indwell ing catheter is left in situ.
Figure 7 – Antegrade JJ stent insertion. Figure 5 – Transposition of ureter.
RESULTS
This 33 year old female patient was dis charged on postoperative day 3. The catheter and drain tube were removed on day 1. The JJ stent was UHPRYHGDWZHHNVSRVWRSHUDWLYHO\7KHSRVWRSHUD WLYH,98DWPRQWKVFRQ¿UPHGQRUPDOGUDLQDJHRI FRQWUDVW)LJXUH
COMMENTS
Robotic technology has become incorporated into certain areas of urology as in robotic prostatec tomy and has become well accepted. Reconstructive urology represents a challenge for the robotic urolo JLVWWRRIIHUWKLVWHFKQRORJ\VDIHO\ZLWKHI¿FDF\RYHU proven techniques and without increased morbidity.
Our case demonstrates the feasibility of a procedure using the robot but does not necessarily justify its use over other modalities. Though the fun GDPHQWDOVXUJLFDOSULQFLSOHVRIDWHQVLRQIUHHZHOO YDVFXODUL]HGDQDVWDPRVLVUHPDLQWKHVDPHSDWLHQWV PD\QRZUHFHLYHWKHEHQH¿WVRIDPLQLPDOO\LQYDVLYH DSSURDFKQDPHO\VPDOOHULQFLVLRQEHWWHUFRVPHWLF HIIHFW GHFUHDVHG SDLQ VKRUWHU KRVSLWDO VWD\ DQG D TXLFNHUUHWXUQWRQRUPDODFWLYLWLHV7KLVKROGVWUXHIRU both a pure laparoscopic or pure robotic approach.
Pure laparoscopic repair of the retrocaval ureter has been performed both transperitoneally and UHWURSHULWRQHDOO\:HKDYHSUHYLRXVO\SXEOLVKHG our results with retroperitoneal ureterolysis and ret URFDYDO XUHWHU UHSDLU 3XUH ODSDURVFRSLF UHSDLU UHPDLQVDWHFKQLFDOO\FKDOOHQJLQJSURFHGXUHEXWLQ H[SHUWVKDQGVWKHUHVXOWVDUHH[FHOOHQW
The robotic approach to retrocaval ureter was ¿UVWSXEOLVKHGIRUDSHGLDWULFSDWLHQWE\*XQGHWLHW DOLQ3\HORS\HORVWRP\ZLWKSUHVHUYDWLRQ RIWKHUHWURFDYDOVHJPHQWZDV¿UVWSHUIRUPHGIRUD UHWURFDYDOXUHWHUE\6LP¿URRVKHWDOLQLQDSXUH ODSDURVFRSLFSURFHGXUH7KLVSUHVHUYDWLRQRIWKH retrocaval segment does not appear to hinder drainage DQGLWPDNHVWKHDQDVWDPRVLVIDUHDVLHUWRSHUIRUPDQG may lead to a lower stricture rate.
The main advantage of the robotic technology is the ease of dissection and intracorporeal suturing. ([SHUWODSDURVFRSLFVXUJHRQVPD\DUJXHWKDWWKHUHLV
no need for the robot in such a procedure in the same way that laparoscopic pyeloplasty can be done with RXWWKHURERW7KLVRIFRXUVHLVWUXHKRZHYHUWKHIDFW remains that new technologies emerge and it seems that robotic technology is here to stay. The downside to the robotic approach is of course the cost.
6LQFHDFTXLULQJWKHGD9LQFL6URERWLQ we have performed many reconstructive procedures such as megaureter repair and pyeloplasty with robotic DVVLVWDQFH7KLVLVWKH¿UVWUHWURFDYDOXUHWHUUHSDLUWKDW we have performed using the robot.
CONCLUSION
We demonstrated in this case that pure ro botic retrocaval ureter repair is feasible. Apart from WKHHUJRQRPLFDQGWHFKQLFDOEHQH¿WVWKDWWKHURERWLF DSSURDFKJLYHVWKHVXUJHRQWKHUHGRHVQRWDSSHDUWR be any other advantage over laparoscopy.
CONFLICT OF INTEREST
REFERENCES
$QGHUVRQ -& +\QHV: 5HWURFDYDO XUHWHU D FDVH GLDJQRVHGSUHRSHUDWLYHO\DQGWUHDWHGVXFFHVVIXOO\E\ DSODVWLFRSHUDWLRQ%U-8URO 0DWVXGD7<DVXPRWR 57VXMLQR7 /DSDURVFRSLF
WUHDWPHQWRIDUHWURFDYDOXUHWHU(XU8URO
*XSWD13+HPDO$.6LQJK,.KDLWDQ$5HWURSHULWR
neoscopic ureterolysis and reconstruction of retrocaval
XUHWHU-(QGRXURO
*XQGHWL06'XII\3*0XVKWDT,5RERWLFDVVLVWHG
laparoscopic correction of pediatric retrocaval ureter.
-/DSDURHQGRVF$GY6XUJ7HFK$ 6LPIRURRVK11RXUL0DKGDYL.7DELEL$/DSDUR
scopic pyelopyelostomy for retrocaval ureter without
H[FLVLRQRIWKHUHWURFDYDOVHJPHQW¿UVWUHSRUWRI FDVHV-8UROGLVFXVVLRQ
Accepted after revision: August 28, 2008
Correspondence address: 'U$VKRN.+HPDO 'HSDUWPHQWRI8URORJ\
:DNH)RUHVW8QLYHUVLW\6FKRRORI0HGLFLQH
Medical Center Boulevard
:LQVWRQ6DOHP1&86$ )D[