Abst ract
Submitted: December 30, 2016 Accepted: December 31, 2016
Oral cancer st em cells - propert ies
and consequences
5HVHDUFKRQFDQFHUVWHPFHOOV&6&VKDVJUHDWO\LQFUHDVHGLQWKH¿HOG
of m edicine and pat hology; how ever, som e concept ual m isunderst andings
DUHVWLOOSUHVHQWDPRQJWKHSXEOLFDVZHOODVZLWKLQWKHJHQHUDOVFLHQWL¿F FRPPXQLW\WKDWLVQRW\HWIDPLOLDUZLWKWKHVXEMHFW7KHYHU\¿UVWSUREOHP
is t he m isint erpret at ion of CSCs as a synonym of t heir norm al count erpart s, t he w ell- know n st em cells ( SCs) . Part icularly in Dent ist ry, anot her com m on m ist ake is t he m isint erpret at ion of oral CSCs as norm al t oot h- derived SCs. The present review aim s t o clarify im port ant concept s relat ed t o norm al SCs and CSCs, as w ell as discuss t he relevance of CSCs t o t he developm ent , m et ast asis and t herapy resist ance of oral squam ous cell carcinom a.
K e y w o r d s: Neo p l ast i c st em cel l s. Mo u t h n eo p l asm s. Ep i t h el i al -m esenchy-m al t ransit ion. Neoplas-m -m et ast asis. Squa-m ous cell carcino-m a. Camila Oliveira RODINI1
Nathália Martins LOPES1
Vanessa Soares LARA2
Ian Campbell MACKENZIE3
http://dx.doi.org/10.1590/1678-7757-2016-0665
1Universidade de São Paulo, Faculdade de Odontologia de Bauru, Departamento de Ciências
Biológicas, Bauru, SP, Brasil.
2Universidade de São Paulo, Faculdade de Odontologia de Bauru, Departamento de Cirurgia,
Estomatologia, Patologia e Radiologia. Bauru, SP, Brasil.
3Queen Mary University of London, Blizard Institute - Barts and The London School of Medicine and
Dentistry, London, United Kingdom.
I nt roduct ion
For several years t he concept of “ st em cells” has EHHQRIJHQHUDOVFLHQWL¿FLQWHUHVWDQGKDVUDLVHGWKH im port ant prospect of being able t o creat e new hum an
t issues in t he laborat ory and use t hem t o replace t hose
lost by inj ur y or disease. Such st em cell concept s
applied t o Dent ist ry, as w ell as t o general Medicine,
could be great ly enhanced by researches exploring t he
abilit y of st em cells t o generat e new t issues such as
m ucosa and bone t issues and, event ually, regenerat e
dent al t issues including perhaps even t he whole t eet h.
Recent ly, how ever, t he dent al lit erat ure has begun t o
cont ain references t o “ cancer st em cells” ( CSCs) and
t hese have quit e a different concept . These are t he
cells t hat have t he abilit y t o st im ulat e t he grow t h of
oral cancers and enable t um ours t o resist t herapy. This
review will describe how CSCs differ from norm al st em
cells, how t hey can be isolat ed and st udied, how t hey
have special propert ies and, of m ost im port ance, how
t hey are responsible for t he spreading of cancer and
how t hey m ight be t arget ed for dest ruct ion. There is
now good evidence t hat CSCs exist in m ost t um ours
but t his review w ill focus m ainly on oral squam ous
cell carcinom a, w hich com prises t he great m aj orit y
of m alignant oral cancers.
Background of oral cancer
Or al sq u am ou s cell car cin om a ( OSCC) is t h e
m ost com m only occurring oral m alignancy and one
of t h e m ost w idely occu r r in g can cer s t h r ou gh ou t
t he w orld9,25,33. OSCC is a m alignancy t hat arises in
t he squam ous epit helium lining t he oral cavit y and
includes t um ours found on t he t ongue, lip, gingival, SDODWHÀRRURIWKHPRXWKDQGEXFFDOPXFRVD13,25. The
risk fact ors for developm ent of OSCC include t obacco
ex posur e, alcohol consum pt ion, and infect ion w it h
oncogenic viruses such as HPV9,35. The t um our can
invade deeply int o adj acent t issues of t he t ongue and WKHÀRRURIWKHPRXWKDVZHOODVLQWRERQHVSULPDULO\ of t he alveolar crest41.
Micr oscop ically, OSCC u su ally sh ow s v ar iab le
d e g r e e s o f k e r a t i n i za t i o n , ce l l u l a r a n d n u cl e a r
pleom orphism , and m it ot ic act ivit y. They are graded
as w ell- , m oderat ely- or poorly- different iat ed ( grades
1 t o 3) according t o WHO crit eria23,43. The t um our ’s
feat ures, including size and sit e, hist ologic m alignant
g r a d e, p er i n eu r a l sp r ea d a t t h e i n v a si v e f r o n t ,
lym phovascular invasion and t um our t hickness, can
DFW DV PDMRU ULVN IDFWRUV LQÀXHQFLQJ WKH SURJQRVLV f or OSCC pat ien t s3 2; h ow ev er, t h e m ain n egat iv e
p r og n ost ic f act or is t h e p r esen ce of ly m p h n od e
m et ast asis, w hich occurs in 25 t o 65% of cases15,29.
The t reat m ent for early- st age OSCC is generally
single m odalit y, eit her sur ger y or radiot herapy. I n
cases of locally advanced OSCC, t he t r eat m ent is
m ult im odal, w it h eit her surgery follow ed by adj uvant
r a d i a t i o n o r ch e m o - r a d i a t i o n , a s i n d i ca t e d b y SDWKRORJLF IHDWXUHV RU GH¿QLWLYH FKHPRUDGLDWLRQ27.
Approxim at ely half of all pat ient s survive 5 years aft er WUHDWPHQW DQG VXUYLYDO LV KHDYLO\ LQÀXHQFHG E\ WKH st age of t he disease at diagnosis35.
The various t ypes of norm al st em cells
The general t er m “ st em cells” includes sev eral GLIIHUHQWW\SHVRIFHOOVDQGWKH¿UVWGLVWLQFWLRQWREH m ade is bet w een ( a) norm al st em cells ( SC) , w hich
are responsible for t he developm ent and m aint enance
of all of t he t issues of t he body, and ( b) t heir diseased
count erpart , called cancer st em cells ( CSC) , t hat have
lost t he close gr ow t h cont r ol t hat is a pr oper t y of
norm al st em cells. The m ost prim it ive t ype of st em FHOOLVWKHIHUWLOL]HGHJJDQGLWV¿UVWIHZGLYLVLRQVHDUO\ in developm ent produce cells t hat ret ain t he abilit y t o
generat e all t he different cell t ypes of t he adult body.
They ar e t her efor e descr ibed as “ t ot ipot ent ” and,
unusually for st em cells, t hey are t ransient . As t he
em br yonic developm ent pr oceeds, t hese t ot ipot ent
st em cells becom e direct ed t owards different iat ion int o
t he m any dist inct t issue t ypes of t he adult individual
( e.g. st em cells for blood, bones, m ucosa, et c.) . As t hey
do so t hey lose som e of t heir developm ent al pot ent ial
and becom e eit her “ pluripot ent ”, t hat is, rest rict ed t o
form ing only a few t ypes of t issues, or " unipot ent " ,
rest rict ed t o generat ing only a single t issue. Thus,
several subt ypes of st em cells exist in adult individuals,
each w it h different pot ent ialit ies depending on t heir
developm ent al hist ory. The epit helial st em cells of oral
m ucosal epit helia are t ypically unipot ent and form only
t he t ype of epit helium t ypical of t he region where t hey
are found ( Figure 1) .
Th e g en er al p r op er t y t h at ch ar act er izes ad u lt
( som at ic) st em cells is t h at t h ey can be div ided LQGH¿QLWHO\QRUPDOO\SURGXFLQJRQHFHOOWKDWUHPDLQV a st em cell and one cell t hat different iat es it self int o
a funct ional t issue cell. This norm al “ asym m et rical”
d iv ision p at t er n is im p or t an t as it r esu lt s in t h e
w hile also providing anot her cell for t issue funct ion.
How ever, w hen it is necessary t o replace st em cells,
such as t hose lost aft er w ounding, st em cells can be
divided “ sym m et rically” t o form t w o st em cells and
t hus increase t heir num ber.
Experim ent ally derived st em cells
Al t h ou g h n or m al ad u l t st em cel l s can d i v i d e
t h em selv es t o r egen erat e t issu es t h r ou gh ou t life, WKH\FDQEHGLI¿FXOWWRJURZIRUDORQJSHULRGLQWKH laborat or y. How ever, t ot ipot ent cells t aken ear ly in
em bryonic developm ent have been shown t o cont inue GLYLGHWKHPVHOYHVLQGH¿QLWHO\LQWLVVXHFXOWXUHZLWKRXW losing t heir t ot ipot ent abilit ies. For t his w ork, Mart in
Evans and colleagues w ere awarded t he Nobel Prize
in 2 0 0 7 , r ecog n izin g t h e g r eat p ot en t ial of su ch
“ em br yonic st em cells” t o allow new t issues t o be
r egen er at ed in t h e labor at or y. Fu r t h er st u dies on
t he genes expressed by em bryonic st em cells have LGHQWL¿HGJHQHVWKDWDUHUHVSRQVLEOHIRUPDLQWDLQLQJ “ st em ness” and t his led t o anot her m aj or st ep. I t was IRXQGWKDWZKHQVXFKJHQHVDUHDUWL¿FLDOO\H[SUHVVHGLQ adult st em cells t hey regain t he t ot ipot ent propert ies of
em bryonic st em cells. For his work wit h t hese “ induced
plu r ipot en t st em cells ( iPSCs) , Sh iny a Yam an ak a
ZDVDZDUGHGWKH1REHO3UL]HLQ7KHVH¿QGLQJV DUH LPSRUWDQW PDLQO\ WR WKH ¿HOGV RI 5HJHQHUDWLYH Medicine and Tissue Bioengineer ing. How ever, t his
w ork also show s t hat alt hough adult st em cells are
norm ally rest rict ed perm anent ly t o a part icular t issue
t ype, t hey can be m anipulat ed experim ent ally t o form
different cell t ypes ( Figure 1) . Such cell plast icit y is
also of int erest t o cancer developm ent , progression
and m et ast asis. Thus, st em cell r esear ch now has
t w o differ ent dir ect ions: ( a) how t o encourage t he
gr ow t h and differ ent iat ion of st em cells for t issue
regenerat ion, and ( b) how t o prevent t he grow t h of
cancer st em cells t o prevent t he expansion, m et ast asis
and recurrence of t he t um ours in which t hey are found.
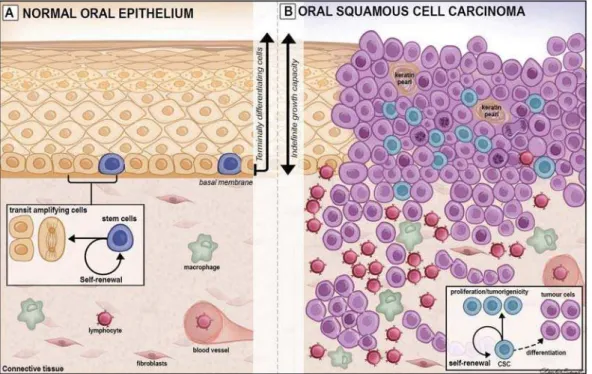
Norm al oral epit helium and oral cancer
1RUPDO RUDO PXFRVD LV FRYHUHG E\ D VWUDWL¿HG squ am ou s epit h eliu m an d alt h ou gh k er at in ocy t es
f or m t h e p r im ar y cell t y p e of t h e t issu e, t h ese
epit h elia also con t ain a m in or it y of cells su ch as
m elan ocy t es, Lan ger h an s cells, Mer k el cells, an d WUDQVLHQW LQÀDPPDWRU\ FHOOV 6RPH UHJLRQV RI WKH PRXWK KDYH D NHUDWLQLHG RU FRUQL¿HG VXUIDFH OD\HU t hat is able t o resist t he forces of m ast icat ion, but
ot her regions, w here t he epit helium act s as a lining
Figure 1- Schematic view of normal stem cells (A) and cancer stem cells (B). A shows different sources of normal SCs, their biological
SURSHUWLHVRILQGH¿QLWHGLYLVLRQWKURXJKVHOIUHQHZDODQGJHQHUDWLRQRIGLIIHUHQWLDWHGFHOOVXQGHUDSSURSULDWHFRQGLWLRQVZKLOHHPEU\RQLF
t hat is r equir ed t o st r et ch, hav e a non- k erat inied
epit helium . Oral epit helia are form ed of a num ber of
cell st rat a know n as t he basal, spinous, granular and
corneal layers in kerat inized regions, and as basal, VSLQRXVLQWHUPHGLDWHDQGVXSHU¿FLDOOD\HUVLQQRQ kerat inized regions. I n all regions, cell proliferat ion
occur s in t he basal cell layer t o pr ov ide new cells
t hat undergo different iat ion as t hey m ove upwards
t hrough t he st rat a and t he whole epit helial com ponent
of t he m ucosa is renew ed in 5- 40 days depending on
t he region. The rapid t issue renewal t hat confers a
rem arkable regenerat ive pot ent ial t o t he oral m ucosa
is ult im at ely relat ed t o t he presence and dynam ics of
t he epit helial st em cells ( eSC) present in t he basal cell
layer. The carefully ordered st ruct ure and balanced cell
renewal found in norm al oral m ucosa is progressively
lost w it h t he developm ent of cancer.
I t was originally t hought t hat all epit helial basal
cells are sim ilar and all divide t hem selves t o produce
cells t hat are com m it t ed t o different iat ion as a result
of being random ly squeezed out of t he basal layer
by populat ion pressure. How ever, m easurem ent s of
regional differences in proliferat ion rat es, and of t he cell
lineages produced by labelled cells, indicat e t hat only
a sm all fract ion of t he proliferat ing cells have t he st em SURSHUW\RILQGH¿QLWHGLYLVLRQ7KHSUHVHQWFRQFHSWLV t hat such st em cells form only a sm all fract ion of t he
t ot al dividing cells and t hat t hey divide quit e slow ly
t o produce cells com m it t ed t o different iat ion. These
different iat ing “ t ransit - am plifying” ( TA) cells have a
high proliferat ive rat e but a low self- renewal capacit y,
so t hey event ually different iat e int o specialized cells
t hat st op dividing and fully different iat e t hem selves11,12
( Figure 2) .
Such cell proliferat ion is fundam ent al for epit helial
renewal but it requires t ight ly cont rolled m echanism s
t hat balance epit helial cell product ion and loss. The
loss of such balance can be result ed from t he increased
or decreased expression of genes ( prot o- oncogenes
and t heir opposit e, t um our suppressor genes) relat ed
t o t he cont rol of t he cell cycle and deat h. Accum ulat ion
of som at ic m ut at ions m ay alt er t he expression pat t ern
of genes involved in t he cont rol of cell grow t h and
dif f er en t iat ion leadin g t o t h e loss of pr olif er at iv e
cont rol t hat charact erizes cancer. Such m ut at ions arise
as a result of long- t erm exposure t o carcinogens such
as t obacco and alcohol ( Figures 1B and 2) .
Oral cancer st em cells
As st em cells ar e ult im at ely r esponsible for all
t he norm al t issue grow t h and renewal occurring in
t he body, it t herefore logically follow s t hat st em cells
are also likely t o be responsible for cancer grow t h.
How ever, alt hough t he idea t hat CSCs st im ulat e t he
Figure 2- Schematic view of normal oral epithelium (A) and oral squamous cell carcinoma (B). In A, the asymmetric division of normal stem cells (SCs) found in the basal cell layer generates one daughter SC (self-renewal) and one daughter transit-amplifying cell committed to differentiation (small black box). In B, loss of balance of genes related to cell growth and death due to cumulative somatic mutations on SCs results on the development of cancer stem cells (CSCs), which retain the biological properties of self-renewal and generation of
GLIIHUHQWLDWHGWXPRXUFHOOVVPDOOEODFNER[7KHVH&6&SURSHUWLHVUHÀHFWWKHLQGH¿QLWHJURZWKFDSDFLW\DQGPRUSKRORJ\KHWHURJHQHLW\
grow t h and spread of t um ours has been discussed for
m any years, t heir exist ence has also been quest ioned.
I t m ight be t hought t hat w it h t he loss of proliferat ive
cont r ol and spat ial or ganizat ion, t he nor m al st em
cell pat t erns w ould disappear. From w hat has been
described above, it can be seen t hat if all dividing cells
of a t um our have equal proliferat ive abilit ies t hey can
all be considered st em cells and a sub- populat ion of VWHPFHOOVZRXOGQRWH[LVW7KHH[SHULPHQWDOGLI¿FXOW\ LQWHVWLQJWKLVKDVEHHQWR¿QGJRRGPDUNHUVIRUVWHP cells and t o t est w het her init iat ion and m aint enance
of t um ours is rest rict ed t o t he sub- populat ion of t he FHOOV LGHQWL¿HG 7KH ¿UVW H[SHULPHQWDO HYLGHQFH IRU t he exist ence of such t um our- init iat ing st em cells was
provided in 1997, w hen Bonnet & Dick found t hat only
t he sm all subpopulat ion of leukem ic cells, m ar ked
by st aining, posit ively for CD34 and negat ively for
CD38, was able t o regenerat e t he original leukaem ia
w h en t r an sp l an t ed i n t o i m m u n o d ef i ci en t m i ce5. 6XEVHTXHQWO\&6&VZHUHLGHQWL¿HGLQVROLGWXPRXUV by Al- Haj j and co- w orkers w ho report ed in 2003 t hat
only a subpopulat ion of breast cancer cells st aining,
posit ively for CD44 and negat ively for CD24, could
re-init iat e t um ours wit h t he cellular het erogeneit y t ypical
of t he original t um our1. Since t hen, increasing evidence
for t he presence of such cells has been found for m any
t um ours including t hose of t he cent ral nervous syst em ,
breast , prost at e and pancreas22,31,39.
Many evidences t hat CSCs also play a cent ral role
in t he pat hogenesis and progression of carcinom as
of t h e h ead an d n eck ( HNSCC) , in clu din g OSCC,
have been found. Early t issue cult ure st udies show ed
t hat only a subpopulat ion of OSCC cells can for m
expanding t um our colonies, suggest ing t hat hum an
OSCC m ay cont ain som e form of st em cells24 and it was
subsequent ly show n t hat only a sm all subpopulat ion
of t he cells in OSCC corresponds t o t um our- init iat ing
cells26,467KHVH¿QGLQJVDUHLQDFFRUGDQFHZLWKWKH&6&
concept17,34 t hat t he t um our m ass is a m ixt ure of ( a)
CSCs dividing t hem selves t o feed t he t um our ’s growt h,
( b) t ransient am plifying cells t hat divide t hem selves
a few t im es before m at uring int o ( c) different iat ed
t um our cells t hat do not cont ribut e t o t um our growt h4.
The isolat ion of CSCs from oral cancers has m ainly
been per f or m ed w it h t h e CD4 4 m ar k er t h at w as
init ially used t o isolat e breast cancer CSCs. CD44 is
an adhesion m olecule t hat binds it self t o hyaluronan
and it s expression is necessary for t he m aint enance
of t he CSC’s propert ies. CSCs lose t heir “ st em ness”
w hen CD44 is ex per im ent ally r educed44. How ev er,
a problem w it h CD44, and also w it h all ot her CSC PDUNHUVWKDWKDYHEHHQLGHQWL¿HGVRIDULVWKDWWKH\ DUHQRWHQWLUHO\VSHFL¿F1RVLQJOHPDUNHULVFDSDEOH RIVSHFL¿FDOO\UHFRJQL]LQJ&6&VDQGDGGLWLRQDOPDUNHUV
Figure 3- Schematic view of the primary site of oral squamous cell carcinoma (A) and metastatic lymph node (B). In A, cancer stem cells
&6&VURXQGEOXHFHOOVXQGHUJR(07(07&6&VXQGHUWKHLQÀXHQFHRIPROHFXOHVVXFKDV7*)ȕ,/71)ĮIURPWKHWXPRXU¶V
microenvironment, assuming a complete mesenchymal (CD44highESAlow/-ALDH-) or epithelial-mesenchymal (CD44highESAlow/+ALDH+)
have t herefore been sought . ALDH1 is an int racellular HQ]\PHLQYROYHGLQGHWR[L¿FDWLRQDQGGUXJUHVLVWDQFH via t he oxidat ion of aldehydes, and ALDH- posit ive cells
in HNSCC are report ed t o have t ypical CSC behavior
and increased t um origenic abilit y21. The com binat ion
of CD44 w it h ot her m ar ker s, such as ALDH1, m ay
im p r ov e t h e sp ecif icit y of CSCs’ r ecog n it ion an d
isolat ion.
Cancer st em cells and t reat m ent failure
As t hey are t he cells st im ulat ing t um our grow t h,elim inat ion of CSCs is necessary for t he elim inat ion
of t um ours. How ever, m any st udies have now show n
t hat CSCs are m ore resist ant t han ot her t um our cells
t o chem ot herapy and radiot herapy7. I n v it r o assays
show t hat w hen CD44- high CSCs ar e ir radiat ed or
exposed t o chem ot herapy, t hey m ay be over 10 t im es
m or e r esist ant t o apopt osis t han CD44- low cells18.
The sensit ivit y of surrounding norm al t issues t o high
doses of chem o- and radio- t herapies r est r ict s t he
dose levels t hat can be adm inist ered and, despit e t he
various m et hods of t arget ing, t he dose provided m ay EHVXI¿FLHQWWRNLOOPDQ\WXPRXUFHOOVEXWQRWDOORI t he CSCs. Clinically, t herefore, t he t um our m ay appear
t o shrink, and even perhaps disappear, only for a few
rem aining CSCs t o begin t o divide and subsequent ly
r egenerat e it . Local t um our r ecur r ence is a m aj or
problem for OSCC t herapy and elim inat ion of CSCs is
a t arget of t herapy but one t hat is m ade m ore com plex
by t he het erogeneit y of CSCs as discussed below.
Epit helial t o m esenchym al t ransit ion
The epit helial t o m esenchy m al t ransit ion ( EMT) ZDV ¿UVW UHFRJQL]HG DV D IHDWXUH RI HPEU\RJHQHVLV but it is also act ivat ed dur ing w ound healing and
o r g an f i b r o si s4 0. Recen t ev i d en ce i n d i cat es t h at
genet ic program s relevant for EMT are also act ivat ed
in epit helial cancer s and t hat t he changes induced
in cancer cells by EMT appears t o play a cent ral role
in cancer pr ogr ession and m et ast asis8,19. Epit helial FHOOV DUH QRUPDOO\ DWWDFKHG ¿UPO\ WR WKH EDVHPHQW m em brane and adj acent cells, but EMT allow s t hem
t o a cq u i r e a m esen ch y m a l cel l p h en o t y p e t h a t
is m igr at or y an d inv asiv e, an d also h as elev at ed
r esi st a n ce t o a p o p t o si s1 9 , 2 0. Th ese ch a n g es a r e
charact erized by t he dow n- regulat ion of E- cadherin, WUDQVORFDWLRQ RI ǃFDWHQLQ IURP WKH FHOO PHPEUDQH t o t he nucleus, and up- r egulat ion of m esenchym al
m olecu lar m ar k er s su ch as v im en t in , f ib r on ect in
and N- cadherin28,36,42. There is also up- regulat ion of
t ranscript ion fact ors such as SNAI L, TWI ST, and LEF- 1
t hat prom ot e EMT14,45.
Met ast asis is a m aj or t h er apeu t ic pr oblem f or
OSCC and t he presence of lym ph node m et ast asis is a
st rong predict or of t herapeut ic failure. For m et ast asis
of OSCC t o occur, cells of t he prim ary t um our need
t o undergo EMT, invade t he surrounding t issue, gain
access t o lym phat ic or blood vessels, and t hen survive
t ransport t o exit from vessels and invade a new t issue
sit e38. Through t he reverse process of m esenchym
al-t o- epial-t helial al-t ransial-t ion ( MET) , al-t he cells al-t hen al-t ransial-t ion
back t o t he proliferat ive epit helial phenot ype t o form
secondary t um ours6. Applying t his t o t he cancer st em
cell concept suggest s t hat CSCs can ex ist as t w o
int erchangeable populat ions and Biddle, et al.3 ( 2011) FRQ¿UPHGWKDW&6&VIRUPDG\QDPLFFHOOSRSXODWLRQ t hat uses EMT and MET t o sw it ch back w ar ds and
forwards bet w een a proliferat ive epit helial phenot ype
( EPI - CSC; CD44highESAlow / +ALDH+) and a m igrat or y
m esenchym al phenot ype ( EMT- CSC; CD44highESAlow /
-ALDH-) ( Figur e 3) . Of par t icular int er est , EMT not
on ly en ab les cell m ig r at ion b u t also alt er s d r u g
sensit ivit ies so t hat EPI - CSCs and EMT CSCs respond
quit e different ly t o chem o- and radio- t herapies2,3,16.
Fut ure t reat m ent perspect ives
Su r g ical r esect ion is st ill a m aj or t h er ap y f or
OSCC and is effect ive, especially in t reat ing sm aller
lesion s3 0. Cu r r en t an t i- can cer t h er ap ies f or m or e
advanced lesions are t ypically based on radio- and
chem o- t herapeut ic agent s t hat t ar get pr oliferat iv e
can cer cells2 7. How ev er, com par ed t o t h e bu lk of
t um our cells, t he resist ance of EPI - CSC populat ions
t o such t herapies is gr eat ly enhanced due t o t heir
slow cell cycle and t heir m echanism s for rapid DNA
repair and drug exclusion37. Consequent ly, alt hough
m ost non- CSC t um our cells m ay be eradicat ed w it h
st andard t herapies, t he t herapy resist ant CSCs m ay
select ively survive t he doses of radi and chem
o-t herapies o-t hao-t are achievable w io-t houo-t m aj or dam ages
t o t h e su r r ou n din g n or m al st r u ct u r es. Wit h su ch
part ially effect ive t herapies, CSCs can be expect ed t o
survive t hrough a process sim ilar t o nat ural select ion,
and t heir self- renewal capacit y can t hen enable t hem
t o regenerat e t hem selves and st im ulat e t he grow t h
of a new t um our. To avoid such recurrence, t herapy
t herefore needs t o em ploy agent s, or com binat ions
of agent s, w hich pr ov ide w idely effect iv e act ions,
effect iv e scr eening of new and ex ist ing dr ugs for
t heir different ial effect s on all sub- t ypes of CSCs and
non- CSCs.
The m olecular advances in t um our biology st udies
are guiding an individualized t reat m ent approach. For
exam ple, a clinically validat ed chem o- predict ive assay
( Chem oI D®) is now being t est ed for HNSCC, in w hich
bot h CSCs and bulk t um our cells are challenged by
various FDA- approved drugs and t heir com binat ions
t o d et er m i n e t h e m o st ef f ect i v e ch em o t h er a p y
schem e. This assay, alt hough st ill not FDA- approved,
w as r ecen t ly pu blish ed as a n ew com plem en t ar y
procedure t o HNSCC drug t reat m ent , aim ing at bot h
t he elim inat ion of unnecessary t oxicit y in pat ient s as
well as avoiding ineffect ive chem ot herapy regim ens10.
A bet t er underst anding of CSC propert ies is crucial
for t he developm ent of effect ive alt ernat ive st rat egies,
f o r ex a m p l e, t a r g et i n g st em cel l m a i n t en a n ce,
signalling pat hways or blocking EMT/ MET t o prevent
t h e sw i t ch i n g o f CSCs b e t w e e n d r u g r e si st a n t
phenot ypes.
Aknow ledgm ent s
The aut hors would like t o t hank FAPESP ( São Paulo
Resear ch Foundat ion, Grant s # 2 0 1 3 / 0 7 2 4 5 - 9 and IRUWKH¿QDQFLDOVXSSRUWDQG&ODXGLD Biguet t i for providing us w it h Figures 1, 2 and 3.
References
1- Al- Haj j M, Wicha MS, Benit o- Hernandez A, Morrison SJ, Clarke MF.
3URVSHFWLYHLGHQWL¿FDWLRQRIWXPRULJHQLFEUHDVWFDQFHUFHOOV3URF1DWO
Acad Sci U S A. 2003; 100( 7) : 3983- 8.
2- Biddle A, Gam m on L, Liang X, Cost ea DE, Mackenzie I C. Phenot ypic
plast icit y det erm ines cancer st em cell t herapeut ic resist ance in oral
squam ous cell carcinom a. EBioMedicine. 2016; 4: 138- 45.
3- Biddle A, Liang X, Gam m on L, Fazil B, Harper LJ, Em ich H, et al.
Cancer st em cells in squam ous cell carcinom a sw it ch bet w een t w o
dist inct phenot ypes t hat are preferent ially m igrat ory or proliferat ive.
Cancer Res. 2011; 71( 15) : 5317- 26.
4- Blanpain C. Cancer: a disease of st em cells [ I nt ernet ] ? 2015 [ cit ed
2016 Dec 29] . Available from : ht t p: / / www.eurost em cell.org/ fact sheet /
cancer- disease- st em - cells.
5- Bonnet D, Dick JE. Hum an acut e m yeloid leukem ia is organized as
a hierarchy t hat originat es from a prim it ive hem at opoiet ic cell. Nat
Med. 1997; 3( 7) : 730- 7.
6- Brablet z T. EMT and MET in m et ast asis: w here are t he cancer st em
cells? Cancer Cell. 2012; 22( 6) : 699- 701.
7- Chang JC. Cancer st em cells: role in t um or grow t h, recurrence,
m et ast asis, and t reat m ent resist ance. Medicine ( Balt im ore) . 2016; 95( 1
Suppl 1) : S20- 5.
8- Chen C, Wei Y, Hum m el M, Hoffm ann TK, Gr oss M, Kaufm ann
AM, et al. Evidence for epit helial- m esenchym al t ransit ion in cancer
st em cells of head and neck squam ous cell car cinom a. PloS One.
2011; 6( 1) : e16466.
9- Chi AC, Day TA, Neville BW. Oral cavit y and oropharyngeal squam ous
cell carcinom a - an updat e. CA Cancer J Clin. 2015; 65( 5) : 401- 21
10- Cort ese A, Pant aleo G, Am at o M, Law rence L, Mayes V, Brow n
L, et al. A new com plem ent ar y pr ocedur e for pat ient s affect ed by
head and neck cancer: chem o- predict ive assay. I nt J Surg Case Rep.
2016; 26: 42- 6.
1 1 - Cost ea DE, Gam m on L, Kit aj im a K, Har per L, Mack enzie I C.
Epit helial st em cells and m alignancy. J Anat . 2008; 213( 1) : 45- 51.
1 2 - Cost ea DE, Tsin k alov sk y O, Vin t er m y r OK, Joh an n essen AC,
Mackenzie I C. Cancer st em cells - new and pot ent ially im por t ant
t arget s for t he t herapy of oral squam ous cell carcinom a. Oral Dis.
2006; 12( 5) : 443- 54.
13- Est ilo CL, O- charoenrat P, Talbot S, Socci ND, Carlson DL, Ghossein
5HWDO2UDOWRQJXHFDQFHUJHQHH[SUHVVLRQSUR¿OLQJLGHQWL¿FDWLRQRI
novel pot ent ial prognost icat ors by oligonucleot ide m icroarray analysis.
BMC Cancer. 2009; 9: 11.
14- Fan F, Sam uel S, Evans KW, Lu J, Xia L, Zhou Y, et al. Overexpression
of snail induces epit helial- m esenchym al t ransit ion and a cancer st em
cell- like phenot y pe in hum an color ect al cancer cells. Cancer Med.
2012; 1( 1) : 5- 16.
1 5 - Fer lit o A, Rin aldo A, Dev an ey KO, MacLen n an K, My er s JN,
Pet r u zzelli GJ, et al. Pr og n ost ic sig n if ican ce of m icr oscop ic an d
m acroscopic ext racapsular spread from m et ast at ic t um or in t he cervical
lym ph nodes. Oral Oncol. 2002; 38( 8) : 747- 51.
16- Gem enet zidis E, Gam m on L, Biddle A, Em ich H, Mackenzie I C.
I nvasive oral cancer st em cells display resist ance t o ionising radiat ion.
Oncot arget . 2015; 6( 41) : 43964- 77.
17- Hanahan D, Weinberg RA. Hallm arks of cancer: t he next generat ion.
Cell. 2011; 144( 5) : 646- 74.
18- Harper LJ, Piper K, Com m on J, Fort une F, Mackenzie I C. St em
cell pat t erns in cell lines derived from head and neck squam ous cell
carcinom a. J Oral Pat hol Med. 2007; 36( 10) : 594- 603.
19- Kallur i R, Weinber g RA. The basics of epit helial- m esenchy m al
t ransit ion. J Clin I nvest . 2009; 119( 6) : 1420- 8.
20- Kong D, Li Y, Wang Z, Sarkar FH. Cancer st em cells and epit
helial-t o- m esenchym al helial-t ransihelial-t ion ( EMT) - phenohelial-t ypic cells: are helial-t hey cousins
or t w ins? Cancers ( Basel) . 2011; 3( 1) : 716- 29.
21- Krishnam urt hy S, Nör JE. Head and neck cancer st em cells. J Dent
Res. 2012; 91( 4) : 334- 40.
2 2 - Li C, Heidt DG, Daler ba P, Bu r an t CF, Zh an g L, Adsay V, et
al. I d en t if icat ion of p an cr eat ic can cer st em cells. Can cer Res.
2007; 67( 3) : 1030- 7.
23- Lindenblat t RC, Mart inez GL, Silva LE, Faria PS, Cam isasca DR,
Lourenço SQ. Oral squam ous cell carcinom a grading syst em s - analysis
of t he best survival predict or. J Oral Pat hol Med. 2012; 41( 1) : 34- 9.
24- Mackenzie I C. Grow t h of m alignant oral epit helial st em cells aft er
seeding int o organot ypical cult ures of norm al m ucosa. J Oral Pat hol
Med. 2004; 33( 2) : 71- 8.
25- Malik UU, Zarina S, Penningt on SR. Oral squam ous cell carcinom a:
key clinical quest ions, biom arker discovery, and t he role of prot eom ics.
Arch Oral Biol. 2016; 63: 53- 65.
26- Mannelli G, Gallo O. Cancer st em cells hypot hesis and st em cells
in head and neck cancers. Cancer Treat Rev. 2012; 38( 5) : 515- 39.
27- Marur S, Forast iere AA. Head and neck squam ous cell carcinom a:
updat e on epidem iology, diagnosis, and t reat m ent . Mayo Clin Proc.
2016; 91( 3) : 386- 96.
28- Nij kam p MM, Span PN, Hoogst een I J, van der Kogel AJ, Kaanders
JH, Bussink J. Expression of E- cadherin and vim ent in correlat es w it h
m et ast asis for m at ion in head and neck squam ous cell car cinom a
29- Okada Y, Mat aga I , Kat agiri M, I shii K. An analysis of cervical
lym ph nodes m et ast asis in oral squam ous cell carcinom a. Relat ionship
bet w een grade of hist opat hological m alignancy and ly m ph nodes
m et ast asis. I nt J Oral Maxillofac Surg. 2003; 32( 3) : 284- 8.
30- Om ura K. Cur r ent st at us of oral cancer t r eat m ent st rat egies:
surgical t reat m ent s for oral squam ous cell carcinom a. I nt J Clin Oncol.
2014; 19( 3) : 423- 30.
31- Pat rawala L, Calhoun T, Schneider- Broussard R, Li H, Bhat ia B, Tang
6HWDO+LJKO\SXUL¿HG&'SURVWDWHFDQFHUFHOOVIURP[HQRJUDIW
hum an t um ors are enriched in t um origenic and m et ast at ic progenit or
cells. Oncogene. 2006; 25( 12) : 1696- 708.
3 2 - Per eir a MC, Oliv eir a DT, Lan dm an G, Kow alsk i LP. Hist ologic
subt ypes of oral squam ous cell carcinom a: prognost ic relevance. J Can
Dent Assoc. 2007; 73( 4) : 339- 44.
33- Pet ersen PE. Oral cancer prevent ion and cont rol - t he approach
of t he World Healt h Organizat ion. Oral Oncol. 2009; 45( 4- 5) : 454- 60.
34- Reya T, Morrison SJ, Clarke MF, Weissm an I L. St em cells, cancer,
and cancer st em cells. Nat ure. 2001; 414( 6859) : 105- 11.
3 5 - Rh o d u s NL, Ke r r AR, Pa t e l K. Or a l ca n ce r : l e u k o p l a k i a ,
prem alignancy, and squam ous cell carcinom a. Dent Clin Nort h Am .
2014; 58( 2) : 315- 40.
36- Scanlon CS, Van Tubergen EA, I nglehart RC, D'Silva NJ. Biom arkers
of epit helial- m esenchym al t ransit ion in squam ous cell carcinom a. J
Dent Res. 2013; 92( 2) : 114- 21.
6FKDWWRQ7)UDQN1<)UDQN0+,GHQWL¿FDWLRQDQGWDUJHWLQJRI
cancer st em cells. Bioessays. 2009; 31( 10) : 1038- 49.
3 8 - Sch eel C, Wein b er g RA. Can cer st em cells an d ep it h
elial-m esenchyelial-m al t ransit ion: concept s and elial-m olecular links. Seelial-m in Cancer
Biol. 2012; 22( 5- 6) : 396- 403.
39- Singh SK, Clarke I D, Terasaki M, Bonn VE, Haw kins C, Squire J, et
DO,GHQWL¿FDWLRQRIDFDQFHUVWHPFHOOLQKXPDQEUDLQWXPRUV&DQFHU
Res. 2003; 63( 18) : 5821- 8.
40- Sm it h BN, Bhow m ick NA. Role of EMT in m et ast asis and t herapy
resist ance. J Clin Med. 2016; 5( 2) .
41- Spencer KR, Fer guson JW, Wiesenfeld D. Cur r ent concept s in
t h e m an agem en t of or al squ am ou s cell car cin om a. Au st Den t J.
2002; 47( 4) : 284- 9.
42- St em m ler MP. Cadherins in developm ent and cancer. Mol Biosyst .
2008; 4( 8) : 835- 50.
4 3 - Wo o l g ar JA. Hi st o p at h o l o g i cal p r o g n o st i cat o r s i n o r al an d
oropharyngeal squam ous cell carcinom a. Oral Oncol. 2006; 42( 3) :
229-39.
44- Yan Y, Zuo X, Wei D. Concise review : em erging role of CD44 in
cancer st em cells: a prom ising biom arker and t herapeut ic t arget . St em
Cells Transl Med. 2015; 4( 9) : 1033- 43.
45- Zeisberg M, Neilson EG. Biom arkers for epit helial- m esenchym al
t ransit ions. J Clin I nvest . 2009; 119( 6) : 1429- 37.
46- Zhang Z, Filho MS, Nör JE. The biology of head and neck cancer